

Abstract
One in three community-dwelling elderly aged ≥ 65 years and one in two aged > 80 years will have at least one fall within a year. Many elderly people are ‘silent fallers’ who do not report the fall nor seek medical assistance unless they are injured. In Singapore, falls account for 40% of injury-related deaths. Unaddressed risk factors for falls lead to recurrent falls and poor quality of life. Elderly people who have experienced falls and near falls can have a fear of falling, post-fall anxiety syndrome, depression and reduction in activities, with a negative impact on their well-being. Primary care doctors can screen and optimise modifiable risk factors such as poor vision, balance, poor gait, motor weakness, joint disorders, psychotropic drugs, sedatives, anti-hypertension medications, choice of footwear and environment factors. Timely referrals for cataract operations, balance and strengthening exercises, and osteoporosis treatment can reduce the risk of falls and injurious outcomes.
Roger brought his 68-year-old mother, Amber, to your clinic for a consultation, as he was concerned that she was becoming more withdrawn and isolated. You have been their family doctor for the last decade. Amber opened up to share that she has been fearful of falling since her bad fall six months ago in the shower. She had restricted her own activities and made up excuses to avoid leaving her home even when family and friends invited her to join them.
WHAT IS AN UNINTENTIONAL FALL AND A LONG LIE?
An unintentional fall is an event that results in a person inadvertently coming to rest on the ground or at a lower level from causes other than sustaining a violent blow, loss of consciousness or sudden onset of paralysis as may occur during a stroke or epileptic seizure.(1)
A long lie is defined as an inability to get up from a fallen position, usually on the floor or ground, for more than an hour. It is associated with complications such as rhabdomyolysis, fear of falling, pneumonia, pressure sores and dehydration.(2) Long lie is a marker of weakness, illness and isolation, and is associated with higher mortality rates.(3) Only 50% of fallers are able to get up from the ground or floor after a fall.(4)
WHAT HAPPENS TO FALLERS?
A fall that is not addressed may lead to recurrent falls.(5) 30% of fallers will fall again. Recurrent falls are defined as more than two falls in a year and are rarely attributable to a ‘mechanical’ (i.e. accidental) cause. The elderly usually fall due to a medical problem or risk factors that are modifiable. Falls are associated with a fear of falling. Fear of falling can happen even with a near-fall experience and is associated with self-inflicted reduction in activity or function, anxiety and even depression. This is also known as post-fall anxiety syndrome and is more common in older persons living alone, those with cognitive and mobility impairments, poor balance and history of falls. It is a risk factor for further falls.(6)
The most common modifiable risk factors for falls are poor balance and gait, medications (e.g. sedatives and antipsychotics), weakness (associated with medical conditions such as Parkinson’s and stroke disease), joint disorders (e.g. osteoarthritis of the knees), impaired cognition resulting in poor safety awareness, poor vision (commonly from cataracts), environmental causes and inappropriate footwear. Recurrent falls are usually due to multiple factors.(7,8)
Falls due to syncope need to be assessed separately, as many studies consider falls and syncopal falls to be two separate diagnoses with two separate aetiologies.(9) Common causes for syncopal falls include cardiac arrhythmias, neurally mediated syncope, orthostatic hypotension and carotid sinus syndrome.(10)
HOW COMMON IS THIS IN MY PRACTICE?
One in every three community-dwelling elderly persons aged 65 years and above have at least one fall within a year.(11) The ratio increases to one in every two for those above 80 years of age.(12) Episodes of falls are often accepted as part of ageing by both the patient and family members. Many elderly are ‘silent fallers’ who do not report the fall and fail to seek medical assistance unless injured. In Singapore, falls are a leading cause of injury among older adults. According to the National Registry of Diseases Office, Singapore, the crude incidence rate of unintentional falls in 2012 was 277.7 per 100,000 for adults aged 60 years and older.(13) Falls account for 40% of injury-related deaths.(14) The elderly population is increasing exponentially, and one in three individuals will be above 65 years of age by 2020.(15) Hence, the number of fallers and ‘silent fallers’ will only increase in Singapore.
