

Abstract
A 29-year-old man with a previous football injury to his left knee presented with pain of the same knee. The patient twisted it as he was turning a corner quickly while going up the stairs, leading to internal rotation of his femur on his tibia with his knee in flexion. MR imaging revealed a bucket-handle tear of the medial meniscus, as well as a complete tear of the anterior cruciate ligament. However, image interpretation was complicated by the presence of a medial oblique meniscomeniscal ligament, a rare normal variant among intermeniscal ligaments of the knee. All four recognised variants of intermeniscal ligaments are discussed, with emphasis on their prevalence, imaging and anatomical features, and the way in which they may mimic meniscal tears.
CASE PRESENTATION
A 29-year-old man presented with pain in his left knee. He had twisted it as he turned a corner quickly while going up the stairs, leading to an internal rotation of his femur on his tibia while his knee was in flexion. He had twisted the same knee a few years ago when playing football, with resultant knee pain, instability and occasional locking. He had not sought treatment then, as the pain had subsequently improved, although the other symptoms had persisted. Physical examination revealed no swelling, but the range of motion of the left knee was reduced and the anterior drawer test was positive. Subsequent imaging of the knee revealed largely unremarkable radiographic findings. Magnetic resonance (MR) imaging findings are shown in Figs.
Fig. 1
Sagittal proton density (PD)-weighted fast spin-echo (FSE) MR image of the left knee.
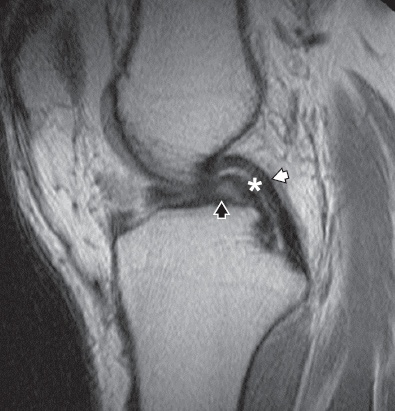
Fig. 2
Serial coronal PD-weighted FSE MR images from the posterior to anterior aspect of the left knee. The medial compartment is on the left side of the images.
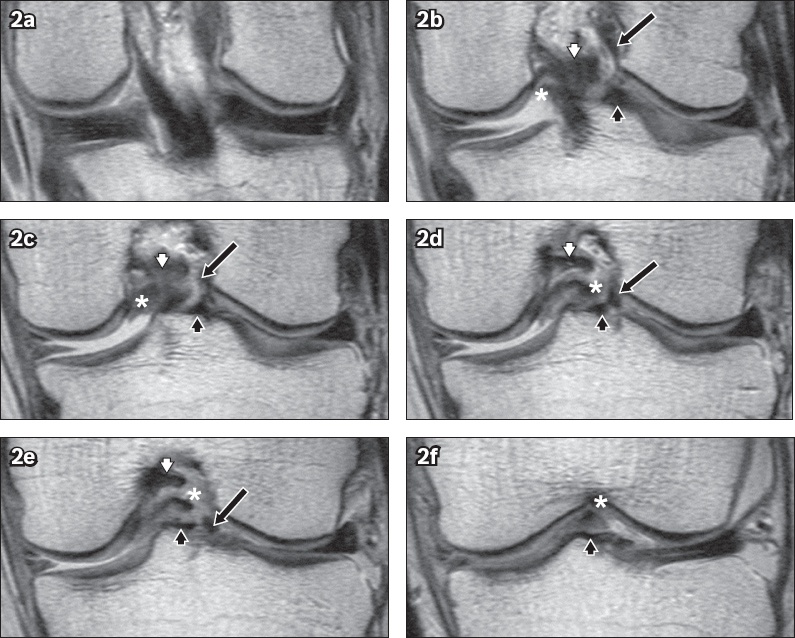
IMAGE INTERPRETATION
MR images show two additional structures within the intercondylar fossa of the knee besides the two structures usually found in the fossa, namely the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). The first is a low-signal-intensity band (* in Figs.
DIAGNOSIS
Medial meniscus bucket-handle tear with medial oblique meniscomeniscal (MM) ligament.
