Singapore Med J 2021; 62(12): 653-658 doi: 10.11622/smedj.2020079
Clinical depression among patients after acute coronary syndrome: a prospective single-tertiary centre analysis
Lai Kuan Leong1, MBBS, MMed, Ahmad Syadi Mahmood Zuhdi1, MBBCh, MMed, Muhammad Imran Abdul Hafidz1, MBChB, MRCP
Author Information >Copyright and License information >
1Department of Cardiology, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia Correspondence: Dr Leong Lai Kuan, Registrar, Department of Cardiology, Faculty of Medicine, University of Malaya, 50603 Kuala Lumpur, Malaysia. leonglk@ummc.edu.my
Clinical depression is a known consequence of acute coronary syndrome (ACS) and is associated with an adverse outcome among these patients, although this is often under-recognised. Through this study, we investigated the incidence of depression in post-ACS patients and its associated factors.
METHODS
We conducted a prospective cohort study in 95 patients with ACS admitted to University Malaya Medical Centre, Malaysia. Clinical depression was assessed during the index admission and at 30 days after discharge, using the Patient Health Questionnaire-9 (PHQ-9). Data was analysed using IBM SPSS Statistics, and binary logistic regression was used to determine the independent factors associated with depression, after adjusting for significant demographic variables and clinical characteristics. The strength of this association was presented as odds ratio and 95% confidence interval, and the significance level was set at 0.05.
RESULTS
The mean age of the study population was about 60 years, and 72.6% of the patients were male. Symptoms of depression were present in 88.4% of the patients at baseline. Depression at 30 days was more likely in female patients, patients with diabetes mellitus and patients on dialysis (p = 0.024, p < 0.001, p = 0.008, respectively). Patients with baseline moderate to severe depression were more likely to have moderate to severe depression at 30 days (p < 0.001). Baseline depression was the strongest predictor of depression at 30 days. An increment of one unit in PHQ-9 baseline score increased the risk of developing severe depression at 30 days by 31%.
CONCLUSION
Depression was prevalent in our post-ACS patients. The associated factors were female gender, diabetes mellitus and dialysis treatment.
Cardiovascular disease is the leading cause of death worldwide. Out of all global deaths in 2016, an estimated 17.9 million (31%) occurred from cardiovascular disease.(1) Patients with coronary artery disease (CAD) may present with acute coronary syndrome (ACS) or stable angina. ACS includes conditions such as ST-elevation myocardial infarction, non-ST-elevation myocardial infarction and unstable angina. Cardiomyocyte necrosis is observed in non-ST-elevation myocardial infarction, while myocardial ischaemia without cell loss is observed in unstable angina.(2)
Depression is prevalent among patients with cardiovascular disease. It affects about 20% of patients with CAD(3) and has a significant negative impact on various outcomes in patients with cardiovascular disease. The association between ACS and depression has been extensively reported and studied. This relationship is bidirectional – cardiovascular disease has been shown to increase the risk of depression, while depression is found to be associated with higher rates of cardiovascular mortality and morbidity.(4) The presence of depression in patients with coronary disease has been linked to lower rates of compliance with treatment and lifestyle modification; it is, thus, important to detect depression among patients in this group.(5) However, recent data from the American College of Cardiology suggests no benefit of detecting depression in these patients.(6)
Following an ACS event, patients often experience psychological stress. This may account for the prevalence of depression in this patient group.(7) However, depression is frequently under-recognised in patients with cardiac disease. Untreated depression can have a significant impact on the patient’s quality of life and increase the burden on family members.(8) Patients with CAD who experience depression show elevated levels of cytokines and interleukin. Inflammatory cytokines cause atherosclerotic plaques to become unstable and subsequently rupture, resulting in thrombosis.(9)
Owing to the negative impact of depression on patient outcomes, professional societies have recommended screening for depression in patients with coronary heart disease and appropriate referral to specialty care.(10) Early treatment and intervention in patients with cardiac disease are crucial to prevent untoward cardiovascular outcomes. The current study investigated the incidence and effect of depression among patients admitted with ACS, to explore whether the effects reported in other studies were observed in our patient population.
METHODS
A prospective study was conducted involving all patients diagnosed with ACS who were admitted to the cardiology ward of University Malaya Medical Centre, Malaysia, from July 2017 to February 2019. Both male and female patients aged > 18 years who presented with a diagnosis of ST-elevation myocardial infarction, non-ST-elevation myocardial infarction or unstable angina and who were able to complete the validated English or Bahasa Melayu Patient Health Questionnaire-9 (PHQ-9) were included. Patients who presented with Type 2 myocardial infarction or heart failure, and those who had underlying depression or had previously been admitted for psychiatric illness were excluded. Patients with ACS who met the inclusion criteria were selected using the consecutive sampling technique.
The statistical power of the study was determined using the OpenEpi software (www.openepi.com). Based on our calculation, a sample size of 68 was required to provide 80% power to estimate an odds ratio of 10 for having depression at 30 days after discharge, with 95% confidence.(11) Considering a potential loss to follow-up of 20%, we required at least 82 participants at the baseline of the study.
Data was collected using the PHQ-9, a diagnostic tool for assessing depression that is easy to administer and has good sensitivity and specificity. There were two sets of questionnaires – an English version and a validated Bahasa Melayu version. The questionnaire was answered by participants in a face-to-face interview during the index admission and via a telephone call at 30 days after discharge.(12) To avoid bias, only one interviewer administered the questionnaire. Data was collected by a designated medical officer, and a pilot study was performed in five patients. The dependent variable was depression at baseline and at 30 days after discharge.
