Singapore Med J 2021; 62(12): 636-641 doi: 10.11622/smedj.2021051
Clinicopathological patterns and survival outcomes of colorectal cancer among young adults in Malaysia: an institutional cohort study
Sui-Weng Wong1, MBBS, Dao-Yao Ling1, MBBS, Ri-Qi Yeow1, MBBS, Ro-Wan Chong1, MBBS, Mohamed Rezal Abdul Aziz1, MS, Nora Abdul Aziz1, MS, Keat-Seong Poh1, MS, April Camilla Roslani1, MS, FRCS
Author Information >Copyright and License information >
1Department of Surgery, University Malaya Medical Centre, Kuala Lumpur, Malaysia Correspondence: Prof Dr April Camilla Roslani, Senior Consultant Colorectal Surgeon, Department of Surgery, Faculty of Medicine, University of Malaya, Jalan Universiti, 50603 Kuala Lumpur, Federal Territory of Kuala Lumpur, Malaysia. april@ummc.edu.my
This study aimed to investigate the clinicopathological patterns and survival outcomes of patients with young-onset colorectal cancer (CRC) in Malaysia.
METHODS
A total of 206 patients with young-onset CRC (age < 50 years at diagnosis) and 1,715 patients with late-onset CRC (age ≥ 50 years at diagnosis) diagnosed during 2002–2016 were included. The clinicopathological characteristics of patients with young-onset CRC were compared with those of patients with late-onset CRC during 2009–2013. Kaplan-Meier survival analysis was performed to determine the overall survival (OS) and disease-specific survival (DSS) in these patients.
RESULTS
The overall proportion of young-onset CRC was 10.7%. The mean age for young-onset CRC was 39.5 ± 7.4 years, with a male-to-female ratio of 1.2:1. There were more Malay patients with young-onset CRC than late-onset CRC (44.0% vs. 19.9%, p = 0.004). Most CRCs were diagnosed at an advanced stage in both groups. However, young-onset CRC showed more aggressive tumour characteristics, such as poorer differentiation and mucinous subtype. Despite such differences, the OS and DSS in both groups were similar (five-year OS for young-onset CRC vs. late-onset CRC: 44.2% vs. 49.0%, p = 0.40; five-year DSS for young-onset CRC vs. late-onset CRC: 48.8% vs. 57.6%, p = 0.53; mean survival of young-onset CRC vs. late-onset CRC: 4.9 years vs. 5.4 years, p = 0.15). Advanced stage at diagnosis and the treatment modality used were independent prognostic factors.
CONCLUSION
The unique ethnic and histological differences between patients with young- and late-onset CRC suggest that young-onset CRC may represent a distinct entity. However, despite such differences, both groups were equivalent.
Keywords: colorectal cancer, Malaysia, prognosis, survival rates, young adults
INTRODUCTION
Colorectal cancer (CRC) is currently the second most common cancer in Malaysia.(1) The age-standardised rate for CRC in Malaysia is about 14.6 per 100,000 population – much lower than that in developed countries in Europe and Northern America, where the age-standardised rate is in excess of 40 per 100,000 population.(1,2) However, the incidence of CRC is rising, possibly owing to rapid socioeconomic development leading to increasing adoption of Western diets and lifestyles.(2-4) The incidence of CRC among young adults in the United States is also increasing sharply.(5-8)
Many studies have sought to determine whether young-onset CRC has any unique clinicopathological features, with conflicting results.(9-13) Thus, it remains unclear whether young-onset CRC represents a distinct entity. Several studies have reported more aggressive tumour characteristics for young-onset CRC.(14,15) At present, there is a paucity of literature on young-onset CRC within the Asia-Pacific region. Institutional studies have reported a variable proportion of young-onset CRC, ranging from 6.7% in Taiwan to 39% in India.(16-19)
To the best of our knowledge, there are no studies on CRC among young adults in Malaysia. Malaysia epitomises a multi-ethnic Asian population, consisting predominantly of Malay, Chinese and Indian people. Identifying disparities in the ethnic distribution of young- and late-onset CRC would help to elucidate the interplay between genetics and environmental factors, and could guide clinical management. Keeping in mind the long-term consequences of CRC in young adults, we conducted a retrospective study at our hospital to determine the clinicopathological patterns and survival outcomes of young-onset CRC in Malaysia.
METHODS
This retrospective study was conducted at the University Malaya Medical Centre, a tertiary hospital in Malaysia. Consecutive patients diagnosed with CRC between 2002 and 2016 were identified and patients with young-onset CRC were included in the study. Young-onset CRC was defined as CRC affecting patients aged less than 50 years, as per previous studies that have considered young-onset patients to be those of pre-screening age, with an upper limit of 39–49 years.(20)
The medical records of patients with young-onset CRC were reviewed and the following data was retrieved for each patient: demographics (e.g. age, gender and ethnicity); tumour characteristics (e.g. TNM staging, tumour site, tumour cellular differentiation, grading, lymphovascular invasion, perineural invasion and tumour-infiltrating lymph nodes) and clinical characteristics (e.g. symptoms, duration of symptoms, predisposing factors [e.g. inflammatory bowel disease, familial adenomatous polyposis, hereditary non-polyposis colorectal cancer and family history of CRC]); and treatment modality.
Separately, a control group consisting of 579 patients aged 50 years and above who were diagnosed with CRC during the period 2009–2013 was compared with 75 patients with young-onset CRC diagnosed during the same period. Patient characteristics and five-year survival outcomes between both groups were compared. The primary and secondary outcomes were five-year overall survival (OS) and five-year disease-specific survival (DSS).
The study was approved by the institutional ethics committee (MREC no. 2017615295).
Statistical analyses were performed using IBM SPSS Statistics version 24.0 (IBM Corp, Armonk, NY, USA). Quantitative variables were expressed as mean ± standard deviation, while categorical variables were expressed as number and percentage. Differences between categorical variables were examined using chi-square test, while differences between numerical variables were examined using t-test or analysis of variance, where appropriate. Kaplan-Meier survival analysis was used to calculate the OS and DSS rates. OS was calculated from the date of histological diagnosis of CRC to the date of death from any cause, and DSS involved the absence of death attributable to CRC. Potential prognostic factors were tested individually using the log-rank test and multivariate logistic regression analysis was conducted using the Cox proportional hazards model. The significance level was set at p < 0.05.
