Author Information >Copyright and License information >
1Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore 2Department of Emergency Medicine, Tan Tock Seng Hospital, Singapore Correspondence: Dr Chiu Li Qi, Consultant, Department of Emergency Medicine, Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng Singapore 308433. chiuliqi@gmail.com
With Singapore’s ageing population, there are increasing numbers of elderly cyclists and motorcyclists. Compared to younger riders, this cohort sustains more injuries and has poorer outcomes. This study aimed to describe and compare patient demographics, injury patterns and outcomes among elderly cyclists and motorcyclists at a Level 1 trauma centre.
METHODS
Data of all cyclists, motorcyclists and pillion riders aged 65 years and above who presented to the emergency department after accidents from 1 January 2013 to 31 December 2017 was extracted from the hospital’s trauma registry and reviewed.
RESULTS
Cyclists and motorcyclists formed 42.0% and 58.0%, respectively, of 157 recruited patients. At the time of the accident, 40.8% of the patients were employed. The mean age of the patients was 71.6 ± 5.8 years. Extremities and pelvic girdle injuries (61.1%) were the most frequent, followed by chest injuries (48.4%), and head and neck injuries (40.1%). Among severe injuries (defined as Abbreviated Injury Scale score ≥ 3), chest injuries (39.5%) were the most common, followed by head and neck injuries (36.3%). The overall mortality rate was 9.6%, with cyclists at nearly three times the risk compared to motorcyclists. More cyclists than motorcyclists (18.2% vs. 11.0%) required intensive care. There were no significant differences in the length of hospital stay between cyclists and motorcyclists.
CONCLUSION
Elderly riders have unique injury patterns and consume significant healthcare resources. Trauma systems need to acknowledge this changing injury epidemiology and equip trauma centres with the necessary resources targeted at elderly patients. Future work should focus on strategies to minimise extremity and chest injuries.
Singapore is a city-state with a high population density of 7,804 persons/km2 and an ageing population, with nearly 13% of the population aged above 65 years.(1) During 2013–2017, national statistics showed a total of 21,415 motorcycle fatalities.(2) Of these, 12% were associated with motorcyclists aged above 60 years.(2) Motorcycles and bicycles are important and affordable modes of transport whose increasing popularity is also related to the advent of bicycle-sharing systems and a demand for food delivery services. Data from the Singapore Police Force and other local studies has shown that motorcyclists and cyclists are among the most vulnerable road users.(3-5) Regionally, motorcyclists and cyclists (along with pedestrians) make up half of all road traffic deaths in Southeast Asia.(6) Studies have shown that compared to younger riders, elderly motorcyclists sustain more injuries(7-9) as well as more severe injuries,(9-14) and show different injury patterns.(9,14) The increasing age of motorcyclists correlated with prolonged hospital stay,(9,10,14,15) increased complications,(9,10,15) increased mortality(10,14,15) and higher care demands after discharge.(9) Similarly, for cyclists, older age was associated with increased injury severity, mortality and length of intensive care unit stay.(16-19)
Current literature comparing cyclists and motorcyclists has revealed differences in injury patterns and outcomes.(20-22) However, to our knowledge, no study has been done to evaluate injury patterns and outcomes specifically in elderly cyclists and motorcyclists. This study aimed to describe and compare the patterns of injuries in elderly cyclists and motorcyclists presenting to the emergency department (ED) at Tan Tock Seng Hospital (TTSH), Singapore.
METHODS
This was a retrospective review of all electronic medical records of cyclists, motorcyclists and pillion riders aged 65 years and above who presented to the ED at TTSH from 1 January 2013 to 31 December 2017 following accidents. TTSH is a 1,600-bed Level 1 trauma centre situated in a region of high population density and older housing estates. It has the busiest ED in Singapore, with over 170,000 attendances annually.
Data was obtained from the hospital’s trauma registry. Data collected included patient demographics, mode of conveyance to the ED, triage Patient Acuity Category (PAC) scores, injury characteristics and patient outcomes. Injury characteristics included the epidemiology and severity of injuries according to Abbreviated Injury Scale (AIS) scores, Injury Severity Score (ISS), Revised Trauma Score (RTS) and probability of survival (Ps) scores. The study was approved by the National Healthcare Group Domain Specific Review Board.