The PHQ assesses eight diagnoses, divided into threshold disorders and subthreshold disorders. Threshold disorders are those that correspond to specific diagnoses in the Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM-IV): major depressive disorder, panic disorder, other anxiety disorder and bulimia nervosa. The PHQ-9 is the nine-item depression module from the full PHQ,(13) and the questions are based on the diagnostic criteria for depression from the DSM-IV.
For the current study, the PHQ-9 sought information about the patient’s experience in the past two weeks. Major depression was defined as the presence of five or more of the nine depressive symptom criteria at least ‘more than half the days’ in the past two weeks, with one of the symptoms being depressed mood or anhedonia. The nine questions from the PHQ-9 were scored using a scale of 0 to 3: not at all (score: 0), several days (score: 1), more than half the days (score: 2) and nearly every day (score: 3). The total PHQ-9 score ranged from 0 to 27, and depression was classified as: none to minimal (score: 0–4), mild (score: 5–9), moderate (score: 10–14), moderately severe (score: 15–19) and severe (score: 20–27).(13) Depression scores were dichotomised into two groups: none to mild depression (PHQ-9 < 10) and moderate to severe depression (PHQ-9 ≥ 10). For regression analysis, patients who scored < 10 were coded as ‘1’ and those who scored ≥ 10 were coded as ‘2’. In this study, we used a cut-off score of ≥ 10. This cut-off score was found to be optimal for maximising sensitivity without the loss of specificity.(13)
The independent variables were sociodemographic characteristics (age, gender, ethnicity) and clinical characteristics (cardiovascular risks, smoking history, premorbid condition and diagnosis of ACS). Data was cleaned, coded and analysed using IBM SPSS Statistics version 24.0 (IBM Corp, Armonk, NY, USA). Crude odds ratios with 95% confidence interval were estimated using binary logistic regression analysis to assess the association between each independent variable and the outcome variable. Variables with a value < 0.25 in the bivariable logistic regression analysis were considered in the multivariable logistic regression analysis.(14) Adjusted odds ratios with 95% confidence interval were estimated to assess the strength of the association, and variables with a p-value < 0.05 were considered significant factors.
RESULTS
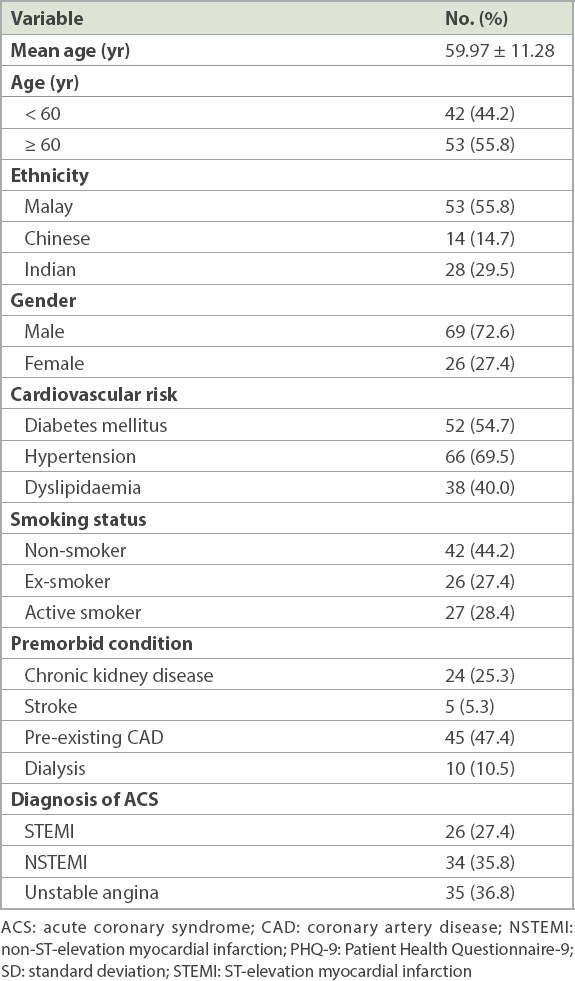
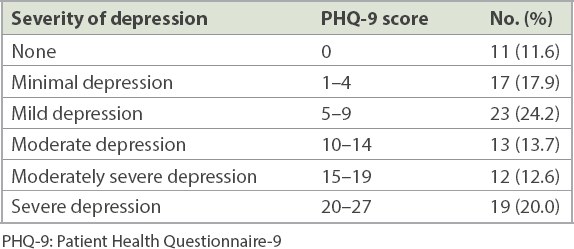
Of the 139 recruited patients, 95 met the inclusion criteria. Seven patients were lost to follow-up and seven patients died during the course of the study, leaving 81 patients for the PHQ-9 reassessment at 30 days after discharge. The mean age of the patients was 59.97 ± 11.28 (range 25–80) years. Patients were predominantly male (72.6%) and Malay (55.8%). The majority had hypertension and were non-smokers. Their cardiovascular risks were similar to those listed in the National Cardiovascular Disease Database Malaysia. Participants were distributed equally among the three subgroups of ACS (Table I). Following an ACS event, at least 88.4% of patients reported depression, with 46.3% of them having moderate to severe depression (Table II).
Table I
Sociodemographic and clinical characteristics of recruited patients (n = 95).
Table II
Prevalence of depression in post-acute coronary syndrome patients on admission (n = 95).