CLINICAL COURSE
Subsequent arthroscopy confirmed all the MR imaging findings. The patient underwent an ACL reconstruction and repair of the medial meniscus bucket-handle tear. He was discharged well after receiving gait training and being issued with crutches. The patient was subsequently followed up by a physiotherapist.
DISCUSSION
The C-shaped fibrocartilaginous menisci of the knee aid in joint stabilisation and load transmission. Four different types of MM ligaments have been described in the medical literature.(1-3) The most commonly observed of these intermeniscal ligaments is the anterior intermeniscal ligament, with a reported frequency of 58%, followed by the posterior intermeniscal ligament, with a reported frequency of 1%–4%.(1) The other two variants are the medial and lateral oblique MM ligaments, which are reported at a combined frequency of 1%–4%.(1) Chan and Goldblatt described two other variants extending from the anterior to the posterior horns of the corresponding medial and lateral menisci, respectively, which they termed unilateral MM ligaments.(4) However, these may merely represent ring menisci, a rare congenital variant characterised by a ring shape; the anterior and posterior horns are connected by an inner horn bridge and present on imaging as complete rings of meniscal tissue.(5)
Oblique MM ligaments are named based on their anterior attachment site.
Fig. 3
Line drawings (viewed from above) show (a) the normal menisci and oblique meniscomeniscal (MM) ligament variants; (b) the medial oblique MM ligament attached to the anterior horn of the medial meniscus and the posterior horn of the lateral meniscus; and (c) the lateral oblique MM ligament attached to the anterior horn of the lateral meniscus and the posterior horn of the medial meniscus.
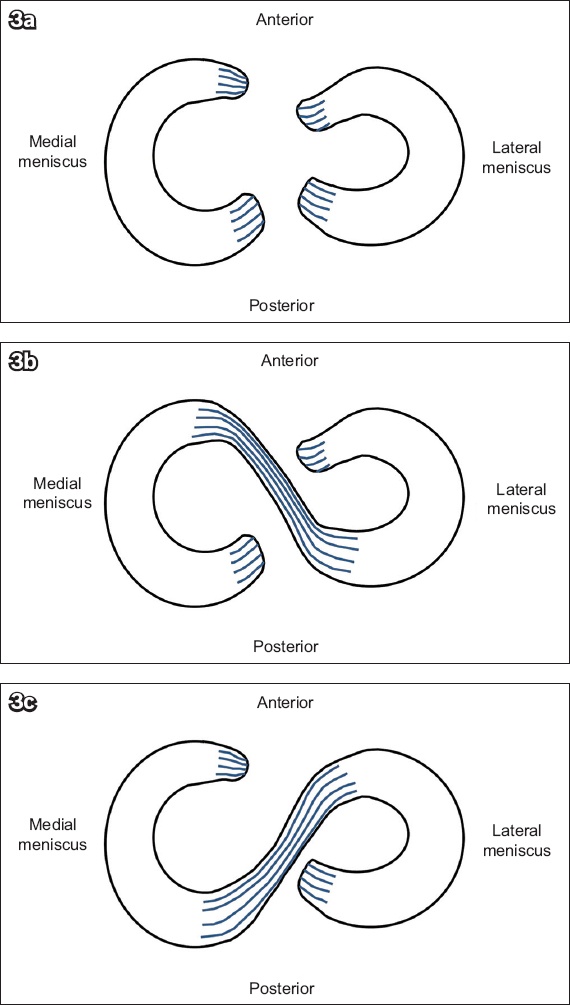
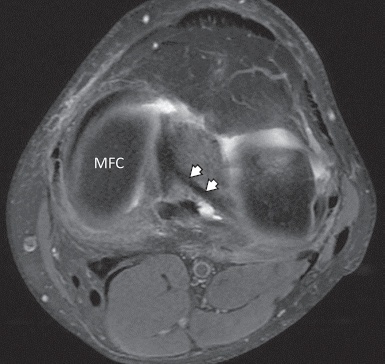
Fig. 4
Axial fat-suppressed PD-weighted FSE MR image of the left knee shows the medial oblique meniscomeniscal ligament (arrowheads) attached to the anterior horn of the medial meniscus and the posterior horn of the lateral meniscus. MFC: medial femoral condyle
The oblique MM ligament may be misinterpreted as a bucket-handle tear of the meniscus since it possesses signal intensity that is similar to that of meniscal tissue and also attaches to the meniscus.(6) It can also be mistaken for a torn ACL or PCL. In our case, the patient did have a bucket-handle tear of the medial meniscus, which accounts for the double PCL sign. However, this rare occurrence of a concurrent oblique MM ligament resulted in an imaging finding that was equivalent to a triple PCL sign (