Analysis was done using IBM SPSS Statistics version 25.0 (IBM Corp, Armonk, NY, USA). Means and standard deviations, and medians and interquartile ranges were calculated for normal and non-normal variables, respectively. Frequencies were tabulated for categorical variables. Student’s t-test and chi-square test were used for analysis. A p-value < 0.05 was considered statistically significant.
RESULTS
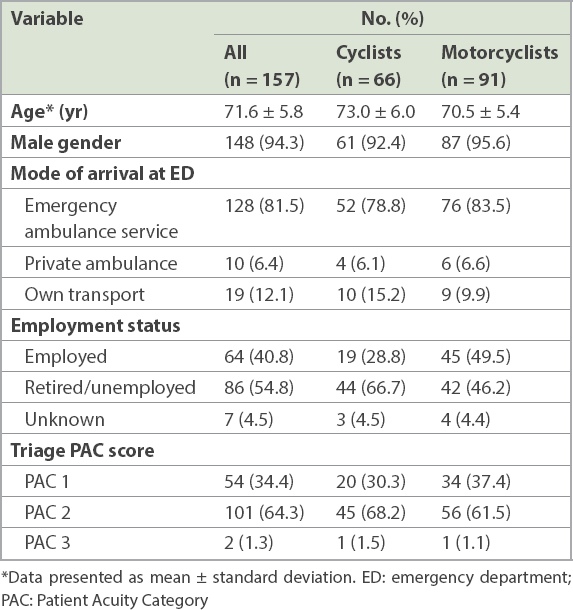
A total of 157 elderly cyclists and motorcyclists presented to our centre from 1 January 2013 to 31 December 2017. Of these, 42.0% (n = 66) were cyclists. The mean age of the patients was 71.6 ± 5.8 years. Most riders (94.3%) were men. At the time of the accident, 40.8% of the patients were employed. A majority (81.5%) of patients arrived at the ED via emergency ambulance services and were triaged as PAC 2 (64.3%). One-third (34.4%) of the patients were triaged as PAC 1 and managed in the resuscitation area. The characteristics of cyclists and motorcyclists were similar, except that a higher proportion of elderly cyclists were retired or unemployed (66.7%) when compared to motorcyclists (46.2%). Table I shows the demographics of the study population.
Table I
Demographics of elderly cyclists and motorcyclists.
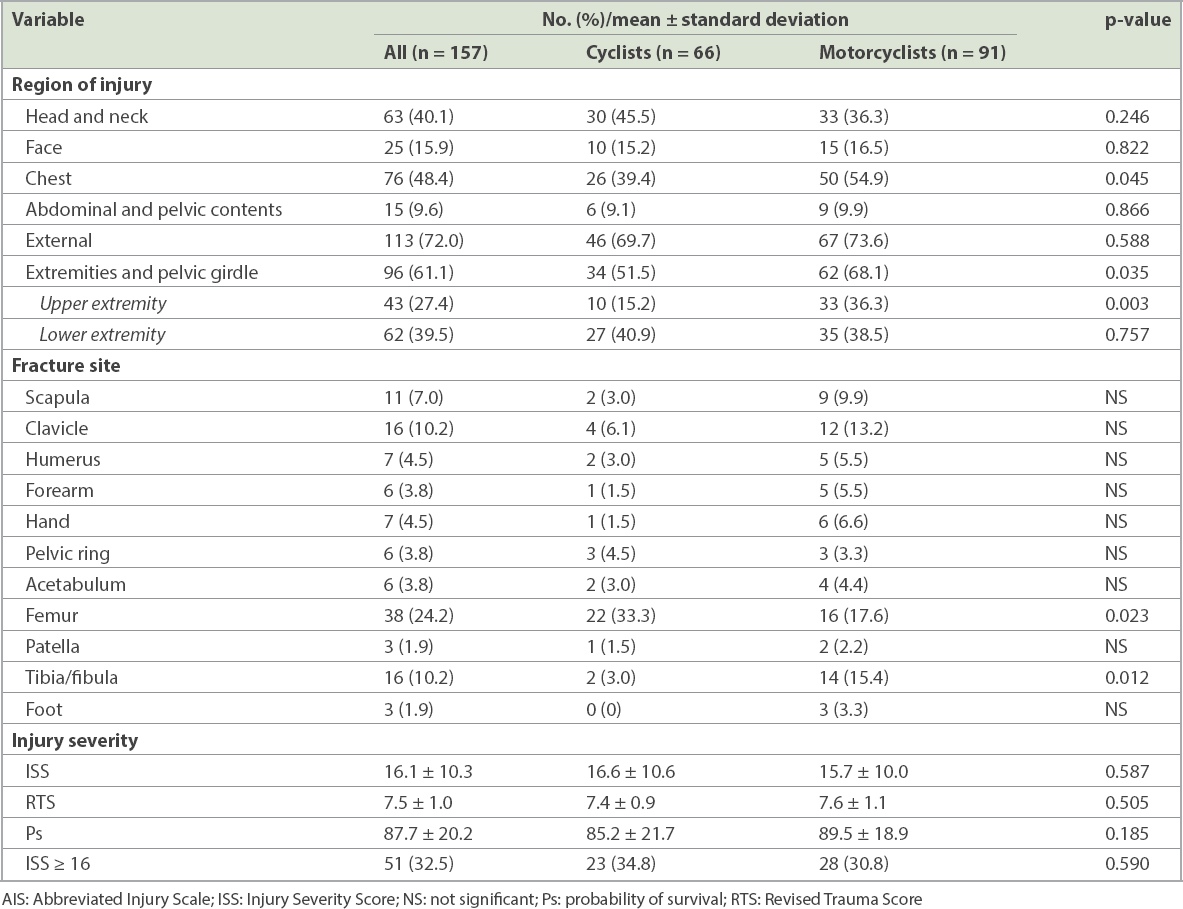
Table II shows the injury patterns categorised according to AIS regions. Excluding AIS region 6 (external system), injuries involving extremities and the pelvic girdle (61.1%) were the most frequent, followed by chest injuries (48.4%), and head and neck injuries (40.1%). Among severe injuries (defined as AIS score ≥ 3), chest injuries were the most common (39.5%), followed by head and neck injuries (36.3%), and extremity and pelvic girdle injuries (34.4%). The occurrence of severe chest injuries (p = 0.045), and extremity and pelvic girdle injuries (p = 0.035) among motorcyclists were significantly higher than among cyclists. Among extremity injuries, femoral fractures (24.2%) were the most common. A significantly higher proportion of motorcyclists sustained upper extremity injuries when compared to cyclists (p = 0.003). Cyclists sustained significantly more femoral fractures than motorcyclists (p = 0.023). The reverse was observed for tibia/fibular fractures (p = 0.012). There were no significant differences in the mean ISS, RTS and Ps scores between cyclists and in the motorcyclists, and in the proportion of patients with major trauma (defined as ISS ≥ 16).
Table II
Injury patterns of elderly cyclists and motorcyclists according to AIS regions.