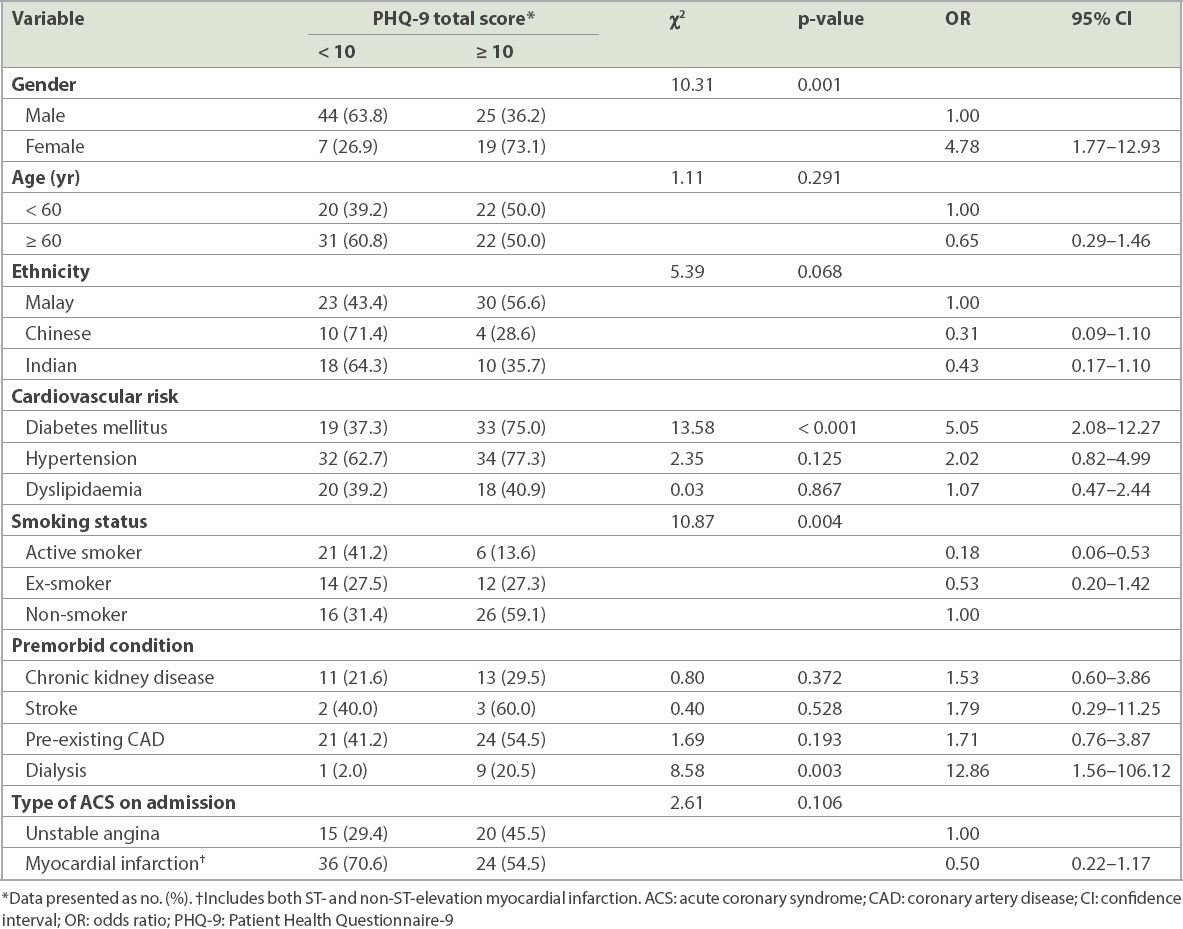
Univariate analysis showed differences in characteristics between patients with and without depression. Using male gender as the reference group, female patients had a four-fold increased risk of having depression. In terms of ethnicity, Malays had a higher rate of depression, although this was not statistically significant. Patients with diabetes mellitus had a five-fold increased risk of developing depression. An association between smoking status and the odds of depression was also observed; at baseline, active smokers were 82% less likely to develop depression compared with non-smokers. In addition, patients undergoing dialysis were found to have significant depression. However, no significant relationship was observed between chronic kidney disease/stroke/dyslipidaemia and depression at baseline, and between the subgroups of ACS and depression at baseline (Table III).
Table III
Univariate analysis of depression with sociodemographic and clinical characteristics on admission (n = 95).
