

CASE 1 CLINICAL PRESENTATION
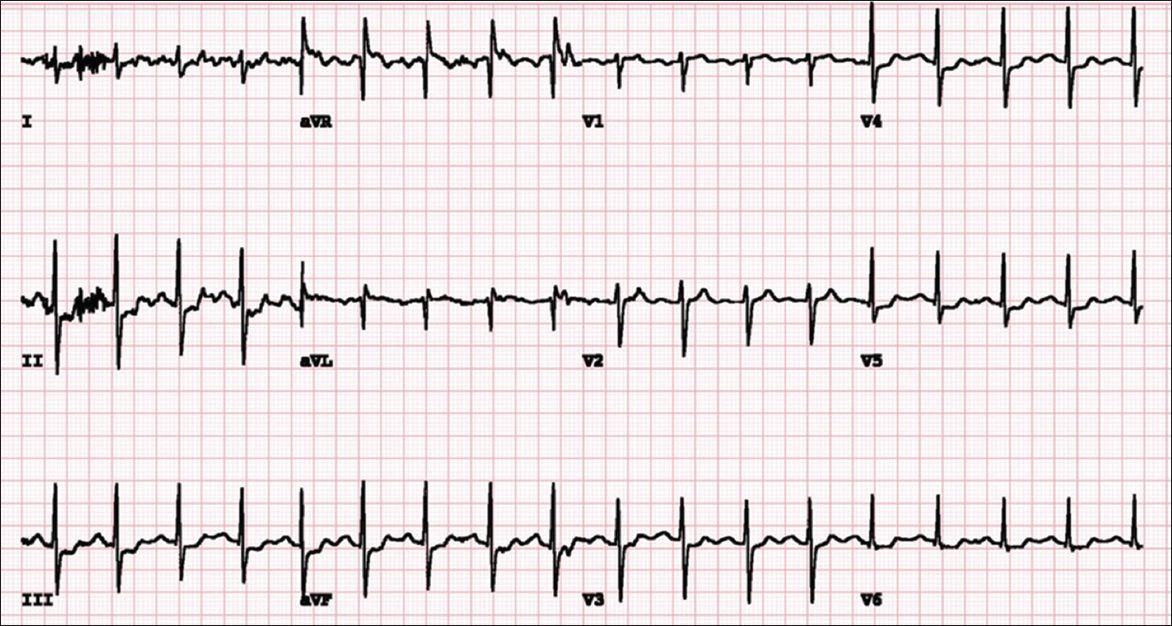
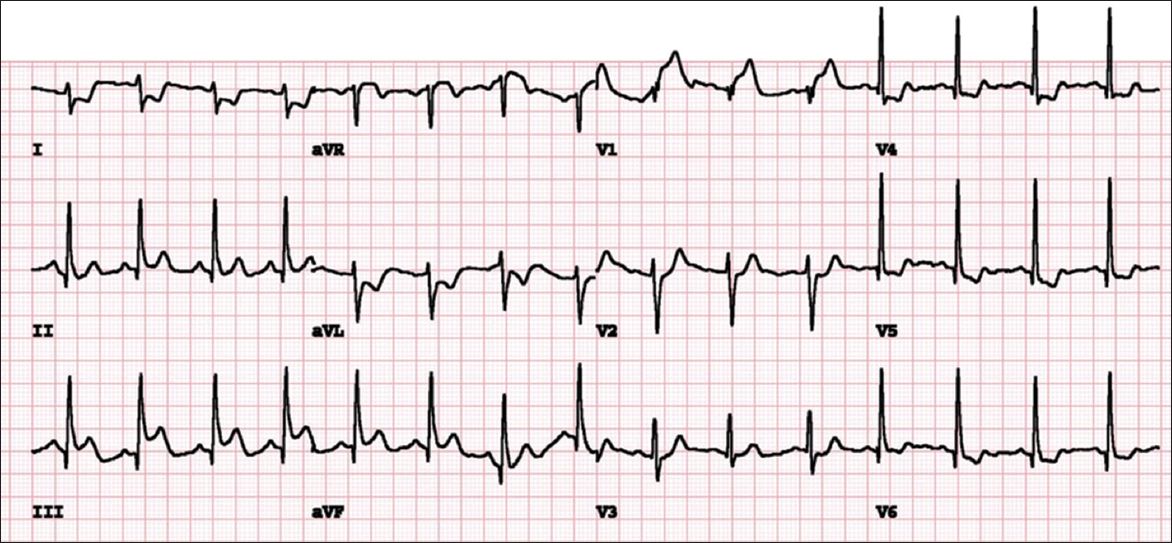
A 62-year-old woman presented with atypical angina for the past three months. Her past medical history includes hyperlipidaemia. Electrocardiography (ECG) performed at rest shows normal sinus rhythm. The patient underwent treadmill ECG stress test, and her ECG at highest heart rate during the treadmill stress test is shown in
Fig. 1
ECG at peak stress during treadmill ECG stress test.