RESULTS
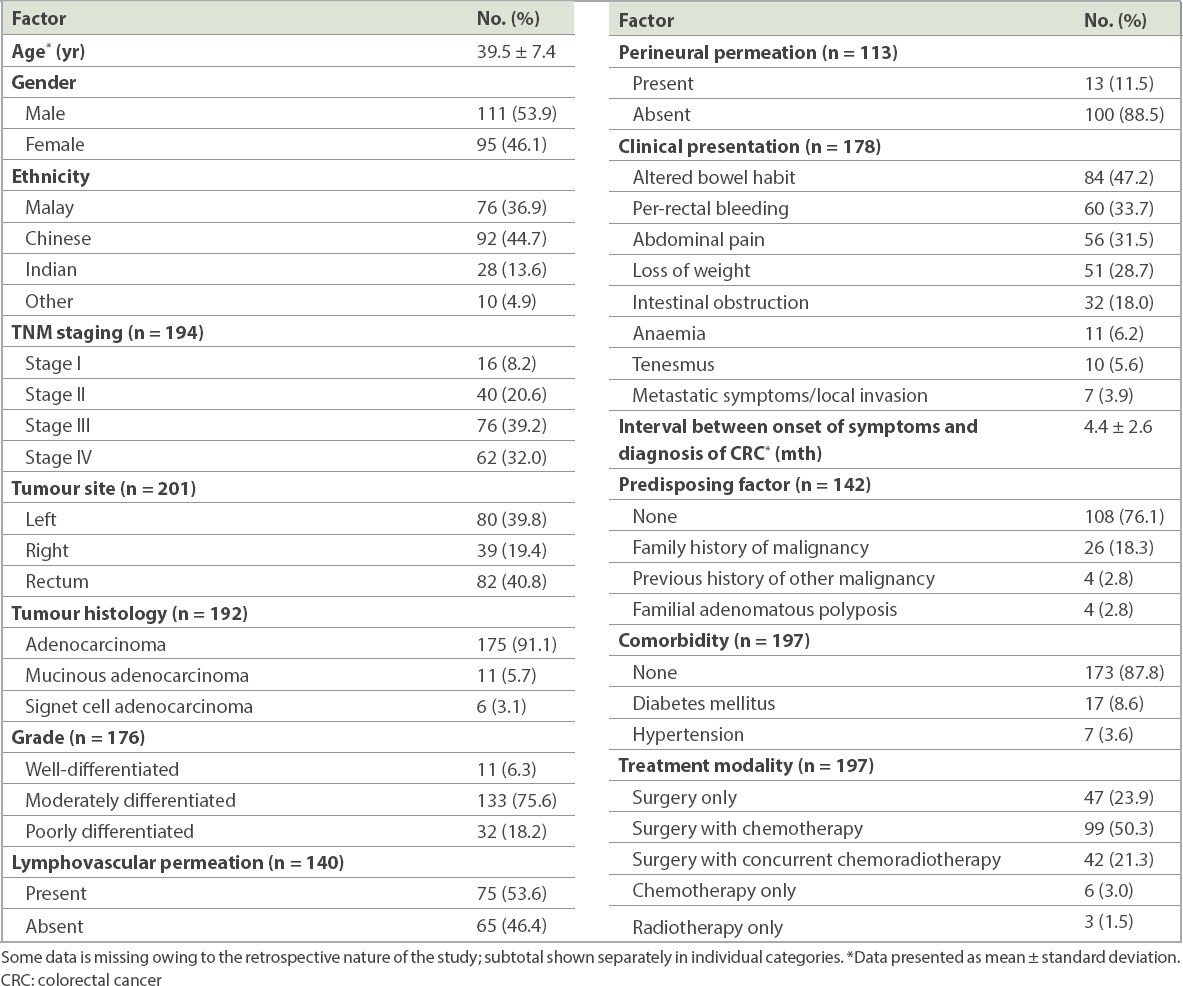
A total of 1,921 patients were diagnosed with CRC from 2002 to 2016, of which 206 patients had young-onset CRC. The overall frequency of young-onset CRC was 10.7%. The demographics and pathological characteristics of patients with young-onset CRC are shown in Table I. The mean age of patients with young-onset CRC was 39.5 ± 7.4 years, with a male-to-female ratio of 1.2:1. A majority of patients with young-onset CRC were diagnosed at an advanced stage (71.2%). Tumours were mostly left-sided (39.8%) or in the rectum (40.8%), and were predominantly adenocarcinoma (91.1%). Most tumours were moderately differentiated (75.6%), but among patients with very young-onset CRC (age < 30 years), tumours were more likely to be poorly differentiated (p = 0.003).
Table I
Demographic and pathological characteristics of patients with young-onset CRC (n = 206).
The two most common symptoms were altered bowel habit (47.2%) and per-rectal bleeding (33.7%). Intestinal obstruction was associated with left-sided tumour (p < 0.001), abdominal pain and anaemia were associated with right-sided tumour (p < 0.05), and per-rectal bleeding and tenesmus were associated with rectal tumour (p < 0.05). Surgery with chemotherapy was the most common treatment modality (50.3%) and was mainly used for advanced CRC (p < 0.001).