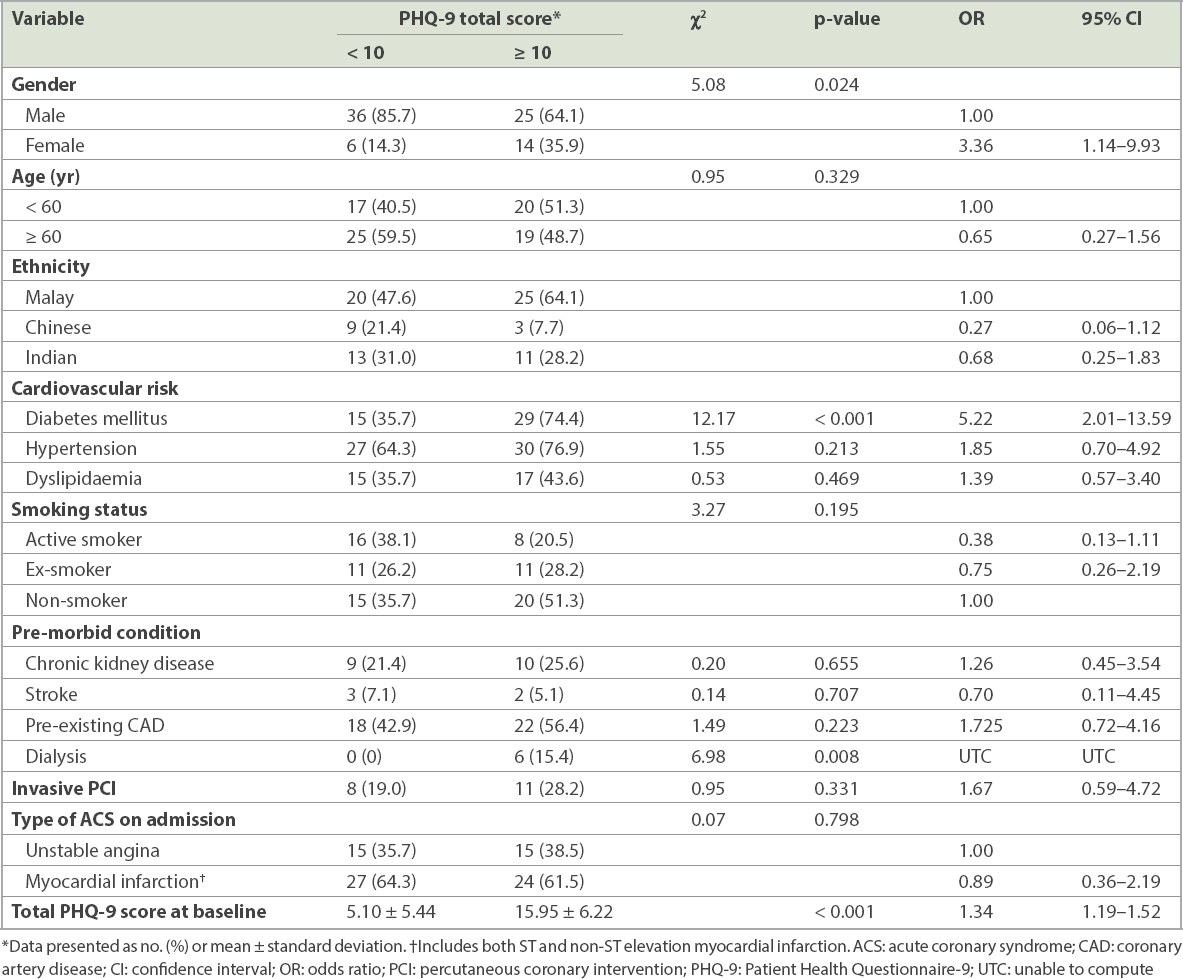
At 30 days after discharge, female patients had a three-fold increased risk of developing depression. Patients with diabetes mellitus and those undergoing dialysis also had increased odds of having depression. Patients who had moderate to severe depression (PHQ-9 score ≥ 10) at 30 days after discharge had a significantly higher baseline PHQ-9 score compared with those with none to mild depression at 30 days after discharge. In the moderate to severe depression group, an additional increase in one unit of PHQ-9 score from the baseline would lead to 34% increased odds of developing worsening depression at 30 days after discharge (Table IV).
Table IV
Univariate analysis of depression at 30 days after discharge with sociodemographic/clinical characteristics and baseline PHQ-9 scores (n = 95).
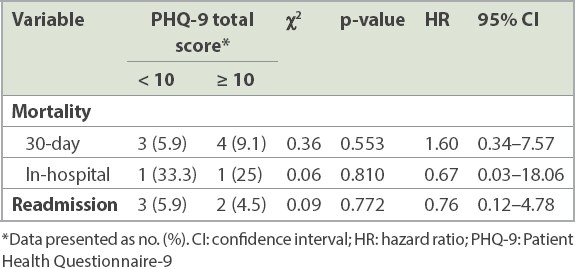
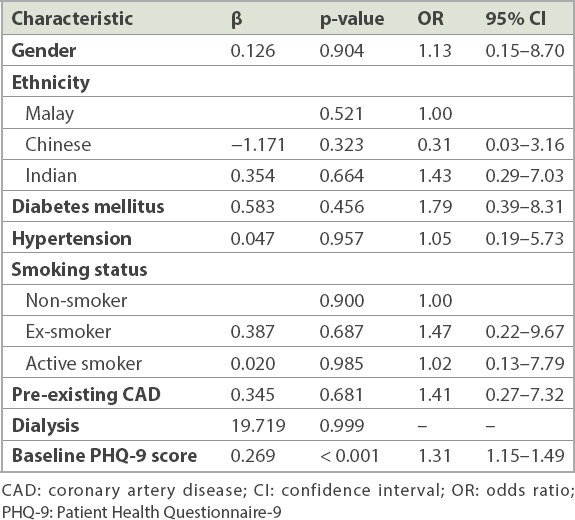
There was no significant difference in mortality outcome between the group of patients with none to mild depression (PHQ-9 < 10) and the group with moderate to severe depression (PHQ-9 ≥ 10). The severity of depression did not change the in-hospital and 30-day mortality outcomes of patients, and it had no influence on readmission rates (Table V). After controlling for all covariates, baseline depression remained the strongest predictor of depression at 30-day follow-up, with an increase in PHQ-9 score of one unit raising the odds of depression by 31% (Table VI).