Falls can lead to serious consequences such as fractures, head injuries, reduced mobility, premature long-term care admissions and even death. In Singapore, falls account for 85% of all cases of elderly patients with trauma seen at the emergency department, according to the SAFE (Steps to Avoid Falls in the Elderly) study.(16) Although most falls do not result in significant injury, the psychological effect of the fear of falling may cause anxiety, self-imposed activity restriction, social isolation, depression, and other negative effects on well-being and quality of life. If not properly addressed, the cycle of falls may set in (
Fig 1
Chart shows the cycle of falls.
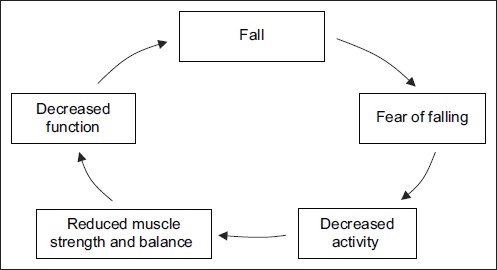
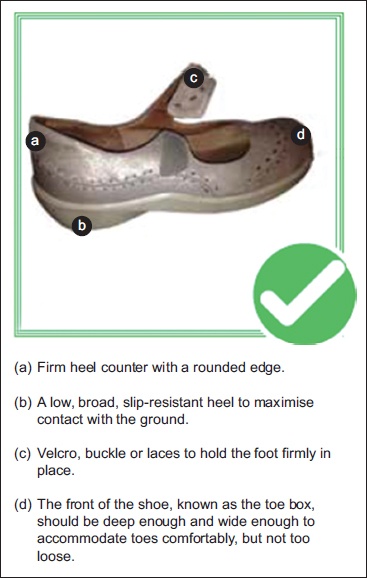
Fig 2
Diagram shows the components of proper footwear to reduce the chance of falls.
HOW RELEVANT IS THIS TO MY PRACTICE?
Primary care practitioners are often the first point of contact for many patients. With an ageing population, a greater proportion of elderly will be managed in the primary healthcare setting, presenting physicians with the opportunity to identify, assess and intervene for falls prevention.
‘Silent fallers’ will usually brush off incidents of falls as part and parcel of ageing, but they may visit a primary care practitioner for pain or injury related to a fall. A scrape on the knee or a bruise on the elbow can be an opening to screen for falls. As many patients do not volunteer information on falls, all older persons above 65 years should be screened for a fall or problems with gait and balance. Failure to adequately address a previous fall can result in a 30% increased chance of the individual falling again.(18) Therefore, adopting a proactive approach to ask about falls, near falls and fear of falling can help us to identify and mitigate any modifiable risks before the next fall.
A fall assessment should be integrated into annual reviews for older patients who are on long-term follow-up in primary care for their chronic medical conditions.
WHAT CAN I DO IN MY PRACTICE?
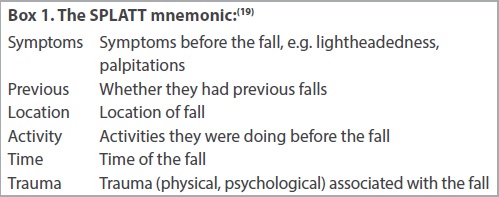
During history taking, ask about a history of previous falls as it is an independent predictor of future falls. The fall event can be described in more detail by using the SPLATT mnemonic(19) (
A focused history includes: (a) pre fall (activity the patient was doing before the fall, any other symptoms prior to falling); (b) during the fall (what happened during the fall, how the patient landed); and (c) post fall (any post-fall syncope, drowsiness or long lie of more than an hour).
Next, do a medication review. Identify precipitating (e.g. acute medical problems) and predisposing factors, consisting of extrinsic causes (e.g. environment, footwear) and intrinsic causes (e.g. poor vision, poor balance and gait due to stroke/Parkinsonism/joint abnormalities, poor cognition). Assess for complications from the fall such as fractures, head injury, skin lacerations, long lie complications, fear of falling.(2,8)
In the physical examination, pay particular attention to the patient’s (a) gait and balance; (b) visual acuity (may want to also consider visual field assessment because conditions such as glaucoma and macular degeneration can adversely affect visual fields and result in an increased risk of falls as well); (c) neurological and cardiovascular systems; (d) postural blood pressure; and (e) screen for any injuries sustained.