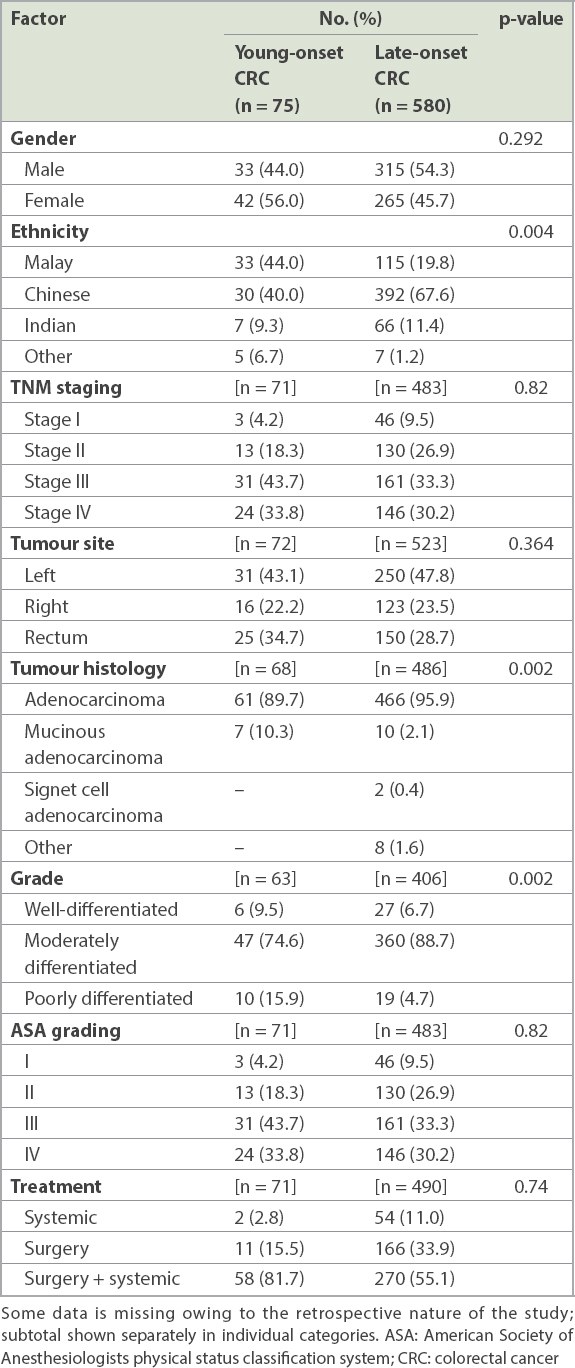
A comparison of patient characteristics among those with young- and late-onset CRC is shown in Table II. There were no significant differences between the genders. However, the ethnic composition between young- and late-onset CRC was markedly different. Young-onset CRC consisted of more Malay patients when compared with late-onset CRC (44.0% vs. 19.9%, p = 0.004). In both groups, CRC was diagnosed at the late stage and was primarily located in the left colon or rectum. Young-onset CRC was more likely to be mucinous adenocarcinoma and poorly differentiated histological subtypes (p < 0.01). Not unexpectedly, young-onset CRC had better premorbid function than late-onset CRC (p < 0.005). A majority (81.7%) of patients with young-onset CRC received combination therapy when compared to those with late-onset CRC (55.1%). However, this difference did not reach statistical significance.
Table II
Comparison of patients with young- and late-onset CRC from 2009 to 2013.
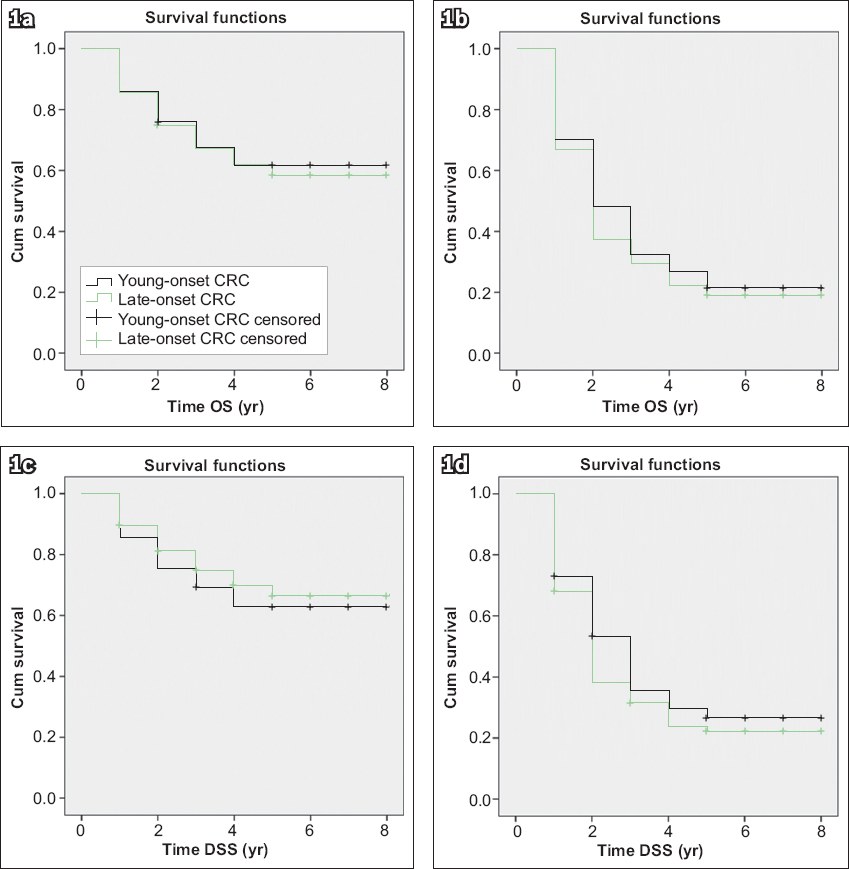
The OS and DSS rates are shown in Fig. 1. There was no statistically significant difference in the five-year OS (young-onset CRC vs. late-onset CRC: 44.2% vs. 49.0%, p = 0.40) and five-year DSS (young-onset CRC vs. late-onset CRC: 48.8% vs. 57.6%, p = 0.53; mean survival of young-onset CRC vs. late-onset CRC: 4.9 years vs. 5.4 years, p = 0.15) rates between the two groups. A sub-analysis comparing individual disease stages between age groups showed no statistically significant difference across all stages for OS and DSS.
Fig. 1
Kaplan-Meier graphs show (a) OS in Stages I–III; (b) OS in Stage IV; (c) DSS in Stages I–III; and (d) DSS in Stage IV CRC. CRC: colorectal cancer; DSS: disease-specific survival; OS: overall survival
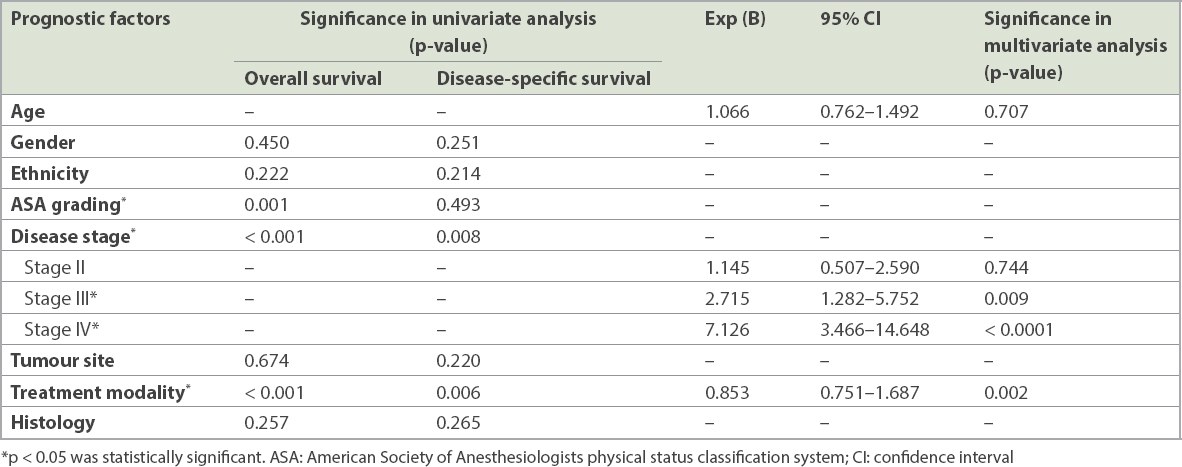
Univariate logistic regression analysis (Table III) showed that advanced stage, ASA grade and treatment modality were significantly associated with reduced OS and DSS. Age, gender, ethnicity, tumour site and histological subtype were not significantly associated with OS and DSS. Multivariate logistic regression analysis identified advanced stage and the treatment modality used as independent prognostic factors.