Fig. 5
A separate patient with an oblique meniscomeniscal (MM) ligament without superimposed bucket-handle tear, and a high-grade tear of the anterior cruciate ligament. Serial sagittal fat-suppressed PD-weighted FSE MR images from the lateral to medial aspect of the knee show the course of the medial oblique MM ligament (arrowhead) from the posterior horn of the lateral meniscus to the anterior horn of the medial meniscus. The posterior cruciate ligament (PCL) is intact (*). There is an apparent double PCL sign, as in
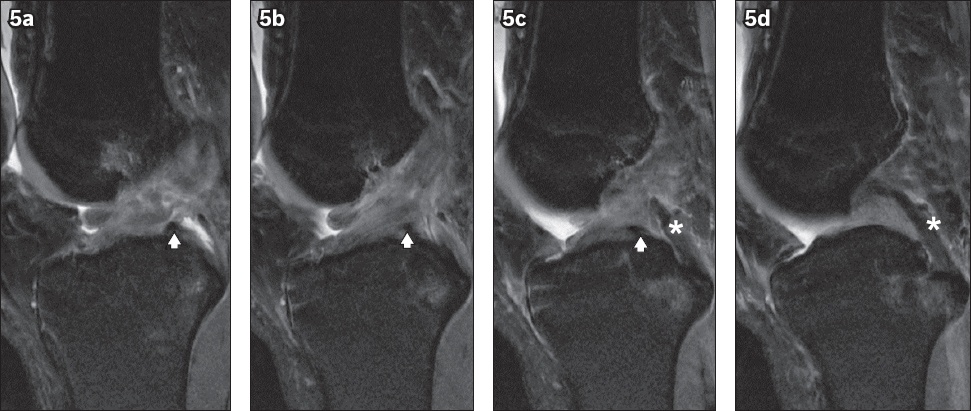
The double PCL sign in the context of a bucket-handle medial meniscal tear is often seen only in patients with an intact ACL, as the intact ACL prevents the flipped fragment from migrating further laterally or not aligning with the PCL.(7) In a minority of patients, a lateral meniscus bucket-handle tear, in the presence of a torn ACL, may also give rise to a double PCL sign. That we were able to see the double PCL sign in our case, despite the torn ACL, may be due to the limiting presence of the oblique MM ligament and remnant torn ACL fibres. Another potential pitfall of the double PCL sign is the presence of a normal anterior meniscofemoral ligament, also known as the ligament of Humphry, which extends from the lateral meniscus posterior horn to the lateral aspect of the medial femoral condyle. This ligament can be differentiated from a bucket-handle fragment by its relatively smaller size and thickness, as well as its extremely close proximity to the PCL.(6) To avoid both of these pitfalls, these ligaments must be carefully traced entirely from their origin to insertion, and corroborated with the normal morphological features of the adjacent menisci.
The anterior and posterior intermeniscal ligaments can also mimic tears at their meniscal attachment sites. The anterior intermeniscal ligament is described in Gray’s Anatomy as “connecting the anterior convex margin of the lateral meniscus to the anterior end of the medial meniscus.”(8) However, Nelson and LaPrade have described three types of insertion: Type I has attachments to the anterior horn of the medial meniscus and anterior margin of the lateral meniscus; Type II has a medial attachment to the anterior margin of the medial meniscus and a lateral attachment to the joint capsule anterior to the lateral meniscus; and Type III has medial and lateral capsular anterior attachments without direct attachments to the anterior horns of either the medial or lateral menisci.(9) Type I, which fits the classic description of primary attachments, is the most common (Figs.