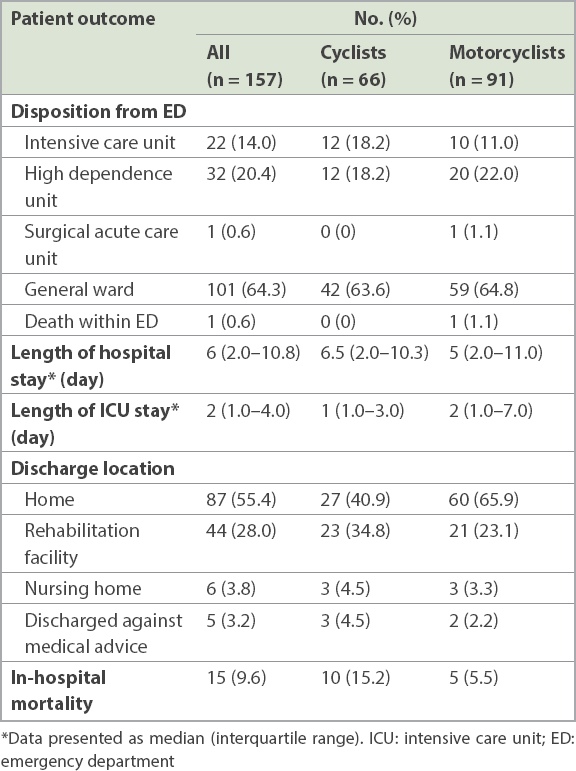
Table III shows the outcomes of our patients. One patient succumbed to injuries within the ED. All other patients required hospital admission, with a median length of stay of 6.0 (range 2.0–10.8) days. The overall mortality rate was 9.6%, with cyclists having nearly three times the mortality risk of motorcyclists. All of the 15 patients who died were men and had an average age of 74 years, and one-third were motorcyclists. The average length of stay before death was 3.6 days, with 11 patients dying within the first day of admission, three patients dying within the first week and one patient dying after a prolonged stay of one month. Head injuries (n = 9) were the overwhelming cause of death, with other reasons being head and chest injuries (n = 2), multiple injuries (n = 2) and blunt abdominopelvic injuries (n = 1). The patient who died at the one-month mark succumbed to pneumonia and renal failure subsequent to head injury. Among the survivors, one-third of both cyclists and motorcyclists required admission to the intensive care unit or high-dependency unit, while most of the others were admitted to the general ward. More cyclists than motorcyclists (18.2% vs. 11.0%) required intensive care. There were no significant differences in the length of hospital stay and disposition status among these patients. A majority (55.4%) of patients were discharged home and 28.0% of patients were discharged to a rehabilitation facility.
Table III
Outcomes of elderly cyclists and motorcyclists.
DISCUSSION
To our knowledge, this is the first study that compares injury patterns among elderly cyclists and motorcyclists. According to local statistics, elderly motorcyclists made up approximately 12% of all traffic casualties during the study period.(2) Our results showed that 40.8% of patients were employed at the time of their accident. This suggests that despite the prevailing retirement age of 62 years, a large proportion of the elderly remain actively employed and contribute to the economy. Accidents in this cohort thus represent potential societal economic losses.
Care for this group consumes more healthcare resources than that for younger patients, as evidenced by one-third of our patients requiring management in the resuscitation area with subsequent admission to the intensive care unit and high-dependency unit. More than a quarter of our patients were discharged to a rehabilitation facility. Unfortunately, longitudinal data on functional outcomes was incomplete, and the impact on long-term outcomes among our patients could not be determined. Nevertheless, our findings emphasised the impact older riders have on healthcare resource utilisation and were similar to the findings of other studies.(9,18)
Results revealed that among elderly cyclists and motorcyclists, the extremities and pelvic girdle region were the most vulnerable to injury. This was consistent with previous studies involving cyclists(18,19,23-27) and motorcyclists.(11,27,28) However, the patterns of extremity injuries differed between cyclists and motorcyclists in our study. Motorcyclists sustained significantly higher rates of upper extremity injuries and tibia/fibular fractures, while cyclists sustained significantly more femoral fractures. Apart from Liu et al,(20) who found that cyclists had a higher odds ratio for femoral fractures when compared to motorcyclists, few studies have been done to investigate these differences. Further studies focusing on injury mechanisms are needed. Unlike head injuries, which may be reduced by helmet use, little is known about prevention of extremity injuries. Studies have shown that extremity injuries have high healthcare and productivity costs,(29,30) and are negatively associated with the quality of well-being outcome.(31,32) Resources should be allocated to investigate ways to minimise extremity injuries in order to reduce associated morbidity and economic costs.
The occurrence of severe chest injuries was significantly higher in elderly motorcyclists than in cyclists. Thoracic injuries are clinically significant because they are more likely to be associated with fatal outcomes,(7,33) and this risk increases with age.(12) As the area of thoracic exposure is comparable, a possible explanation could be that motorcyclists sustain greater impact during accidents due to higher speeds. This has a significant bearing on injury prevention for elderly motorcyclists. Possible strategies to explore include stricter laws regarding speed limits and protective gear.