Table V
Univariate analysis of depression with clinical characteristics and mortality outcome (in-hospital and 30-day all-cause mortality rates).
Table VI
Multivariate logistic regression of clinical predictors of depression 30 days after discharge.
DISCUSSION
The association between depression and cardiovascular morbidity and mortality has been explored for many years.(5) Several meta-analyses have summarised the findings as a bidirectional association, whereby the presence of depression is an independent risk factor for CAD and vice versa.(15) The presence of depression was shown to confer a negative prognosis in patients with CAD.(16) The mechanism of how depression affects the outcome has been described on many levels, and these include the behavioural, hormonal and endothelial aspects.(17-19) Depression is more likely to be associated with poor lifestyle modifications and lower compliance with therapies. On a more cellular level, various theories such as endothelial stress and platelet activation have been explored.(20)
The current study found that female patients with cardiac disorders were four times more likely to have at least moderate depression during the index admission compared with male patients. This female preponderance has also been reported in other studies.(21) A meta-analysis has shown that the prevalence of major depression in female patients with CAD is higher than that in male patients.(22) It has also been reported that the incidence of depression is two times greater in women than in men.(23) Postulated explanations for gender differences include psychosocial factors (e.g. role overload) and biological factors (e.g. hormones).(22) One study found that women more often present with internalising symptoms, whereas men present with externalising symptoms.(24) Women who are depressed have also been found to have poorer outcomes than depressed men do.(25) Having less social support as compared to men and an older average age of event in women have been put forward as the causes.
The association between diabetes mellitus and depression is bidirectional.(26) Studies have also shown that overweight and obesity are associated with depression. These patients have an approximately 40% higher risk of developing Type 2 diabetes mellitus.(27) Diabetes mellitus has a considerable impact on patients’ quality of life, with possible limitations in physical activities, family relations, social life and leisure activities. Thus, diabetics have an increased risk of developing depression.(28) A meta-analysis reported an 11% prevalence of major depression among patients with diabetes mellitus.(29)
Depression is also common in patients with end-stage renal failure. Patients undergoing dialysis experience a wide range of somatic symptoms and have significantly less involvement in occupational, social and recreational activities. The combination of psychological distress and disturbing physical symptoms results in significantly reduced quality of life, contributing to the development of depression.(30)
In our study, patients who were active smokers at baseline had 82% lower odds of developing significant depression. This might be attributable to smoking being a coping mechanism. Following a cigarette puff, nicotine enters the cerebral circulation and binds to the neuronal nicotinic acetylcholine receptors.(31) Hence, nicotine stimulates dopamine receptors in the brain, causing patients to feel less depressed. However, at 30 days after discharge, smoking was no longer associated with less depression. It is possible that active smokers might have quit smoking after they were discharged from the hospital.
Patients who had significant baseline depression were found to have an increased risk of developing significant depression at 30 days after discharge. However, depression in our patients with ACS was not significantly associated with an increase in in-hospital or out-of-hospital mortality and morbidity. Similarly, no increase in readmission rates was observed. Our findings contrasted with those of other studies,(32-34) which have shown positive associations between depression and all these factors. Our follow-up period was only 30 days compared with most studies, which showed a mortality difference at six months.(35,36) Despite these differences, we feel that this study should be treated as a pilot to a larger study with a longer follow-up duration. This will allow us to ascertain whether depression is a negative prognostic factor in our population. Larger or definitive studies will also enable us to determine whether screening for depression will help our population, like it has in Western practice.
This study has some limitations. An important confounding factor that may limit the generalisability of our study findings was the exclusion of patients with language barriers, namely patients who were unable to read or write English and Malay. Communication problems faced by patients have been found to be a barrier to seeking and accessing mental health services, which could subsequently affect the outcomes that are measured.(37,38) Additionally, the mean age of our patients was lower (60 years) compared to that of patients in developed countries (63.4–68.0 years). However, as the mean age of our cohort was comparable to that of patients with ACS (55.9–59.1 years) in Malaysia (based on the Malaysian National Cardiovascular Disease Database), we opine that this would have little impact on generalisability.(39) Another limitation of the study was its small sample size, resulting in possible selection bias. Also, we recognise that factors such as socioeconomic status, social support, alcohol intake and substance abuse are important confounders that may have an impact on depression;(34) unfortunately, these factors were not explored in our study.
In conclusion, depression was prevalent in our cohort of post-ACS patients. Factors associated with the presence of depression were female gender, diabetes mellitus and dialysis treatment. In addition, we found that severity of depression had no impact on in-hospital and 30-day outcomes in our cohort. Most of our results did not reach statistical significance, possibly owing to the short duration of follow-up. Hence, our findings should be replicated in a larger study with a longer follow-up period, to guide future screening for depression in patients with ACS.