Table III
Univariate and multivariate logistic regression analyses of overall survival and disease-specific survival according to various factors.
DISCUSSION
The incidence of CRC among young adults is on the rise and has become a major public health concern.(8,21) However, data on this subpopulation, particularly within the Southeast Asia region, is scarce and conflicting. As a result, the approach towards young-onset CRC in Malaysia is largely guided by experience. Our study aimed to better define the clinicopathological characteristics of young-onset CRC, utilising two potential strengths: a hospital-based study, with more complete clinical information, and the multi-racial composition of Malaysia, in view of similar environmental exposure across all ethnicities.
In our study, young-onset CRC represented about 11% of all patients with CRC. The proportions of young-onset CRC in developing countries were noted to be higher than those in developed countries.(8-11,16,18,19,22,23) This puzzling difference may be due to lifestyle and dietary patterns that individuals are exposed to during their childhood and younger adulthood years, which were different from those of preceding generations.(24) In other words, in historically low-risk regions for CRC, where rates in the older population have remained low, CRC incidence has increased significantly in newer generations.(25) Even among developed countries, CRC among young adults is rising.(5,7,21,26) This can also be attributed to changes in lifestyle and environmental factors, with evidence of strong birth cohort effects on the incidence of CRC.(6,7) The rise in young-onset CRC parallels with the obesity epidemic, as obesity significantly increases the risk of developing CRC.(27,28) Moreover, complex epigenetic interactions between obesity, sedentary lifestyles and changes in dietary patterns, such as increased intake of fat with decreased intake of fibre, could also contribute to the rise in young-onset CRC.(27,29-32) Recently, alterations in the gut microbiome have been implicated in the causation of CRC.(33,34) Separately, diet and antibiotic use are also known to change the population of gut microbiome.(35-38) It would not be unreasonable to link all three factors to the increasing incidence of CRC in the younger cohort. Population-based studies would be helpful in further characterising national epidemiological trends with regard to young-onset CRC.
According to our National Cancer Registry data, individuals with Chinese ethnicity had the highest CRC incidence (27.35), followed by those with Malay (18.95) and Indian (17.55) ethnicities.(39) Other institutional studies in Malaysia have reported similar findings.(40,41) These ethnic differences could be attributed to genetic factors, as similar patterns were observed in Singapore and Brunei.(18,42) The disparity in the incidence between Chinese and Indians living in Southeast Asia mirrors the rates in the countries of origin, despite both groups having migrated more than three generations ago.(43) When we compared the ethnic composition between young- and late-onset CRC, there were markedly fewer Chinese and more Malay individuals in the younger group. Although the exact causation has not been identified, an increasingly Westernised lifestyle adopted by Malay people over recent years could have led to an increase in young-onset CRC.(44,45) However, it is unlikely that lifestyle factors alone could result in such differences, thus supporting the theory that young-onset CRC may represent a distinct entity.(46,47) This warrants further research to better understand the molecular differences between young- and late-onset CRC.
The clinicopathological characteristics described in this study are in keeping with the current understanding of young-onset CRC, which usually presents with altered bowel habit and per-rectal bleeding.(9-11,14) The diagnostic challenge here is to distinguish benign causes of per-rectal bleeding from malignant causes. It is challenging for clinicians to thoroughly investigate per-rectal bleeding among young adults owing to cost constraints in public hospitals. However, when per-rectal bleeding is associated with other symptoms, such as altered bowel habit, investigation for more sinister causes is warranted. It is also a common misconception that young-onset CRC is usually hereditary. In our study, only 18.3% of patients with young-onset CRC had a family history of cancer, which was lower than the average incidence of 22.8% reported in a review.(14) This suggests that in a majority of cases, young-onset CRC is sporadic, and the lack of suspicion in these individuals may lead to a delay in diagnosis, resulting in late presentation and poorer outcomes.(14,48) While most studies report that young-onset CRC is more often diagnosed at advanced stages when compared with late-onset CRC, late presentations occurred in both groups in our study.(10) Currently, there are no nationwide, population-based screening programmes for CRC in Malaysia.(49,50) Hence, public awareness on CRC and participation rate for opportunistic screening in Malaysia remained low.(51) Strategies to increase awareness of the symptoms of CRC among the general population along with implementation of screening programmes in Malaysia are necessary for early detection of CRC, which could lead to improved survival.
Nevertheless, late presentations only partially account for the poorer prognosis in young patients. Many studies have reported that patients with young-onset CRC tend to have poorer histological features.(9,10,12,52) Our findings, which show that young-onset CRC shows a trend towards mucinous adenocarcinoma subtype and poor differentiation with lymphovascular permeation, are consistent with this. However, there is no consensus that more aggressive histological subtypes are indicative of poorer prognosis, and we have shown similar survival outcomes for patients with young- and late-onset CRC.(9-11,14,53) The possible explanations are that more patients with young-onset CRC received combination therapy, hence compensating for worse tumour biology, or that younger patients had fewer comorbidities and better baseline life expectancy independent of the cancer diagnosis.(53) Treatment modality was pivotal in influencing OS and DSS for both young and old cohorts, where combination therapy (both systemic and surgery) was superior to monotherapy for achieving better survival outcomes. Our study showed a trend for more patients with young-onset CRC receiving combination therapy than those with late-onset CRC. However, this finding did not reach statistical significance, which could be attributed to Type II error owing to the limited sample size.