It is well established that helmets reduce the frequency and severity of head injuries in riders. Current traffic laws in Singapore do not mandate the use of helmets for cyclists. Interestingly, our study did not show any significant differences in head injuries between cyclists and motorcyclists. However, as this was not an a priori analysis, further studies specifically designed to evaluate the utility of helmets for head injury prevention in our population are necessary.
There were some limitations to this study. It was a retrospective, single-centre study with a small sample size. It omitted data from riders who did not present to the ED or died at the scene of the accident. Although it can be assumed that persons who did not present to the ED probably had more minor injuries, injury patterns among the most severely injured patients in our study were not captured. Longitudinal data regarding functional capacity after discharge was also unavailable for comparison due to these patients being lost to follow-up.
In conclusion, elderly motorcyclists and cyclists have unique injury patterns and consume significant healthcare resources. As our population ages and two-wheeled vehicles continue to be an indispensable mode of transport, this burden of injury will only increase. Trauma systems need to acknowledge this changing injury epidemiology and equip trauma centres with the necessary resources targeted at elderly riders. Future work should focus on strategies to minimise extremity and chest injuries. A prospective multicentre study using the nation’s trauma database would be useful to assess the national burden of geriatric trauma among cyclists and motorcyclists. In addition, such a study should address possible differences in epidemiology and outcomes among younger riders when compared to older ones.
About the First Author
Dr Cheong Hui Shyuan is a medical officer who is currently still exploring her interests. One year into working life, she still enjoys her work and interacting with patients. In her free time, she enjoys spending precious time with family and friends, and a good yoga or spin session. She is fervently hoping for the day travel restrictions are lifted and she can go hiking again.
References Department of Statistics, SingaporePopulation and Population Structure. Available at: https://www.singstat.gov.sg/find-data/search-by-theme/population/population-and-population-structure/latest-data. Accessed January 4, 2019. Singapore Police ForceTraffic Annual 2017.Publication [online]. Available at: https://www.police.gov.sg/news-and-publications/publications?category=Annual%20Reports. Accessed December 20, 2018. Wong ZH, Chong CK, Tai BC, Lau G.A review of fatal road traffic accidents in Singapore from 2000 to 2004.Ann Acad Med Singapore. 2009;38:594-6. Wong E, Leong MK, Anantharaman V, et al. Road traffic accident mortality in Singapore.J Emerg Med. 2002;22:139-46. World Health OrganizationRoad Safety in the South-East Asian Region 2015. Available at: http://www.who.int/violence_injury_prevention/road_safety_status/2015/Road_Safety_SEAR_3_for_web.pdf. Accessed December 20, 2018. Department of Statistics, SingaporePopulation Overview. Available at: https://www.singstat.gov.sg/find-data/search-by-theme/population/population-and-population-structure/visualising-data/population-trends. Accessed May 6, 2018. Dischinger PC, Ryb GE, Ho SM, Braver ER.Injury patterns and severity among hospitalised motorcyclists:a comparison of younger and older riders.Annu Proc Assoc Adv Automot Med. 2006;50:237-49. Ashie A, Wilhelm A, Carney D, DiPasquale T, Bush C.Comparing fracture patterns of younger versus older riders involved in nonfatal motorcycle accidents.Traffic Inj Prev. 2018;19:761-5. Muratore S, Hawes L, Farhat J, et al. Riding into the golden years:injury patterns and outcomes of advanced-age motorcycle trauma.Am J Surg. 2016;212:670-6. Brown JB, Bankey PE, Gorczyca JT, et al. The aging road warrior:national trend toward older riders impacts outcome after motorcycle injury.Am Surg. 2010;76:279-86. Jackson TL, Mello MJ.Injury patterns and severity among motorcyclists treated in US emergency departments, 2001-2008:a comparison of younger and older riders.Inj Prev. 2013;19:297-302. Talving P, Teixeira PG, Barmparas G, et al. Motorcycle-related injaes:effect of age on type and severity of injaes and mortality.J Trauma. 