

Dear Sir,
Astroblastomas are extremely rare primary glial tumours. A majority of reports have described their tendency to develop in the paediatric population(1,2) and cerebral hemispheres.(1) We report a unique case of intraventricular astroblastoma. In view of the paucity of disease knowledge on astroblastomas, this case is highlighted together with the relevant literature.
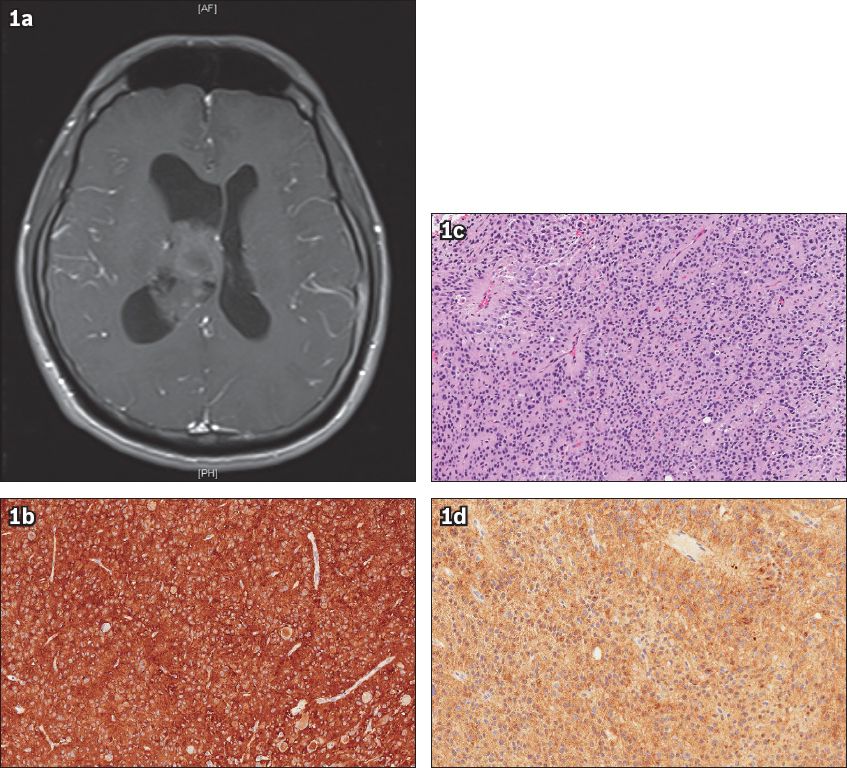
A 35-year-old man presented with left-sided upper and lower limb numbness and weakness. Postcontrast T1-weighted magnetic resonance imaging showed a lobulated, heterogeneous mass in the brain, centred in the body of the right lateral ventricle and measuring 5.0 cm × 2.6 cm × 2.3 cm. The mass formed a broad base with the septum pellucidum and medial wall of the lateral ventricle, with a component extending into the third ventricle via the foramen of Monro (
Fig. 1
(a) Axial T1 postcontrast MR image shows a mass with mixed signal intensity, centred in the body of the right lateral ventricle. (b) Photomicrograph shows tumour tissue composed of cells arranged in sheets (Haematoxylin & eosin, × 200). Scattered perivascular pseudorosettes are observed within the sheets of cells. The cell nuclei surrounding the central vessels are oriented away from the vessels. No definite ependymal rosettes or canals are seen. Mitotic rate is less than one per ten high power fields. No necrosis or microvascular proliferation is identified. (c) Photomicrograph shows diffuse strong immunostaining for glial fibrillary acid (GFAP) protein, a glial marker (GFAP, × 200). (d) Photomicrograph shows diffuse moderate staining for synaptophysin, a neuronal marker (synaptophysin, × 200).
Astroblastomas account for an estimated 0.45%–2.80% of primary brain tumours such as gliomas.(3) The World Health Organization’s classification places astroblastomas in the category of ‘Other neuroepithelial tumours’.(4) The origin of these tumours has been debated, as they share features of astrocytomas and ependymomas.(1) Typical histopathological features include perivascular pseudorosettes, typically made up of neoplastic epithelial elements. The presence of pseudorosettes makes distinguishing between astroblastomas and ependymomas challenging.(5) Other distinguishing features include absent fibrillar patterns, rarefied spaces between pseudorosettes, hyalinised vessels and thick perivascular cytoplasmic processes.(3) On imaging, astroblastomas are often visualised as a well-demarcated, heterogeneous, lobulated and/or cystic mass in the cerebral hemispheres.(1)
Owing to the rarity of astroblastomas, there is no established treatment for their management. The current consensus is that surgical treatment is essential. The goal of total resection is validated by logical considerations; the tumour is usually well-demarcated with non-infiltrative features. However, the role of adjuvant therapy is less defined. The number of large studies is presently insufficient to reaffirm its use as part of routine treatment.
In conclusion, this article describes a unique case of an intraventricular astroblastoma in an adult. To establish a future standard of care, the authors advocate the need for molecular studies to comprehend the properties of this unusual neoplasm.
Yours sincerely,
ACKNOWLEDGEMENT
The authors would like to thank Professor Gregory Fuller of the Department of Pathology, MD Anderson Cancer Centre, Houston, Texas, USA, for his expert opinion on the histopathology findings from the patient’s surgery.