In view of the advanced presentation of CRC in both groups, we fully support efforts to establish nationwide CRC screening, as it has been shown to reduce incidence, particularly in high-prevalence countries. However, the costs and benefits of screening in Malaysia are unclear at this stage owing to its low yield compared to Western populations and limited resources.(54-56) Hence, in a resource-limited setting, guidance on identification of susceptible individuals and a tailored approach to screening modalities, through consensus or guideline-guided screening policies, are essential. Although the Malaysian clinical practice guidelines provide some guidance, this will need to be reviewed as new data emerges.(57)
There are several limitations to this study. Results drawn from a single-centre study may not reflect the entire Malaysian population, and the retrieval of patients’ data using the International Classification of Diseases coding system might have been subject to misclassification. Incomplete medical records also limited the completeness of the data. Moreover, we did not compare the differences in risk factors and socioeconomic determinants between patients with young- and late-onset CRC owing to incomplete data.
In conclusion, CRC in young adults is unique in terms of ethnic predilection and tumour biology, but age alone does not affect survival outcomes. Diagnosis at an early stage would improve survival, in general, among patients with CRC. However, a significant minority of patients in our study population had young-onset CRC. Hence, clinicians need to be suspicious when young adults present with altered bowel habit or per-rectal bleeding, even in the absence of predisposing factors.
References Azizah Ab M, Nor Saleha IT, Noor Hashimah A, Asmah ZA, Mastulu W.Malaysian National Cancer Registry Report 2007-2011.Malaysia cancer statistics, data and figure. National Cancer Institute, Ministry of Health Malaysia. Available at: https://www.crc.gov.my/wp-content/uploads/documents/report/MNCRRrepor2007-2011.pdf. Accessed August 1, 2019. Arnold M, Sierra MS, Laversanne M, et al. Global patterns and trends in colorectal cancer incidence and mortality.Gut. 2017;66:683-91. Center MM, Jemal A, Smith RA, Ward E.Worldwide variations in colorectal cancer.CA Cancer J Clin. 2009;59:366-78. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide:sources, methods and major patterns in GLOBOCAN 2012.Int J Cancer. 2015;136:E359-86. Siegel RL, Jemal A, Ward EM.Increase in incidence of colorectal cancer among young men and women in the United States.Cancer Epidemiol Biomarkers Prev. 2009;18:1695-8. Siegel RL, Fedewa SA, Anderson WF, et al. Colorectal cancer incidence patterns in the United States, 1974-2013.J Natl Cancer Inst. 2017;109:djw322. Singh KE, Taylor TH, Pan CJG, Stamos MJ, Zell JA.Colorectal cancer incidence among young adults in California.J Adolesc Young Adult Oncol. 2014;3:176-84. Bailey CE, Hu CY, You YN, et al. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975-2010.JAMA Surg. 2015;150:17-22. Ganapathi S, Kumar D, Katsoulas N, et al. Colorectal cancer in the young:trends, characteristics and outcome.Int J Colorectal Dis. 2011;26:927-34. Chou CL, Chang SC, Lin TC, et al. Differences in clinicopathological characteristics of colorectal cancer between younger and elderly patients:an analysis of 322 patients from a single institution.Am J Surg. 2011;202:574-82. Nagai Y, Hata K, Kawai K, et al. Clinicopathological features of colorectal cancer patients under the age of 50:recent experience and case-control study of prognosis in a Japanese cohort.Digestion. 2016;93:272-9. Goldvaser H, Pam O, Kundel Y, et al. Colorectal cancer in young patients:is it a distinct clinical entity?.Int J Clin Oncol. 2016;21:684-95. Liang JT, Huang KC, Cheng AL, et al. Clinicopathological and molecular biological features of colorectal cancer in patients less than 40 years of age.Br J Surg. 2003;90:205-14. O'Connell JB, Maggard MA, Livingston EH, Yo CK.Colorectal cancer in the young.Am J Surg. 2004;187:343-8. Inra JA, Syngal S.Colorectal cancer in young adults.Dig Dis Sci. 2015;60:722-33. Gupta S, Bhattacharya D, Acharya AN, et al. Colorectal carcinoma in young adults:a retrospective study on Indian patients: 2000-2008.Colorectal Dis. 2010;12:e182-9. Chiang JM, Chen MC, Changchien CR, et al. Favorable influence of age on tumor characteristics of sporadic colorectal adenocarcinoma:patients 30 years of age or younger may be a distinct patient group.Dis Colon Rectum. 2003;46:904-10. Koh KS, Telisinghe PU, Bickle I, et al. Characteristics of young colorectal cancer in Brunei Darussalam:an epidemiologic study of 29 years (1986-2014).Asian Pac J Cancer Prev. 2015;16:3279-83. Hav M, Eav S, Ky V, et al. Colorectal cancer in young Cambodians.Asian Pac J Cancer Prev. 2011;12:1001-5. Rho YS, Gilabert M, Polom K, et al. Comparing clinical characteristics and outcomes of young-onset and late-onset colorectal cancer:an international collaborative study.Clin Colorectal Cancer. 2017;16:334-42. O'Connell JB, Maggard MA, Liu JH, et al. Rates of colon and rectal cancers are increasing in young adults.Am Surg. 2003;69:866-72. Quach DT, Nguyen OT.Clinical, endoscopic and pathogical characteristics of early-onset colorectal cancer in Vietnamese.Asian Pac J Cancer Prev. 2012;13:1767-70. Park HC, Shin A, Kim BW, et al. Data on the characteristics and the survival of Korean patients with colorectal cancer from the Korea Central Cancer Registry.Ann Coloproctol. 2013;29:144-9. Ansari R, Mahdavinia M, Sadjadi A, et al. Incidence and age distribution of colorectal cancer in Iran:results of a population-based cancer registry.Cancer Lett. 2006;240:143-7. Bishehsari F, Mahdavinia M, Vacca M, Malekzadeh R, Mariani-Costantini R.Epidemiological transition of colorectal cancer in developing countries:environmental factors, molecular pathways, and opportunities for prevention.World J Gastroenterol. 