2010;68:441-6. Stutts J, Foss R, Svoboda C.Characteristics of older motorcyclist crashes.Annu Proc Assoc Adv Automot Med. 2004;48:197-211. Hsieh CH, Liu HT, Hsu SY, Hsieh HY, Chen YC.Motorcycle-related hospitalizations of the elderly.Biomed J. 2017;40:121-8. Warlick B, Nuismer A, Israel H, Cannada LK.The aging motorcyclist:a comparative epidemiologic study on pattern and severity of injury.J Trauma Acute Care Surg. 2012;73:175-8. Chong S, Poulos R, Olivier J, Watson WL, Grzebieta R.Relative injury severity among vulnerable non-motorised road users:comparative analysis of injury arising from bicycle-motor vehicle and bicycle-pedestrian collisions.Accid Anal Prev. 2010;42:290-6. Cripton PA, Shen H, Brubacher JR, et al. Severity of urban cycling injaes and the relationship with personal, trip, route and crash characteristics:analyses using four severity metrics.BMJ Open. 2015;5:e006654. Lustenberger T, Inaba K, Talving P, et al. Bicyclists injured by automobiles:relationship of age to injury type and severity--a national trauma databank analysis.J Trauma. 2010;69:1120-5. Rivara FP, Thompson DC, Thompson RS.Epidemiology of bicycle injaes and risk factors for serious injury.Inj Prev. 1997;3:110-4. Liu HT, Rau CS, Liang CC, et al. Bicycle-related hospitalizations at a Taiwanese level I Trauma Center.BMC Public Health. 2015;15:722. Pai CW, Chen YC, Lin HY, Chen PL.A population-based case-control study of hospitalisation due to head injaes among bicyclists and motorcyclists in Taiwan.BMJ Open. 2017;7:e018574. Pai CW, Lin HY, Tsai SH, Chen PL.Comparison of traffic-injury related hospitalisation between bicyclists and motorcyclists in Taiwan.PLoS One. 2018;13:e0191221. Davidson JA.Epidemiology and outcome of bicycle injaes presenting to an emergency department in the United Kingdom.Eur J Emerg Med. 2005;12:24-9. Dinh MM, Kastelein C, Hopkins R, et al. Mechanisms, injaes and helmet use in cyclists presenting to an inner city emergency department.Emerg Med Australas. 2015;27:323-7. Neumann MV, Eley R, Vallmuur K, Schuetz M.Current profile of cycling injaes:a retrospective analysis of a trauma centre level 1 in Queensland.Emerg Med Australas. 2016;28:90-5. Gopinath B, Jagnoor J, Craig A, et al. Describing and comparing the characteristics of injured bicyclists and other injured road users:a prospective cohort study.BMC Public Health. 2016;16:324. Chichom-Mefire A, Atashili J, Tsiagadigui JG, Fon-Awah C, Ngowe-Ngowe M.A prospective pilot cohort analysis of crash characteristics and pattern of injaes in riders and pillion passengers involved in motorcycle crashes in an urban area in Cameroon:lessons for prevention.BMC Public Health. 2015;15:915. Tham KY, Seow E, Lau G.Pattern of injaes in helmeted motorcyclists in Singapore.Emerg Med J. 2004;21:478-82. Meerding WJ, Looman CW, Essink-Bot ML, et al. Distribution and determinants of health and work status in a comprehensive population of injury patients.J Trauma. 2004;56:150-61. Polinder S, Haagsma J, Panneman M, et al. The economic burden of injury:health care and productivity costs of injaes in the Netherlands.Accid Anal Prev. 2016;93:92-100. Holbrook TL, Anderson JP, Sieber WJ, Browner D, Hoyt DB.Outcome after major trauma:discharge and 6-month follow-up results from the Trauma Recovery Project.J Trauma. 1998;45:315-24. Holbrook TL, Anderson JP, Sieber WJ, Browner D, Hoyt DB.Outcome after major trauma:12-month and 18-month follow-up results from the Trauma Recovery Project.J Trauma. 1999;46:765-73. Doyle D, Muir M, Chinn B.Motorcycle accidents in Strathclyde Region, Scotland dang 1992:a study of the injaes sustained.Health Bull (Edinb). 1995;53:386-94.