Fig. 6
Axial PD-weighted FSE MR image of the left knee shows an anterior intermeniscal ligament (arrowheads). MFC: medial femoral condyle
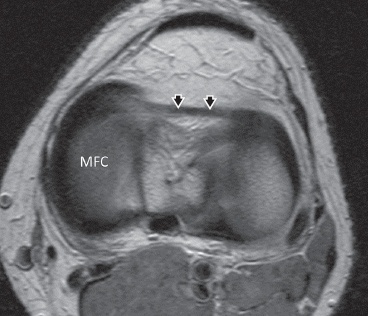
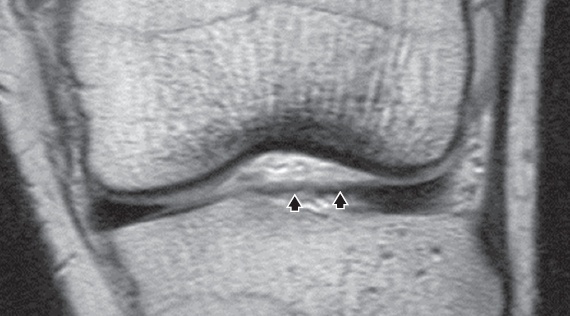
Fig. 7
Coronal PD-weighted FSE MR image shows an anterior intermeniscal ligament (arrowheads).
Regardless of insertion type, the region of confluence of the ligament with the anterior horn of the lateral meniscus and its central tendinous attachments can give the appearance of a high-signal cleft within the meniscus on sagittal images.(10) Pseudotears of the anterior horn of the lateral meniscus are seen in 22%–38% of MR imaging examinations of the knee due to the course of the intermeniscal ligament.(11) In reality, isolated tears of the anterior horn of the lateral meniscus are relatively rare and account for only 16% of lateral meniscal tears.(5)
Similarly, normal anatomic interfaces may also mimic meniscal tears in the case of the posterior intermeniscal ligament (
Fig. 8
Axial PD-weighted FSE MR image shows a posterior intermeniscal ligament (arrowheads) attached to the respective posterior horns of the medial and lateral menisci. MFC: medial femoral condyle.
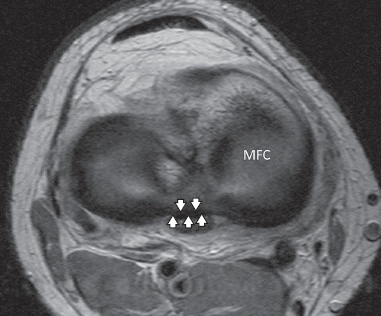
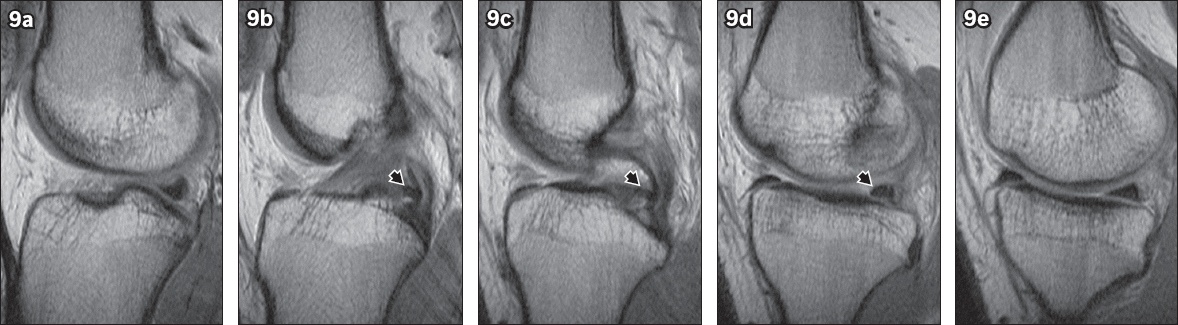
Fig. 9
Serial sagittal PD-weighted FSE MR images from the lateral to medial aspect of the knee show the course of the posterior intermeniscal ligament (arrowhead in 9b–d) as it attaches to the posterior horns of the medial and lateral menisci. Increased signal intensity at the interface between the ligament and posterior horn of the lateral meniscus mimics a tear (9d). The ligament can also be misinterpreted as a displaced meniscal fragment (9c).
In conclusion, one must be aware of the MM ligament variants of the knee during MR imaging, as they can mimic meniscal tears. By tracing these ligaments along their entire course from origin to insertion, these variants can be correctly identified, using the normal morphology of the adjacent meniscus as further supporting evidence.
SMJ-58-245.pdf