2014;20:6055-72. Edwards BK, Ward E, Kohler BA, et al. Annual report to the nation on the status of cancer, 1975-2006, featang colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates.Cancer. 2010;116:544-73. Huxley RR, Ansary-Moghaddam A, Clifton P, et al. The impact of dietary and lifestyle risk factors on risk of colorectal cancer:a quantitative overview of the epidemiological evidence.Int J Cancer. 2009;125:171-80. Lee JM, Pilli S, Gebremariam A, et al. Getting heavier, younger:trajectories of obesity over the life course.Int J Obes (Lond). 2010;34:614-23. Aune D, Chan DSM, Lau R, et al. Dietary fibre, whole grains, and risk of colorectal cancer:systematic review and dose-response meta-analysis of prospective studies.BMJ. 2011;343:d6617. Nielsen SJ, Popkin BM.Patterns and trends in food portion sizes, 1977-1998.JAMA. 2003;289:450-3. Brownson RC, Boehmer TK, Luke DA.Declining rates of physical activity in the United States:what are the contributors?.Annu Rev Public Health. 2005;26:421-43. Ezzati M, Riboli E.Behavioral and dietary risk factors for noncommunicable diseases.N Engl J Med. 2013;369:954-64. Dejea CM, Wick EC, Hechenbleikner EM, et al. Microbiota organization is a distinct feature of proximal colorectal cancers.Proc Natl Acad Sci U S A. 2014;111:18321-6. Gagnière J, Raisch J, Veziant J, et al. Gut microbiota imbalance and colorectal cancer.World J Gastroenterol. 2016;22:501-18. Murphy EA, Velazquez KT, Herbert KM.Influence of high-fat diet on gut microbiota:a driving force for chronic disease risk.Curr Opin Clin Nutr Metab Care. 2015;18:515-20. Clarke SF, Murphy EF, Nilaweera K, et al. The gut microbiota and its relationship to diet and obesity:new insights.Gut Microbes. 2012;3:186-202. Modi SR, Collins JJ, Relman DA.Antibiotics and the gut microbiota.J Clin Invest. 2014;124:4212-8. Lange K, Buerger M, Stallmach A, Bruns T.Effects of antibiotics on gut microbiota.Dig Dis. 2016;34:260-8. Abu Hassan MR, Ismail I, Mohd Suan MA, et al. Incidence and mortality rates of colorectal cancer in Malaysia.Epidemiol Health. 2016;38:e2016007. Goh KL, Quek KF, Yeo GTS, et al. Colorectal cancer in Asians:a demographic and anatomic survey in Malaysian patients undergoing colonoscopy.Aliment Pharmacol Ther. 2005;22:859-64. Magaji BA, Moy FM, Roslani AC, Law CW.Descriptive epidemiology of colorectal cancer in University Malaya Medical Centre, 2001 to 2010.Asian Pac J Cancer Prev. 2014;15:6059-64. Wang H, Seow A, Lee HP.Trends in cancer incidence among Singapore Malays:a low-risk population.Ann Acad Med Singapore. 2004;33:57-62. Sung JJ, Lau JY, Goh KL, Leung WK.Increasing incidence of colorectal cancer in Asia:implications for screening.Lancet Oncol. 2005;6:871-6. Chan YY, Lim KK, Lim KH, et al. Physical activity and overweight/obesity among Malaysian adults:findings from the 2015 National Health and Morbidity Survey (NHMS).BMC Public Health. 2017;17:733. Jan Mohamed HJ, Yap RW, Loy SL, et al. Prevalence and determinants of overweight, obesity, and type 2 diabetes mellitus in adults in Malaysia.Asia Pac J Public Health. 2015;27:123-35. Wang MJ, Ping J, Li Y, et al. The prognostic factors and multiple biomarkers in young patients with colorectal cancer.Sci Rep. 2015;5:10645. Ballester V, Rashtak S, Boardman L.Clinical and molecular features of young-onset colorectal cancer.World J Gastroenterol. 2016;22:1736-44. Stapley SA, Rubin GP, Alsina D, et al. Clinical features of bowel disease in patients aged <50 years in primary care:a large case-control study.Br J Gen Pract. 2017;67:e336-e344. Veettil SK, Lim KG, Chaiyakunapruk N, Ching SM, Abu Hassan MR.Colorectal cancer in Malaysia:its burden and implications for a multiethnic country.Asian J Surg. 2017;40:481-9. Syful Azlie MF, Hassan MR, Junainah S, Rugayah B.Immunochemical faecal occult blood test for colorectal cancer screening:a systematic review.Med J Malaysia. 2015;70:24-30. Koo JH, Leong RWL, Ching J, et al. Knowledge of, attitudes toward, and barriers to participation of colorectal cancer screening tests in the Asia-Pacific region:a multicenter study.Gastrointest Endosc. 2012;76:126-35. Chalya PL, McHembe MD, Mabula JB, et al. Clinicopathological patterns and challenges of management of colorectal cancer in a resource-limited setting:a Tanzanian experience.World J Surg Oncol. 2013;11:88. Shemesh-Bar L, Kundel Y, Idelevich E, et al. Colorectal cancer in young patients in Israel:a distinct clinicopathological entity?.World J Surg. 2010;34:2701-9. Zauber AG.The impact of screening on colorectal cancer mortality and incidence:has it really made a difference?.Dig Dis Sci. 2015;60:681-91. Pan J, Xin L, Ma YF, Hu LH, Li ZS.Colonoscopy reduces colorectal cancer incidence and mortality in patients with non-malignant findings:a meta-analysis.Am J Gastroenterol. 2016;111:355-65. Ministry of Health, MalaysiaNational strategic plan for cancer control programme 2016-2020. Available at: https://www.iccp-portal.org/system/files/plans/National_Strategic_Plan_Book_final%4025SEPT2017%20%281%29.pdf. Accessed August 1, 2019. Ministry of Health, MalaysiaClinical practice guidelines:management of colorectal carcinoma. Available at: http://www.acadmed.org.my/index.cfm?&menuid=67. Accessed August 1, 2019.
REFERENCES
1. Azizah Ab M, Nor Saleha IT, Noor Hashimah A, Asmah ZA, Mastulu W. Malaysian National Cancer Registry Report 2007-2011. Malaysia cancer statistics, data and figure. National Cancer Institute, Ministry of Health Malaysia. Available at: https://www.crc.gov.my/wp-content/uploads/documents/report/MNCRRrepor200.... Accessed August 1, 2019.