3. Wong ZH, Chong CK, Tai BC, Lau G. A review of fatal road traffic accidents in Singapore from 2000 to 2004. Ann Acad Med Singapore 2009; 38:594-6.
4. Wong E, Leong MK, Anantharaman V, et al. Road traffic accident mortality in Singapore. J Emerg Med 2002; 22:139-46. https://doi.org/10.1016/S0736-4679(01)00455-3
7. Dischinger PC, Ryb GE, Ho SM, Braver ER. Injury patterns and severity among hospitalised motorcyclists: a comparison of younger and older riders. Annu Proc Assoc Adv Automot Med 2006; 50:237-49.
8. Ashie A, Wilhelm A, Carney D, DiPasquale T, Bush C. Comparing fracture patterns of younger versus older riders involved in nonfatal motorcycle accidents. Traffic Inj Prev 2018; 19:761-5. https://doi.org/10.1080/15389588.2018.1494384
PMid:29985641
9. Muratore S, Hawes L, Farhat J, et al. Riding into the golden years: injury patterns and outcomes of advanced-age motorcycle trauma. Am J Surg 2016; 212:670-6. https://doi.org/10.1016/j.amjsurg.2016.06.011
PMid:27570081
10. Brown JB, Bankey PE, Gorczyca JT, et al. The aging road warrior: national trend toward older riders impacts outcome after motorcycle injury. Am Surg 2010; 76:279-86. https://doi.org/10.1177/000313481007600308
PMid:20349657
11. Jackson TL, Mello MJ. Injury patterns and severity among motorcyclists treated in US emergency departments, 2001-2008: a comparison of younger and older riders. Inj Prev 2013; 19:297-302. https://doi.org/10.1136/injuryprev-2012-040619
PMid:23393164
12. Talving P, Teixeira PG, Barmparas G, et al. Motorcycle-related injuries: effect of age on type and severity of injuries and mortality. J Trauma 2010; 68:441-6. https://doi.org/10.1097/TA.0b013e3181cbf303
PMid:20154556
13. Stutts J, Foss R, Svoboda C. Characteristics of older motorcyclist crashes. Annu Proc Assoc Adv Automot Med 2004; 48:197-211.
14. Hsieh CH, Liu HT, Hsu SY, Hsieh HY, Chen YC. Motorcycle-related hospitalizations of the elderly. Biomed J 2017; 40:121-8. https://doi.org/10.1016/j.bj.2016.10.006
PMid:28521903 PMCid:PMC6138602
15. Warlick B, Nuismer A, Israel H, Cannada LK. The aging motorcyclist: a comparative epidemiologic study on pattern and severity of injury. J Trauma Acute Care Surg 2012; 73:175-8. https://doi.org/10.1097/TA.0b013e31824acc08
PMid:22743387
16. Chong S, Poulos R, Olivier J, Watson WL, Grzebieta R. Relative injury severity among vulnerable non-motorised road users: comparative analysis of injury arising from bicycle-motor vehicle and bicycle-pedestrian collisions. Accid Anal Prev 2010; 42:290-6. https://doi.org/10.1016/j.aap.2009.08.006
PMid:19887170
17. Cripton PA, Shen H, Brubacher JR, et al. Severity of urban cycling injuries and the relationship with personal, trip, route and crash characteristics: analyses using four severity metrics. BMJ Open 2015; 5:e006654. https://doi.org/10.1136/bmjopen-2014-006654
PMid:25564148 PMCid:PMC4289714
18. Lustenberger T, Inaba K, Talving P, et al. Bicyclists injured by automobiles: relationship of age to injury type and severity--a national trauma databank analysis. J Trauma 2010; 69:1120-5. https://doi.org/10.1097/TA.0b013e3181d0f68b
PMid:20526215
19. Rivara FP, Thompson DC, Thompson RS. Epidemiology of bicycle injuries and risk factors for serious injury. Inj Prev 1997; 3:110-4. https://doi.org/10.1136/ip.3.2.110
PMid:9213156 PMCid:PMC1067791