References World Health OrganizationCardiovascular diseases (CVDs). Available at: www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds). Accessed April 22, 2019. Roffi M, Patrono C, Collet JP, et al. ESC Scientific Document Group2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation:Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC).Eur Heart J. 2016;37:267-315. Whooley MA.Depression and cardiovascular disease:healing the broken-hearted.JAMA. 2006;295:2874-81. Vaccarino V, Badimon L, Bremner JD, et al. ESC Scientific Document Group ReviewersDepression and coronary heart disease:2018 ESC position paper of the working group of coronary pathophysiology and microcirculation developed under the auspices of the ESC Committee for Practice Guidelines.Eur Heart J. 2020;41:1687-96. Gehi A, Haas D, Pipkin S, Whooley MA.Depression and medication adherence in outpatients with coronary heart disease:findings from the Heart and Soul Study.Arch Intern Med. 2005;165:2508-13. American College of CardiologyCODIACS-QoL:depression screening does not improve quality of life after ACS. Available at: www.acc.org/latest-in-cardiology/articles/2019/03/08/15/32/sat-1215pm-codiacs-qol-depression-screening-acs-acc-2019. Accessed April 20, 2019. Carney RM, Freedland KE.Depression in patients with coronary heart disease.Am J Med. 2008;121:11 Suppl 2S20-7. Huffman JC, Celano CM, Beach SR, Motiwala SR, Januzzi JL.Depression and cardiac disease:epidemiology, mechanisms, and diagnosis.Cardiovasc Psychiatry Neurol. 2013;2013:695925. Howren MB, Lamkin DM, Suls J.Associations of depression with C-reactive protein, IL-1, and IL-6:a meta-analysis.Psychosom Med. 2009;71:171-86. Lichtman JH, Bigger JT, JrBlumenthal JA, et al. Depression and coronary heart disease:recommendations for screening, referral, and treatment:a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research:endorsed by the American Psychiatric Association.Circulation. 2008;118:1768-75. Michael AJ, Krishnaswamy S, Muthusamy TS, Yusuf K, Mohamed J.Anxiety, depression and psychosocial stress in patients with cardiac events.Malays J Med Sci. 2005;12:57-63. Pinto-Meza A, Serrano-Blanco A, Peñarrubia MT, Blanco E, Haro JM.Assessing depression in primary care with the PHQ-9:Can it be carried out over the telephone?.J Gen Intern Med. 2005;20:738-42. Kroenke K, Spitzer RL, Williams JB.The PHQ-9:validity of a brief depression severity measure.J Gen Intern Med. 2001;16:606-13. Mickey RM, Greenland S.The impact of confounder selection criteria on effect estimation.Am J Epidemiol. 1989;129:125-37. Nicholson A, Kuper H, Hemingway H.Depression as an aetiologic and prognostic factor in coronary heart disease:a meta-analysis of 6362 events among 146,538 participants in 54 observational studies.Eur Heart J. 2006;27:2763-74. de Jonge P, van den Brink RH, Spijkerman TA, Ormel J.Only incident depressive episodes after myocardial infarction are associated with new cardiovascular events.J Am Coll Cardiol. 2006;48:2204-8. Weber B, Lewicka S, Deuschle M, et al. Increased diurnal plasma concentrations of cortisone in depressed patients.J Clin Endocrinol Metab. 2000;85:1133-6. Froger N, Palazzo E, Boni C, et al. Neurochemical and behavioral alterations in glucocorticoid receptor-impaired transgenic mice after chronic mild stress.J Neurosci. 2004;24:2787-96. Sherwood A, Hinderliter AL, Watkins LL, Waugh RA, Blumenthal JA.Impaired endothelial function in coronary heart disease patients with depressive symptomatology.J Am Coll Cardiol. 2005;46:656-9. Laghrissi-Thode F, Wagner WR, Pollock BG, Johnson PC, Finkel MS.Elevated platelet factor 4 and beta-thromboglobulin plasma levels in depressed patients with ischemic heart disease.Biol Psychiatry. 1997;42:290-5. Mallik S, Spertus JA, Reid KJ, et al. PREMIER Registry InvestigatorsDepressive symptoms after acute myocardial infarction:evidence for highest rates in younger women.Arch Intern Med. 2006;166:876-83. Shanmugasegaram S, Russell KL, Kovacs AH, Stewart DE, Grace SL.Gender and sex differences in prevalence of major depression in coronary artery disease patients:a meta-analysis.Matatas. 2012;73:305-11. Nolen-Hoeksema S, Larson J, Grayson C.Explaining the gender difference in depressive symptoms.J Pers Soc Psychol. 1999;77:1061-72. Albert PR.Why is depression more prevalent in women?.J Psychiatry Neurosci. 2015;40:219-21. Shah AJ, Ghasemzadeh N, Zaragoza-Macias E, et al. Sex and age differences in the association of depression with obstructive coronary artery disease and adverse cardiovascular events.J Am Heart Assoc. 2014;3:e000741. Pan A, Lucas M, Sun Q, et al. Bidirectional association between depression and type 2 diabetes mellitus in women.Arch Intern Med. 2010;170:1884-91. Arroyo C, Hu FB, Ryan LM, et al. Depressive symptoms and risk of type 2 diabetes in women.Diabetes Care. 2004;27:129-33. Eren I, Erdi O, Sahin M.The effect of depression on quality of life of patients with type II diabetes mellitus.Depress Anxiety. 2008;25:98-106. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ.The prevalence of comorbid depression in adults with diabetes:a meta-analysis.Diabetes Care. 2001;24:1069-78. King-Wing Ma T, Kam-Tao Li P.Depression in dialysis patients.Nephrology (Carlton). 2016;21:639-46. Herman AI, DeVito EE, Jensen KP, Sofuoglu M.Pharmacogenetics of nicotine addiction:role of dopamine.Pharmacogenomics. 2014;15:221-34. Lichtman JH, Froelicher ES, Blumenthal JA, et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome:systematic review and recommendations:a scientific statement from the American Heart Association.Circulation. 2014;129:1350-69. Barth J, Schumacher M, Herrmann-Lingen C.Depression as a risk factor for mortality in patients with coronary heart disease:a meta-analysis.Psychosom Med. 2004;66:802-13. Figueiredo JHC, Silva N, Pereira BB, Oliveira GMM.Major depression and acute coronary syndrome-related factors.Arq Bras Cardiol. 2017;108:217-27. Eagle KA, Lim MJ, Dabbous OH, et al. A validated prediction model for all forms of acute coronary syndrome:estimating the risk of 6-month postdischarge death in an international registry.JAMA. 2004;291:2727-33. Fox KA, Dabbous OH, Goldberg RJ, et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome:prospective multinational observational study (GRACE).BMJ. 2006;333:1091. Havranek EP, Mujahid MS, Barr DA, et al. Social determinants of risk and outcomes for cardiovascular disease:a scientific statement from the American Heart Association.Circulation. 2015;132:873-98. Sambrook Smith M, Lawrence V, Sadler E, Easter A.Barriers to accessing mental health services for women with perinatal mental illness:systematic review and meta-synthesis of qualitative studies in the UK.BMJ Open. 2019;9:e024803. Lu HT, Nordin RB.Ethnic differences in the occurrence of acute coronary syndrome:results of the Malaysian National Cardiovascular Disease (NCVD) Database Registry (March 2006 –February 2010).BMC Cardiovasc Disord. 2013;13:97.