ECG STRESS TEST INTERPRETATION
The test was terminated at Stage 2 of the Bruce protocol with seven Metabolic Equivalents of Tasks (METs) of work due to reports of chest pain and breathlessness. The patient could not achieve the target heart rate of 135 beats per minute (bpm). ECG performed at her highest heart rate (
CLINICAL COURSE
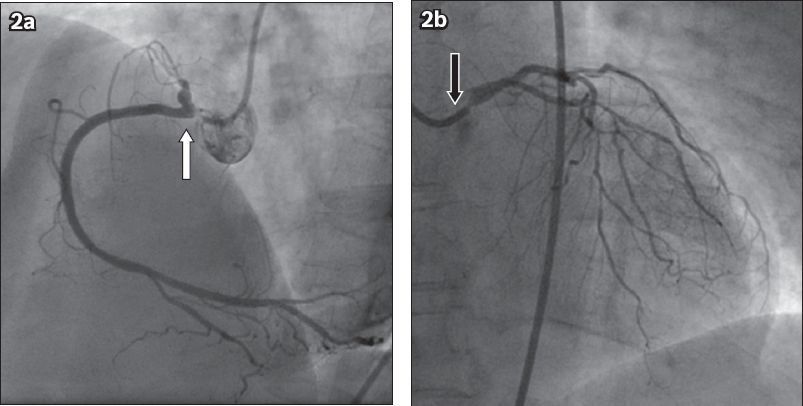
In view of her symptoms and abnormal treadmill ECG stress test, the patient underwent coronary angiography, which showed severe left main and triple vessel disease. She had 90% ostial left main stenosis, severe diffuse distal disease in the left anterior descending (LAD) and circumflex arteries, as well as 90% ostial right coronary artery (RCA) stenosis with 70% stenosis in the posterior descending artery (
Fig. 2
Coronary angiograms show (a) 90% stenosis in the ostium of the right coronary artery (white arrow) in the left anterior oblique view; and (b) 90% stenosis in the ostium of the left main coronary artery (black arrow) with diffuse disease in the left anterior descending and left circumflex artery in the right anterior oblique cranial view.
CASE 2 CLINICAL PRESENTATION
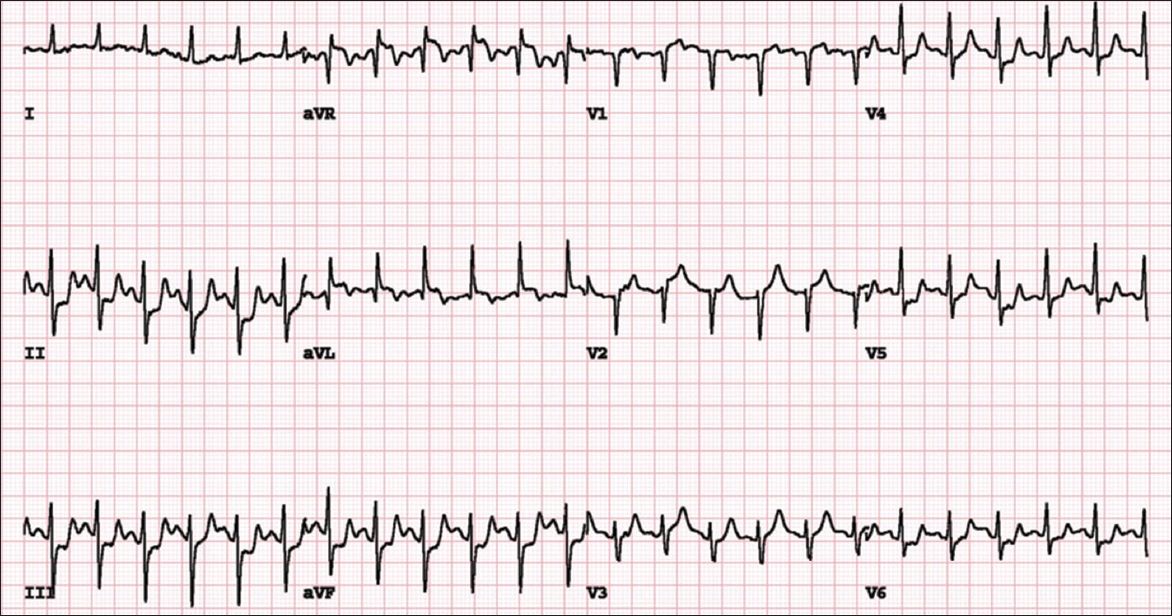
A 51-year-old man was referred for treadmill ECG stress test due to breathlessness on exertion. He had a previous anterior ST-elevation myocardial infarction in the year 2005 and primary percutaneous intervention to his proximal LAD coronary artery. The patient’s medical history also included diabetes mellitus and dyslipidaemia. ECG done at rest shows Q waves in the anterior lead V1–2, consistent with a previous anterior myocardial infarction. The patient underwent treadmill ECG stress test. The ECG in