2. Arnold M, Sierra MS, Laversanne M, et al. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017; 66:683-91. https://doi.org/10.1136/gutjnl-2015-310912
PMid:26818619
3. Center MM, Jemal A, Smith RA, Ward E. Worldwide variations in colorectal cancer. CA Cancer J Clin 2009; 59:366-78. https://doi.org/10.3322/caac.20038
PMid:19897840
4. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015; 136:E359-86. https://doi.org/10.1002/ijc.29210
PMid:25220842
5. Siegel RL, Jemal A, Ward EM. Increase in incidence of colorectal cancer among young men and women in the United States. Cancer Epidemiol Biomarkers Prev 2009; 18:1695-8. https://doi.org/10.1158/1055-9965.EPI-09-0186
PMid:19505901
6. Siegel RL, Fedewa SA, Anderson WF, et al. Colorectal cancer incidence patterns in the United States, 1974-2013. J Natl Cancer Inst 2017; 109:djw322. https://doi.org/10.1093/jnci/djw322
7. Singh KE, Taylor TH, Pan CJG, Stamos MJ, Zell JA. Colorectal cancer incidence among young adults in California. J Adolesc Young Adult Oncol 2014; 3:176-84. https://doi.org/10.1089/jayao.2014.0006
PMid:25538862 PMCid:PMC4270106
8. Bailey CE, Hu CY, You YN, et al. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975-2010. JAMA Surg 2015; 150:17-22. https://doi.org/10.1001/jamasurg.2014.1756
PMid:25372703 PMCid:PMC4666003
9. Ganapathi S, Kumar D, Katsoulas N, et al. Colorectal cancer in the young: trends, characteristics and outcome. Int J Colorectal Dis 2011; 26:927-34. https://doi.org/10.1007/s00384-011-1174-z
PMid:21424713
10. Chou CL, Chang SC, Lin TC, et al. Differences in clinicopathological characteristics of colorectal cancer between younger and elderly patients: an analysis of 322 patients from a single institution. Am J Surg 2011; 202:574-82. https://doi.org/10.1016/j.amjsurg.2010.10.014
PMid:21872205
11. Nagai Y, Hata K, Kawai K, et al. Clinicopathological features of colorectal cancer patients under the age of 50: recent experience and case-control study of prognosis in a Japanese cohort. Digestion 2016; 93:272-9. https://doi.org/10.1159/000446344
PMid:27188463
12. Goldvaser H, Purim O, Kundel Y, et al. Colorectal cancer in young patients: is it a distinct clinical entity? Int J Clin Oncol 2016; 21:684-95. https://doi.org/10.1007/s10147-015-0935-z
PMid:26820719
13. Liang JT, Huang KC, Cheng AL, et al. Clinicopathological and molecular biological features of colorectal cancer in patients less than 40 years of age. Br J Surg 2003; 90:205-14. https://doi.org/10.1002/bjs.4015
PMid:12555297
16. Gupta S, Bhattacharya D, Acharya AN, et al. Colorectal carcinoma in young adults: a retrospective study on Indian patients: 2000-2008. Colorectal Dis 2010; 12:e182-9. https://doi.org/10.1111/j.1463-1318.2010.02223.x
PMid:20128837
17. Chiang JM, Chen MC, Changchien CR, et al. Favorable influence of age on tumor characteristics of sporadic colorectal adenocarcinoma: patients 30 years of age or younger may be a distinct patient group. Dis Colon Rectum 2003; 46:904-10. https://doi.org/10.1007/s10350-004-6683-1
PMid:12847364
18. Koh KS, Telisinghe PU, Bickle I, et al. Characteristics of young colorectal cancer in Brunei Darussalam: an epidemiologic study of 29 years (1986-2014). Asian Pac J Cancer Prev 2015; 16:3279-83. https://doi.org/10.7314/APJCP.2015.16.8.3279
PMid:25921132
19. Hav M, Eav S, Ky V, et al. Colorectal cancer in young Cambodians. Asian Pac J Cancer Prev 2011; 12:1001-5.
20. Rho YS, Gilabert M, Polom K, et al. Comparing clinical characteristics and outcomes of young-onset and late-onset colorectal cancer: an international collaborative study. Clin Colorectal Cancer 2017; 16:334-42. https://doi.org/10.1016/j.clcc.2017.03.008
PMid:28462853
21. O'Connell JB, Maggard MA, Liu JH, et al. Rates of colon and rectal cancers are increasing in young adults. Am Surg 2003; 69:866-72.
22. Quach DT, Nguyen OT. Clinical, endoscopic and pathogical characteristics of early-onset colorectal cancer in Vietnamese. Asian Pac J Cancer Prev 2012; 13:1767-70. https://doi.org/10.7314/APJCP.2012.13.5.1767
PMid:22901119
23. Park HC, Shin A, Kim BW, et al. Data on the characteristics and the survival of Korean patients with colorectal cancer from the Korea Central Cancer Registry. Ann Coloproctol 2013; 29:144-9. https://doi.org/10.3393/ac.2013.29.4.144
PMid:24032114 PMCid:PMC3767863
24. Ansari R, Mahdavinia M, Sadjadi A, et al. Incidence and age distribution of colorectal cancer in Iran: results of a population-based cancer registry. Cancer Lett 2006; 240:143-7. https://doi.org/10.1016/j.canlet.2005.09.004
PMid:16288832
25. Bishehsari F, Mahdavinia M, Vacca M, Malekzadeh R, Mariani-Costantini R. Epidemiological transition of colorectal cancer in developing countries: environmental factors, molecular pathways, and opportunities for prevention. World J Gastroenterol 2014; 20:6055-72. https://doi.org/10.3748/wjg.v20.i20.6055
PMid:24876728 PMCid:PMC4033445
26. Edwards BK, Ward E, Kohler BA, et al. Annual report to the nation on the status of cancer, 1975-2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer 2010; 116:544-73. https://doi.org/10.1002/cncr.24760
PMid:19998273 PMCid:PMC3619726
27. Huxley RR, Ansary-Moghaddam A, Clifton P, et al. The impact of dietary and lifestyle risk factors on risk of colorectal cancer: a quantitative overview of the epidemiological evidence. Int J Cancer 2009; 125:171-80. https://doi.org/10.1002/ijc.24343
PMid:19350627
28. Lee JM, Pilli S, Gebremariam A, et al. Getting heavier, younger: trajectories of obesity over the life course. Int J Obes (Lond) 2010; 34:614-23. https://doi.org/10.1038/ijo.2009.235
PMid:19949415 PMCid:PMC2926791
29. Aune D, Chan DSM, Lau R, et al. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose-response meta-analysis of prospective studies. BMJ 2011; 343:d6617. https://doi.org/10.1136/bmj.d6617
PMid:22074852 PMCid:PMC3213242