2. Roffi M, Patrono C, Collet JP, et al; ESC Scientific Document Group. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2016; 37:267-315. https://doi.org/10.1093/eurheartj/ehv320
PMid:26320110
3. Whooley MA. Depression and cardiovascular disease: healing the broken-hearted. JAMA 2006; 295:2874-81. https://doi.org/10.1001/jama.295.24.2874
PMid:16804154 PMCid:PMC2771193
4. Vaccarino V, Badimon L, Bremner JD, et al; ESC Scientific Document Group Reviewers. Depression and coronary heart disease: 2018 ESC position paper of the working group of coronary pathophysiology and microcirculation developed under the auspices of the ESC Committee for Practice Guidelines. Eur Heart J 2020; 41:1687-96. https://doi.org/10.1093/eurheartj/ehy913
PMid:30698764
5. Gehi A, Haas D, Pipkin S, Whooley MA. Depression and medication adherence in outpatients with coronary heart disease: findings from the Heart and Soul Study. Arch Intern Med 2005; 165:2508-13. https://doi.org/10.1001/archinte.165.21.2508
PMid:16314548 PMCid:PMC2776695
7. Carney RM, Freedland KE. Depression in patients with coronary heart disease. Am J Med 2008; 121(11 Suppl 2):S20-7. https://doi.org/10.1016/j.amjmed.2008.09.010
PMid:18954589
8. Huffman JC, Celano CM, Beach SR, Motiwala SR, Januzzi JL. Depression and cardiac disease: epidemiology, mechanisms, and diagnosis. Cardiovasc Psychiatry Neurol 2013; 2013:695925. https://doi.org/10.1155/2013/695925
PMid:23653854 PMCid:PMC3638710
9. Howren MB, Lamkin DM, Suls J. Associations of depression with C-reactive protein, IL-1, and IL-6: a meta-analysis. Psychosom Med 2009; 71:171-86. https://doi.org/10.1097/PSY.0b013e3181907c1b
PMid:19188531
10. Lichtman JH, Bigger JT Jr, Blumenthal JA, et al. Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Psychiatric Association. Circulation 2008; 118:1768-75. https://doi.org/10.1161/CIRCULATIONAHA.108.190769
PMid:18824640
11. Michael AJ, Krishnaswamy S, Muthusamy TS, Yusuf K, Mohamed J. Anxiety, depression and psychosocial stress in patients with cardiac events. Malays J Med Sci 2005; 12:57-63.
12. Pinto-Meza A, Serrano-Blanco A, Peñarrubia MT, Blanco E, Haro JM. Assessing depression in primary care with the PHQ-9: Can it be carried out over the telephone? J Gen Intern Med 2005; 20:738-42. https://doi.org/10.1111/j.1525-1497.2005.0144.x
PMid:16050884 PMCid:PMC1490180
13. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001; 16:606-13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
PMid:11556941 PMCid:PMC1495268
15. Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146,538 participants in 54 observational studies. Eur Heart J 2006; 27:2763-74. https://doi.org/10.1093/eurheartj/ehl338
PMid:17082208
16. de Jonge P, van den Brink RH, Spijkerman TA, Ormel J. Only incident depressive episodes after myocardial infarction are associated with new cardiovascular events. J Am Coll Cardiol 2006; 48:2204-8. https://doi.org/10.1016/j.jacc.2006.06.077
PMid:17161246
17. Weber B, Lewicka S, Deuschle M, et al. Increased diurnal plasma concentrations of cortisone in depressed patients. J Clin Endocrinol Metab 2000; 85:1133-6. https://doi.org/10.1210/jcem.85.3.6469
PMid:10720051
18. Froger N, Palazzo E, Boni C, et al. Neurochemical and behavioral alterations in glucocorticoid receptor-impaired transgenic mice after chronic mild stress. J Neurosci 2004; 24:2787-96. https://doi.org/10.1523/JNEUROSCI.4132-03.2004
PMid:15028772 PMCid:PMC6729531
19. Sherwood A, Hinderliter AL, Watkins LL, Waugh RA, Blumenthal JA. Impaired endothelial function in coronary heart disease patients with depressive symptomatology. J Am Coll Cardiol 2005; 46:656-9. https://doi.org/10.1016/j.jacc.2005.05.041
PMid:16098431
20. Laghrissi-Thode F, Wagner WR, Pollock BG, Johnson PC, Finkel MS. Elevated platelet factor 4 and beta-thromboglobulin plasma levels in depressed patients with ischemic heart disease. Biol Psychiatry 1997; 42:290-5. https://doi.org/10.1016/S0006-3223(96)00345-9
21. Mallik S, Spertus JA, Reid KJ, et al; PREMIER Registry Investigators. Depressive symptoms after acute myocardial infarction: evidence for highest rates in younger women. Arch Intern Med 2006; 166:876-83. https://doi.org/10.1001/archinte.166.8.876