Fig. 3
ECG at peak stress during treadmill ECG stress test.
ECG STRESS TEST INTERPRETATION
The patient achieved Stage 4 of the Bruce protocol, exercising for a total of nine minutes 46 seconds with 11.2 METs of work. ECG at peak stress showed sinus tachycardia at a rate of 146 bpm. There were new horizontal and up-sloping ST-segment depressions in leads II, III, aVF and V4–6, which were suggestive of myocardial ischaemia. In addition, there was an isolated 1-mm ST-segment elevation in lead aVL. The ST segments returned to baseline at five minutes of recovery.
CLINICAL COURSE
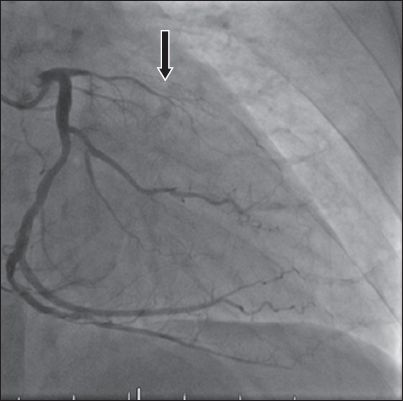
The patient subsequently underwent coronary angiography, which showed total occlusion in the ostial LAD artery, with further 90% stenosis in the left posterior descending artery (LPDA) (
Fig. 4
Coronary angiogram shows total occlusion of the ostial left anterior descending artery in the right anterior oblique caudal view. The occluded left anterior descending stent is also seen (arrow).
CASE 3 CLINICAL PRESENTATION
A 61-year-old man presented with a one-week history of angina. He had a history of hypertension and dyslipidaemia. The patient underwent myocardial perfusion treadmill ECG stress test. ECG at rest showed normal sinus rhythm.
Fig. 5
ECG done immediately after peak stress.