30. Nielsen SJ, Popkin BM. Patterns and trends in food portion sizes, 1977-1998. JAMA 2003; 289:450-3. https://doi.org/10.1001/jama.289.4.450
PMid:12533124
31. Brownson RC, Boehmer TK, Luke DA. Declining rates of physical activity in the United States: what are the contributors? Annu Rev Public Health 2005; 26:421-43. https://doi.org/10.1146/annurev.publhealth.26.021304.144437
PMid:15760296
32. Ezzati M, Riboli E. Behavioral and dietary risk factors for noncommunicable diseases. N Engl J Med 2013; 369:954-64. https://doi.org/10.1056/NEJMra1203528
PMid:24004122
33. Dejea CM, Wick EC, Hechenbleikner EM, et al. Microbiota organization is a distinct feature of proximal colorectal cancers. Proc Natl Acad Sci USA 2014; 111:18321-6. https://doi.org/10.1073/pnas.1406199111
PMid:25489084 PMCid:PMC4280621
34. Gagnière J, Raisch J, Veziant J, et al. Gut microbiota imbalance and colorectal cancer. World J Gastroenterol 2016; 22:501-18. https://doi.org/10.3748/wjg.v22.i2.501
PMid:26811603 PMCid:PMC4716055
35. Murphy EA, Velazquez KT, Herbert KM. Influence of high-fat diet on gut microbiota: a driving force for chronic disease risk. Curr Opin Clin Nutr Metab Care 2015; 18:515-20. https://doi.org/10.1097/MCO.0000000000000209
PMid:26154278 PMCid:PMC4578152
36. Clarke SF, Murphy EF, Nilaweera K, et al. The gut microbiota and its relationship to diet and obesity: new insights. Gut Microbes 2012; 3:186-202. https://doi.org/10.4161/gmic.20168
PMid:22572830 PMCid:PMC3427212
37. Modi SR, Collins JJ, Relman DA. Antibiotics and the gut microbiota. J Clin Invest 2014; 124:4212-8. https://doi.org/10.1172/JCI72333
PMid:25271726 PMCid:PMC4191029
38. Lange K, Buerger M, Stallmach A, Bruns T. Effects of antibiotics on gut microbiota. Dig Dis 2016; 34:260-8. https://doi.org/10.1159/000443360
PMid:27028893
39. Abu Hassan MR, Ismail I, Mohd Suan MA, et al. Incidence and mortality rates of colorectal cancer in Malaysia. Epidemiol Health 2016; 38: e2016007. https://doi.org/10.4178/epih.e2016007
PMid:26971697 PMCid:PMC5081307
40. Goh KL, Quek KF, Yeo GTS, et al. Colorectal cancer in Asians: a demographic and anatomic survey in Malaysian patients undergoing colonoscopy. Aliment Pharmacol Ther 2005; 22:859-64. https://doi.org/10.1111/j.1365-2036.2005.02646.x
PMid:16225496
41. Magaji BA, Moy FM, Roslani AC, Law CW. Descriptive epidemiology of colorectal cancer in University Malaya Medical Centre, 2001 to 2010. Asian Pac J Cancer Prev 2014; 15:6059-64. https://doi.org/10.7314/APJCP.2014.15.15.6059
PMid:25124558
42. Wang H, Seow A, Lee HP. Trends in cancer incidence among Singapore Malays: a low-risk population. Ann Acad Med Singapore 2004; 33:57-62.
43. Sung JJ, Lau JY, Goh KL, Leung WK. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol 2005; 6:871-6. https://doi.org/10.1016/S1470-2045(05)70422-8
44. Chan YY, Lim KK, Lim KH, et al. Physical activity and overweight/obesity among Malaysian adults: findings from the 2015 National Health and Morbidity Survey (NHMS). BMC Public Health 2017; 17:733. https://doi.org/10.1186/s12889-017-4772-z
PMid:28934939 PMCid:PMC5609047
45. Jan Mohamed HJ, Yap RW, Loy SL, et al. Prevalence and determinants of overweight, obesity, and type 2 diabetes mellitus in adults in Malaysia. Asia Pac J Public Health 2015; 27:123-35. https://doi.org/10.1177/1010539514562447
PMid:25524952
46. Wang MJ, Ping J, Li Y, et al. The prognostic factors and multiple biomarkers in young patients with colorectal cancer. Sci Rep 2015; 5:10645. https://doi.org/10.1038/srep10645
PMid:26013439 PMCid:PMC4445043
47. Ballester V, Rashtak S, Boardman L. Clinical and molecular features of young-onset colorectal cancer. World J Gastroenterol 2016; 22:1736-44. https://doi.org/10.3748/wjg.v22.i5.1736
PMid:26855533 PMCid:PMC4724605
48. Stapley SA, Rubin GP, Alsina D, et al. Clinical features of bowel disease in patients aged < 50 years in primary care: a large case-control study. Br J Gen Pract 2017; 67:e336-e344. https://doi.org/10.3399/bjgp17X690425
PMid:28347985 PMCid:PMC5409433
49. Veettil SK, Lim KG, Chaiyakunapruk N, Ching SM, Abu Hassan MR. Colorectal cancer in Malaysia: its burden and implications for a multiethnic country. Asian J Surg 2017; 40:481-9. https://doi.org/10.1016/j.asjsur.2016.07.005
PMid:27492344
50. Syful Azlie MF, Hassan MR, Junainah S, Rugayah B. Immunochemical faecal occult blood test for colorectal cancer screening: a systematic review. Med J Malaysia 2015; 70:24-30.
51. Koo JH, Leong RWL, Ching J, et al. Knowledge of, attitudes toward, and barriers to participation of colorectal cancer screening tests in the Asia-Pacific region: a multicenter study. Gastrointest Endosc 2012; 76:126-35. https://doi.org/10.1016/j.gie.2012.03.168
PMid:22726471
52. Chalya PL, McHembe MD, Mabula JB, et al. Clinicopathological patterns and challenges of management of colorectal cancer in a resource-limited setting: a Tanzanian experience. World J Surg Oncol 2013; 11:88. https://doi.org/10.1186/1477-7819-11-88
PMid:23597032 PMCid:PMC3637367
53. Shemesh-Bar L, Kundel Y, Idelevich E, et al. Colorectal cancer in young patients in Israel: a distinct clinicopathological entity? World J Surg 2010; 34:2701-9. https://doi.org/10.1007/s00268-010-0748-1
PMid:20809152
54. Zauber AG. The impact of screening on colorectal cancer mortality and incidence: has it really made a difference? Dig Dis Sci 2015; 60:681-91. https://doi.org/10.1007/s10620-015-3600-5
PMid:25740556 PMCid:PMC4412262
55. Pan J, Xin L, Ma YF, Hu LH, Li ZS. Colonoscopy reduces colorectal cancer incidence and mortality in patients with non-malignant findings: a meta-analysis. Am J Gastroenterol 2016; 111:355-65. https://doi.org/10.1038/ajg.2015.418
PMid:26753884 PMCid:PMC4820666
57. Ministry of Health, Malaysia. Clinical practice guidelines: management of colorectal carcinoma. Available at: http://www.acadmed.org.my/index.cfm?&menuid=67. Accessed August 1, 2019.