20. Liu HT, Rau CS, Liang CC, et al. Bicycle-related hospitalizations at a Taiwanese level I Trauma Center. BMC Public Health 2015; 15:722. https://doi.org/10.1186/s12889-015-2075-9
PMid:26219341 PMCid:PMC4517401
21. Pai CW, Chen YC, Lin HY, Chen PL. A population-based case-control study of hospitalisation due to head injuries among bicyclists and motorcyclists in Taiwan. BMJ Open 2017; 7:e018574. https://doi.org/10.1136/bmjopen-2017-018574
PMid:29122803 PMCid:PMC5695412
22. Pai CW, Lin HY, Tsai SH, Chen PL. Comparison of traffic-injury related hospitalisation between bicyclists and motorcyclists in Taiwan. PLoS One 2018; 13:e0191221. https://doi.org/10.1371/journal.pone.0191221
PMid:29342208 PMCid:PMC5771601
23. Davidson JA. Epidemiology and outcome of bicycle injuries presenting to an emergency department in the United Kingdom. Eur J Emerg Med 2005; 12:24-9. https://doi.org/10.1097/00063110-200502000-00007
PMid:15674081
24. Dinh MM, Kastelein C, Hopkins R, et al. Mechanisms, injuries and helmet use in cyclists presenting to an inner city emergency department. Emerg Med Australas 2015; 27:323-7. https://doi.org/10.1111/1742-6723.12407
PMid:25939667
25. Neumann MV, Eley R, Vallmuur K, Schuetz M. Current profile of cycling injuries: a retrospective analysis of a trauma centre level 1 in Queensland. Emerg Med Australas 2016; 28:90-5. https://doi.org/10.1111/1742-6723.12495
PMid:26607850
26. Gopinath B, Jagnoor J, Craig A, et al. Describing and comparing the characteristics of injured bicyclists and other injured road users: a prospective cohort study. BMC Public Health 2016; 16:324. https://doi.org/10.1186/s12889-016-2988-y
PMid:27074801 PMCid:PMC4831149
27. Chichom-Mefire A, Atashili J, Tsiagadigui JG, Fon-Awah C, Ngowe-Ngowe M. A prospective pilot cohort analysis of crash characteristics and pattern of injuries in riders and pillion passengers involved in motorcycle crashes in an urban area in Cameroon: lessons for prevention. BMC Public Health 2015; 15:915. https://doi.org/10.1186/s12889-015-2290-4
PMid:26384779 PMCid:PMC4575460
28. Tham KY, Seow E, Lau G. Pattern of injuries in helmeted motorcyclists in Singapore. Emerg Med J 2004; 21:478-82.
29. Meerding WJ, Looman CW, Essink-Bot ML, et al. Distribution and determinants of health and work status in a comprehensive population of injury patients. J Trauma 2004; 56:150-61. https://doi.org/10.1097/01.TA.0000062969.65847.8B
PMid:14749582
30. Polinder S, Haagsma J, Panneman M, et al. The economic burden of injury: health care and productivity costs of injuries in the Netherlands. Accid Anal Prev 2016; 93:92-100. https://doi.org/10.1016/j.aap.2016.04.003
PMid:27177394
31. Holbrook TL, Anderson JP, Sieber WJ, Browner D, Hoyt DB. Outcome after major trauma: discharge and 6-month follow-up results from the Trauma Recovery Project. J Trauma 1998; 45:315-24. https://doi.org/10.1097/00005373-199808000-00018
PMid:9715189
32. Holbrook TL, Anderson JP, Sieber WJ, Browner D, Hoyt DB. Outcome after major trauma: 12-month and 18-month follow-up results from the Trauma Recovery Project. J Trauma 1999; 46:765-73. https://doi.org/10.1097/00005373-199905000-00003
PMid:10338392
33. Doyle D, Muir M, Chinn B. Motorcycle accidents in Strathclyde Region, Scotland during 1992: a study of the injuries sustained. Health Bull (Edinb) 1995; 53:386-94.