ECG STRESS TEST INTERPRETATION1
ECG performed immediately after achieving target heart rate (
CLINICAL COURSE
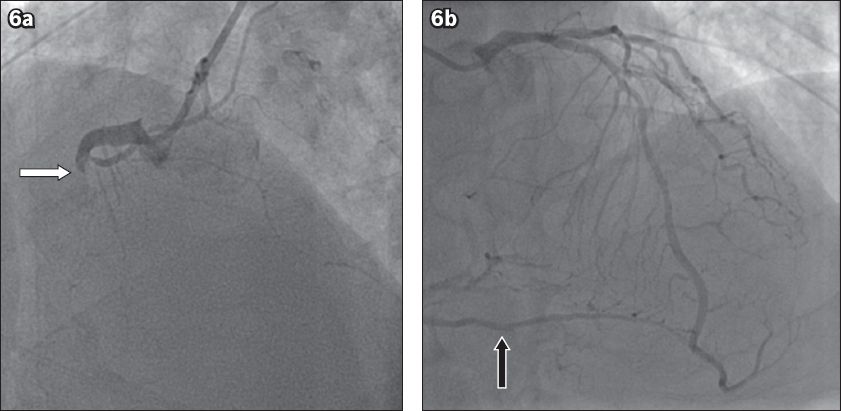
The patient’s myocardial perfusion images showed a reversible perfusion defect in the mid-to-basal inferior wall, which is suspicious of obstructive CAD in the RCA territory. His coronary angiogram showed total occlusion of the proximal RCA, with Rentrop Grade 2 collaterals from the left coronary arteries to the distal RCA (
Fig. 6
Coronary angiogram shows (a) 100% occlusion of the proximal right coronary artery (white arrow) in the left anterior oblique cranial view; and (b) collateral from the left coronary arteries (black arrow) in the left anterior oblique cranial view.
DISCUSSION
Treadmill ECG stress test
In 2014, ischaemic heart disease (IHD) was the third leading cause of death in Singapore, accounting for 16% of total deaths.(1) There is a need for early identification and improved treatment of IHD. The treadmill ECG stress test is commonly used as a screening test to identify myocardial ischaemia. During exercise, limitation of coronary blood flow due to obstructive CAD may lead to myocardial ischaemia and its subsequent ECG changes. This is the basis of detecting significant CAD on the treadmill ECG stress test. In addition, the treadmill ECG stress test is also frequently used to assess for chronotropic response to exercise, exercise-induced arrhythmia and evaluation of symptoms during exercise, as well as the individual’s exercise capacity. The sensitivity of the treadmill ECG stress test in diagnosing obstructive CAD was approximately 50%, with a specificity of approximately 90%.(2)
Indications for the treadmill ECG stress test
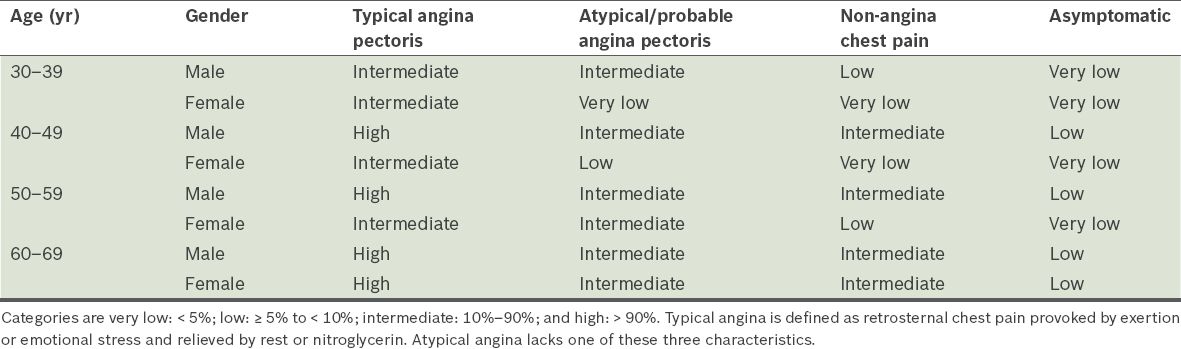
The American Heart Association previously published a guideline recommending stress tests for adult patients with intermediate pretest probability of CAD.(3)
Table I
Pretest probability of coronary artery disease based on age, gender and presenting symptoms.(3)
The Ministry of Health, Singapore, published its own guidelines on screening for cardiovascular disease.(4) In addition to evaluating symptomatic patients with intermediate pretest probability, the guidelines also recommended the treadmill ECG stress test for the detection of CAD in the following groups: (a) asymptomatic individuals with multiple risk factors; (b) asymptomatic men above 45 years of age and women above 55 years of age who are planning to start vigorous exercise; (c) individuals in occupations in which impairment may affect public safety (e.g. pilots); (d) individuals at high risk of coronary artery disease due to comorbidities; and (e) patients with diabetes mellitus who are planning to start vigorous exercise.
