

Dear Sir,
Persimmons contain large amounts of soluble tannin, which may interact with gastric acid to form a conglomerate that is harder than other phytobezoars.(1) The presence of ingestible fruit tannins, cellulose, hemicellulose and lignins in persimmons make such a phytobezoar more difficult to dissolve or segment into smaller divisions due to its hard consistency.(2) This makes persimmon phytobezoars particularly difficult to manage. We report a case of multiple persimmon phytobezoars causing simultaneous small bowel and gastric outlet obstruction.
A 39-year-old woman was admitted to our hospital with symptoms of nausea, vomiting and epigastric pain. She had no past medical illness. On examination, she had a distended abdomen without scars and no external hernias. Blood investigations and imaging established a diagnosis of intestinal obstruction. Computed tomography established a diagnosis of small bowel intestinal obstruction with grossly distended stomach. There was no reporting of ‘bezoar’ by the on-duty radiologist. However, the surgical team adjudged the possibility of an intraluminal mass in the distal bowel and retrospectively asked the patient about her dietary history. She confirmed that she had eaten four persimmons from her own farm ten days ago. A clinical diagnosis of small bowel obstruction secondary to persimmon phytobezoar was established.
A 5-cm phytobezoar obstruction in the distal small bowel was retrieved through an enterotomy with primary repair. Another 15 cm × 6 cm sausage-shaped phytobezoar was retrieved from the stomach through a gastrotomy and primary repair (
Fig. 1
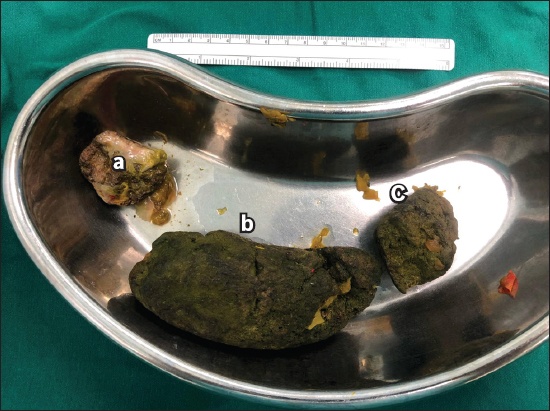
Photograph shows gross specimens of a 5-cm phytobezoar obstruction in the distal small bowel retrieved through an enterotomy and primary repair (a & c). Another 15 cm × 6 cm sausage-shaped phytobezoar (b) was also imaged and retrieved from the stomach via gastrotomy and primary repair.
Old age, poor dentition, previous gastrectomy, diabetes mellitus and hypothyroidism can increase the risk of bezoar formation due to problems with digestion or gut motility. The clinical manifestation of the bezoar is dependent on the location of the obstruction. Small bowel obstruction is the most common manifestation. The majority of phytobezoars pass spontaneously (80%–90%); some can be retrieved through an endoscopy (10%–20%) and surgery is rarely needed (< 1%).(3,4) Recently, the use of effervescent aerated drinks such as Coca-Cola has been reported in the management of phytobezoars.(5) This is an attractive management option, as it avoids surgical intervention and its resultant morbidity. However, there is an increased risk of the occurrence of secondary ‘daughter’ phytobezoars.
In our patient, endoscopy and Coca-Cola were not advocated due to her small bowel obstruction. In patients with multiple bezoars causing intestinal obstruction, laparotomy is considered more effective to concurrently remove all the bezoars. One should also check for the possibility of more bezoars to avoid early recurrent obstruction from the ‘missed’ bezoars. Laparoscopic surgery is an option when the expertise is available, but we caution against this approach, as potential concurrent bezoars can be missed due to loss of tactile feedback.
Yours sincerely,