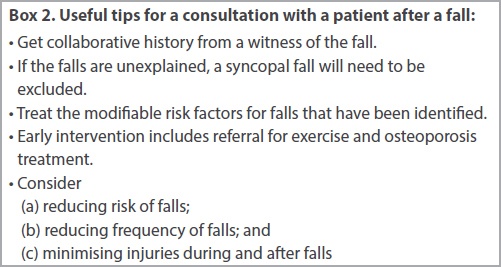
Postural or orthostatic hypotension is diagnosed when, within 2–5 minutes of quiet standing (after a five-minute period of supine rest), one or both of the following is present: ≥ 20 mmHg drop in systolic pressure and/or ≥ 10 mmHg drop in diastolic pressure. The heart rate normally rises immediately on standing. Investigations to be undertaken include basic blood tests to screen for precipitating causes of falls, such as full blood count, renal panel, C-reactive protein, calcium and vitamin D level for bone health screening; and electrocardiography (if suspicious of a syncopal/cardiac cause for the fall).(20-23) Useful tips for the consultation are shown in
Box 2
Useful tips for a consultation with a patient after a fall:
Interventions
There is good research evidence that a number of single interventions can reduce falls and injuries. These interventions can be in the clinic or home setting and target the risk factors shown in Tables
Table I
Risk factors and possible interventions in the clinic setting.
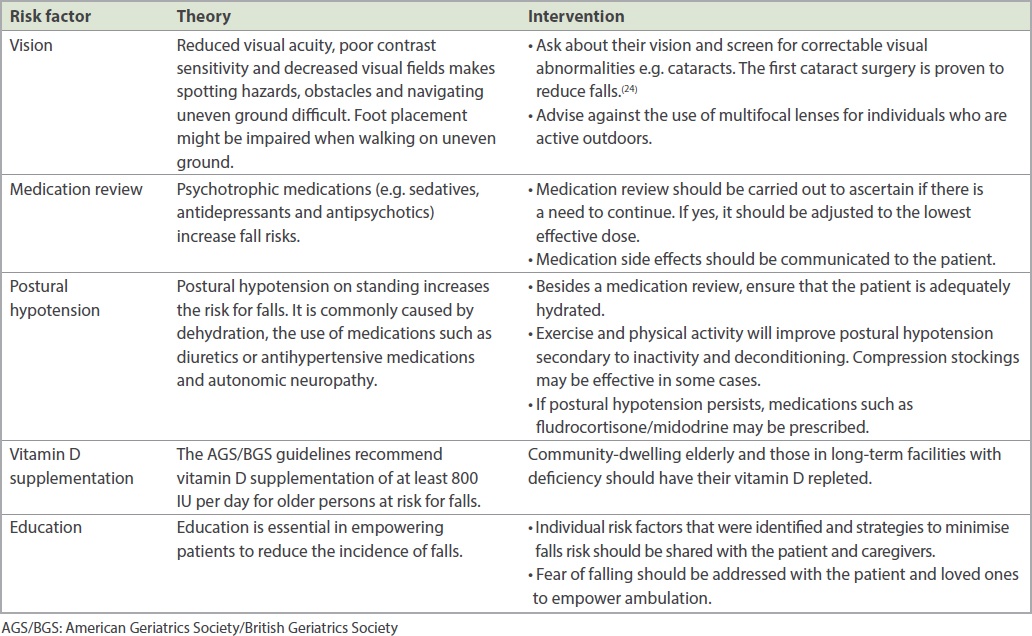
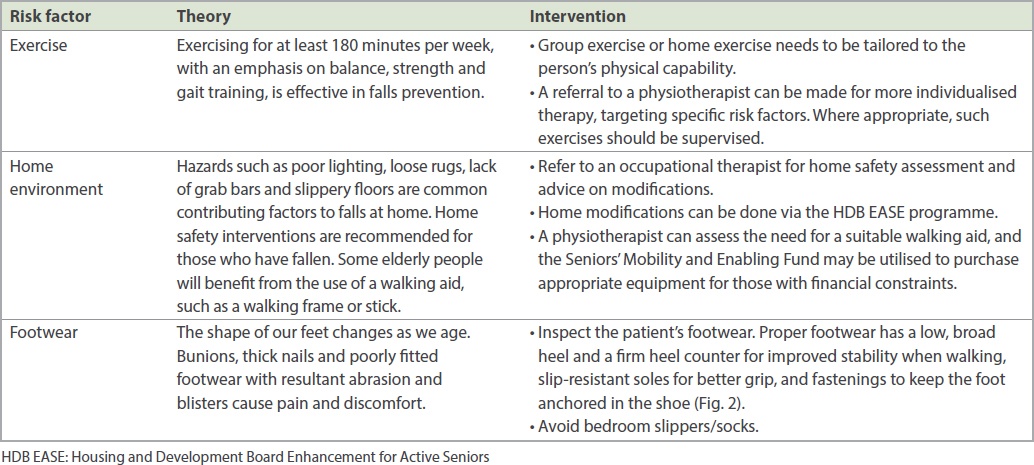
Table II
Risk factors and possible interventions in the home setting
Targeted multifactorial interventions based on falls risk assessments have been shown to be effective, particularly in the high-risk falls group and those with a previous history of falls.(25) A common pitfall for falls assessment is the failure to address bone health. The Osteoporosis Self-assessment Tool for Asians is a simple tool to screen for osteoporosis.(26)
Falls are preventable and the risk of injurious falls can be reduced if risk factors are identified early and there is timely introduction of appropriate interventions.
WHEN SHOULD I REFER TO A SPECIALIST?
If there is clear history of a loss of consciousness, a work-up for possible causes of syncope needs to be carried out. Diagnoses of carotid sinus hypersensitivity and tachyarrhythmias/bradyarrhythmias also need to be considered. Implantation of a permanent pacemaker may be beneficial for this group of patients. For patients with recurrent falls, a referral to a falls clinic at a hospital would allow a multidisciplinary assessment and a tailored multicomponent intervention to be performed to target pertinent risk factors.