Patients whose baseline ECG shows more than 1-mm ST-depression or less than 1-mm ST-depression, and who are taking digoxin or fulfil the ECG criteria for left ventricular hypertrophy, electronically paced ventricular rhythm or complete left bundle branch block were considered not suitable for evaluation using the treadmill ECG stress test alone, as it would be difficult to interpret any changes in the ST segment during the test.
Performing the treadmill ECG stress test
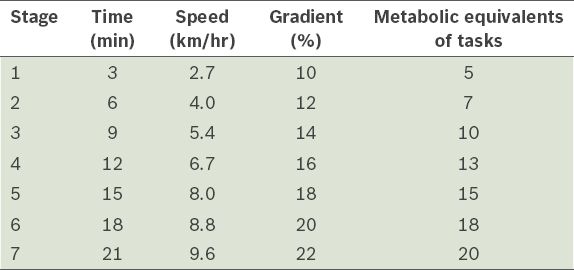
The Bruce protocol is the most commonly used exercise treadmill stress protocol. It consists of a total of seven stages, with a gradual increment in the speed and gradient of the treadmill. Each stage lasts three minutes to allow the patient to acclimatise to the specific speed and gradient before advancing to the next stage. Exercise intensity during the treadmill ECG stress test is calculated in METs, which reflect the amount of oxygen consumed per minute. 1 MET is equal to 3.5 mL/min/kg of oxygen used. Watching television, for example, requires 1 MET, while brisk walking requires 4 METs.
Prior to starting the Bruce protocol, ECG may be performed with the patient hyperventilating in the standing position to assess for any ST-segment changes caused by hyperventilation. The MET value increases as the patient advances to higher stages of the Bruce protocol.
Table II
Characteristics of each stage of the Bruce protocol.
Contraindications for exercise stress test
As with any investigation, it is important to ensure the safety of the patient undergoing the test, since the treadmill ECG stress test could be harmful to the patient in certain situations. Each laboratory has its own protocol regarding the safety and suitability of the patients undergoing such tests.
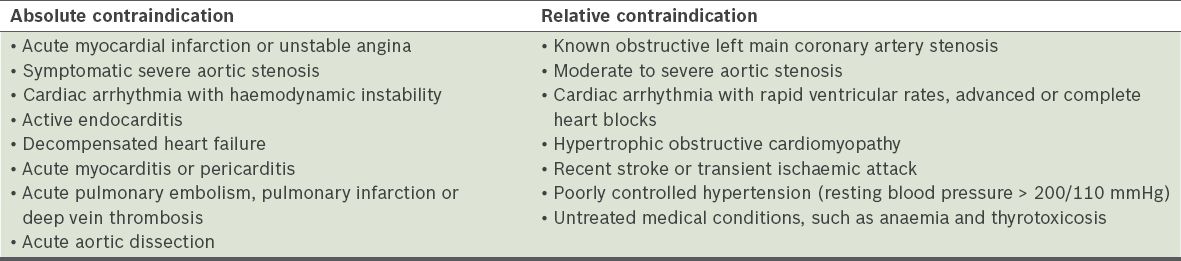
Table IV
Main contraindications for exercise stress test.
Heart rate response
During exercise, the physiological increase in heart rate is due to a decrease in vagal tone followed by an increase in sympathetic tone. This, in turn, leads to increased oxygen supply to the vital organs in the body. However, the maximal heart rate achievable during exercise is heavily influenced by age. Most laboratories worldwide use a simple equation to predict the maximum heart rate: Maximum predicted heart rate = 220 – age in years.
Traditionally, sufficient effort during treadmill ECG stress testing is defined as achieving 85% of the age-predicted maximal heart rate. However, some studies have reported a significant variability in the maximum predicted heart rate among people of identical ages;(5,6) hence, this may not be used in isolation as a termination criterion. In addition to the evaluation of CAD, the treadmill ECG stress test is also often used to evaluate for chronotropic incompetency, in which the patient is unable to mount an adequate heart rate response to exercise, leading to symptoms such as effort-related dyspnoea and lethargy.