PMid:16636213
22. Shanmugasegaram S, Russell KL, Kovacs AH, Stewart DE, Grace SL. Gender and sex differences in prevalence of major depression in coronary artery disease patients: a meta-analysis. Maturitas 2012; 73:305-11. https://doi.org/10.1016/j.maturitas.2012.09.005
PMid:23026020 PMCid:PMC4490896
23. Nolen-Hoeksema S, Larson J, Grayson C. Explaining the gender difference in depressive symptoms. J Pers Soc Psychol 1999; 77:1061-72. https://doi.org/10.1037/0022-3514.77.5.1061
PMid:10573880
24. Albert PR. Why is depression more prevalent in women? J Psychiatry Neurosci 2015; 40:219-21. https://doi.org/10.1503/jpn.150205
PMid:26107348 PMCid:PMC4478054
25. Shah AJ, Ghasemzadeh N, Zaragoza-Macias E, et al. Sex and age differences in the association of depression with obstructive coronary artery disease and adverse cardiovascular events. J Am Heart Assoc 2014; 3:e000741. https://doi.org/10.1161/JAHA.113.000741
26. Pan A, Lucas M, Sun Q, et al. Bidirectional association between depression and type 2 diabetes mellitus in women. Arch Intern Med 2010; 170:1884-91. https://doi.org/10.1001/archinternmed.2010.356
PMid:21098346 PMCid:PMC3065781
27. Arroyo C, Hu FB, Ryan LM, et al. Depressive symptoms and risk of type 2 diabetes in women. Diabetes Care 2004; 27:129-33. https://doi.org/10.2337/diacare.27.1.129
PMid:14693978 PMCid:PMC4502913
28. Eren I, Erdi O, Sahin M. The effect of depression on quality of life of patients with type II diabetes mellitus. Depress Anxiety 2008; 25:98-106. https://doi.org/10.1002/da.20288
PMid:17311266
29. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2001; 24:1069-78. https://doi.org/10.2337/diacare.24.6.1069
PMid:11375373
30. King-Wing Ma T, Kam-Tao Li P. Depression in dialysis patients. Nephrology (Carlton) 2016; 21:639-46. https://doi.org/10.1111/nep.12742
PMid:26860073
31. Herman AI, DeVito EE, Jensen KP, Sofuoglu M. Pharmacogenetics of nicotine addiction: role of dopamine. Pharmacogenomics 2014; 15:221-34. https://doi.org/10.2217/pgs.13.246
PMid:24444411 PMCid:PMC4154357
32. Lichtman JH, Froelicher ES, Blumenthal JA, et al. Depression as a risk factor for poor prognosis among patients with acute coronary syndrome: systematic review and recommendations: a scientific statement from the American Heart Association. Circulation 2014; 129:1350-69. https://doi.org/10.1161/CIR.0000000000000019
PMid:24566200
33. Barth J, Schumacher M, Herrmann-Lingen C. Depression as a risk factor for mortality in patients with coronary heart disease: a meta-analysis. Psychosom Med 2004; 66:802-13. https://doi.org/10.1097/01.psy.0000146332.53619.b2
PMid:15564343
34. Figueiredo JHC, Silva N, Pereira BB, Oliveira GMM. Major depression and acute coronary syndrome-related factors. Arq Bras Cardiol 2017; 108:217-27. https://doi.org/10.5935/abc.20170028
PMid:28443957 PMCid:PMC5389871
35. Eagle KA, Lim MJ, Dabbous OH, et al. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. JAMA 2004; 291:2727-33. https://doi.org/10.1001/jama.291.22.2727
PMid:15187054
36. Fox KA, Dabbous OH, Goldberg RJ, et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). BMJ 2006; 333:1091. https://doi.org/10.1136/bmj.38985.646481.55
PMid:17032691 PMCid:PMC1661748
37. Havranek EP, Mujahid MS, Barr DA, et al. Social determinants of risk and outcomes for cardiovascular disease: a scientific statement from the American Heart Association. Circulation 2015; 132:873-98. https://doi.org/10.1161/CIR.0000000000000228
PMid:26240271
38. Sambrook Smith M, Lawrence V, Sadler E, Easter A. Barriers to accessing mental health services for women with perinatal mental illness: systematic review and meta-synthesis of qualitative studies in the UK. BMJ Open 2019; 9:e024803. https://doi.org/10.1136/bmjopen-2018-024803
PMid:30679296 PMCid:PMC6347898
39. Lu HT, Nordin RB. Ethnic differences in the occurrence of acute coronary syndrome: results of the Malaysian National Cardiovascular Disease (NCVD) Database Registry (March 2006 - February 2010). BMC Cardiovasc Disord 2013; 13:97. https://doi.org/10.1186/1471-2261-13-97
PMid:24195639 PMCid:PMC4229312