USEFUL LINKS
-
Housing and Development Board’s Enhancement for Active Seniors programme:
https://www.hdb.gov.sg/cs/infoweb/residential/living-in-an-hdb-flat/for-our-seniors/ease (accessed January 1, 2020) -
Prevention of Falls Network Earth:
http://profane.co (accessed June 1, 2019) -
Changi General Hospital’s No Falls Programme:
https://www.cgh.com.sg/nofalls/ (accessed January 1, 2020) -
Fall prevention exercises (accessed January 1, 2020)
– Introduction: https://vimeo.com/48017706
– Strengthening: https://vimeo.com/48014858
– Balancing: https://vimeo.com/48014859
– Cool down/conclude: https://vimeo.com/48016508 -
Fall recovery (accessed January 1, 2020)
– What to do after a fall (alone): https://vimeo.com/47986154
– What to do after a fall with help from someone: https://vimeo.com/47987342
TAKE HOME MESSAGES
-
Falls and ‘silent falls’ are common and under-recognised in our community.
-
Falls with risk factors that are not addressed will lead to recurrent falls and poor quality of life.
-
Falls and near falls can result in fear of falling, post-fall anxiety syndrome, depression and reduction in activities, with a negative impact on general well-being.
-
Modifiable risks include poor vision, balance, poor gait, motor weakness, joint disorders, psychotropic drugs, sedatives, anti-hypertension medications, choice of footwear and environment factors.
-
Timely referrals for cataract operations, balance and strengthening exercises, and osteoporosis treatment can reduce the risk of falls and injurious outcomes.
You reviewed Amber six months after her son brought her to you. She walked in by herself this time and reported that she had regained her confidence and independence after the cataract surgery you had referred her for. Earlier, she had also heeded your advice to stop wearing her fluffy bedroom slippers, which could have caused her falls. You noted no side effects from her biphosphonates and reminded her to be careful, as she had started taking the bus again to visit her grandchildren.
SMJ-61-116.pdf