Blood pressure response
The increase in sympathetic tone and vasodilation during exercise generally causes a rise in blood pressure. A drop in systolic blood pressure > 10 mmHg is an indication to terminate the treadmill ECG stress tests, as it could be due to myocardial ischaemia leading to left ventricular dysfunction. This often signifies severe multi-vessel CAD, especially if there are accompanying symptoms and/or ST changes on the ECG. An exaggerated blood pressure response, defined as a peak systolic blood pressure of > 210 mmHg in men and > 190 mmHg in women according to the Framingham criteria,(7) was shown to predict the risk of hypertension in normotensive individuals.(8)
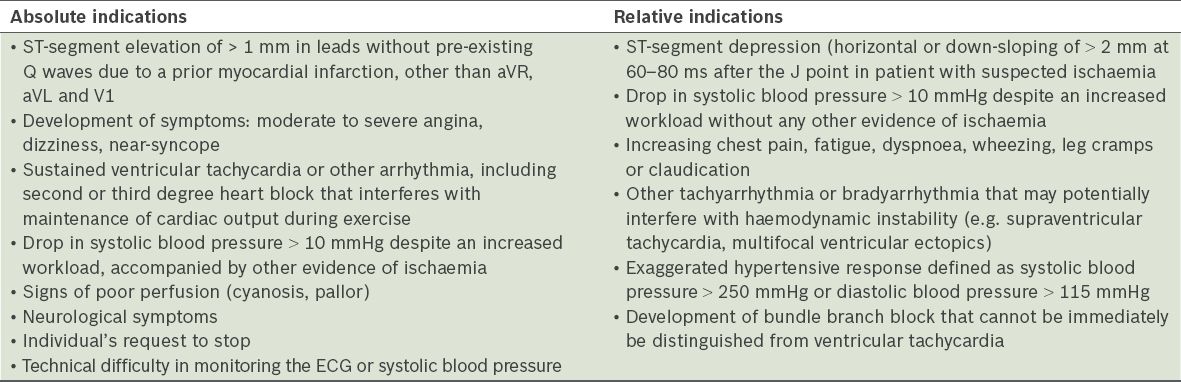
Indications for termination of the treadmill ECG stress test
In addition to achieving 85% of the age-predicted maximal heart rate, other indications for the termination of a treadmill ECG stress test are shown in
Interpretation of the treadmill ECG stress test
ST-segment changes indicative of obstructive CAD
A treadmill ECG stress test is considered abnormal when there is a horizontal or down-sloping ST-segment depression ≥ 1 mm at 60–80 ms after the J point.(9) Exercise ECGs with up-sloping ST-segment depressions are typically reported as an ‘equivocal’ test. In general, the occurrence of horizontal or down-sloping ST-segment depression at a lower workload (calculated in METs) or heart rate indicates a worse prognosis and higher likelihood of multi-vessel disease. The duration of ST-segment depression is also important, as prolonged recovery after peak stress is consistent with a positive treadmill ECG stress test. Another finding that is highly indicative of significant CAD is the occurrence of ST-segment elevation > 1 mm (often suggesting transmural ischaemia); these patients are frequently referred urgently for coronary angiography.
In Case 1, the patient had an abnormal treadmill ECG stress test with mild horizontal and down-sloping ST depression in the inferior-lateral leads at Stage 2 (low workload) of the Bruce protocol. In addition to being electrically positive, the test was also subjectively positive, with the patient reporting chest pain with exercise stress. These are highly suggestive of obstructive CAD, as proven in the subsequent coronary angiogram. Case 2 illustrated the use of the treadmill ECG stress test in a patient with a previous history of anterior myocardial infarction; the ST-segment depressions were seen not only at maximal heart rate, but also during the recovery period, indicating significant ischaemia. While ST-segment depression in the inferolateral leads during the treadmill ECG stress test indicates ischaemia from obstructive CAD, we cannot identify the diseased coronary artery from the ST-segment depression alone. However, as shown in Case 3, the ST-segment elevation during the treadmill ECG stress test can be used to identify the culprit coronary artery (where the stenosis causing ischaemia was located), which in this case was the RCA. Other possible causes of ST-segment elevation during the treadmill ECG stress test are coronary artery spasm and the presence of existing Q waves due to previous myocardial infarction.
In conclusion, the treadmill stress ECG test is a reliable screening test for obstructive CAD, especially in patients with an intermediate pretest probability. It is readily available in many centres in Singapore.
SMJ-57-353.pdf