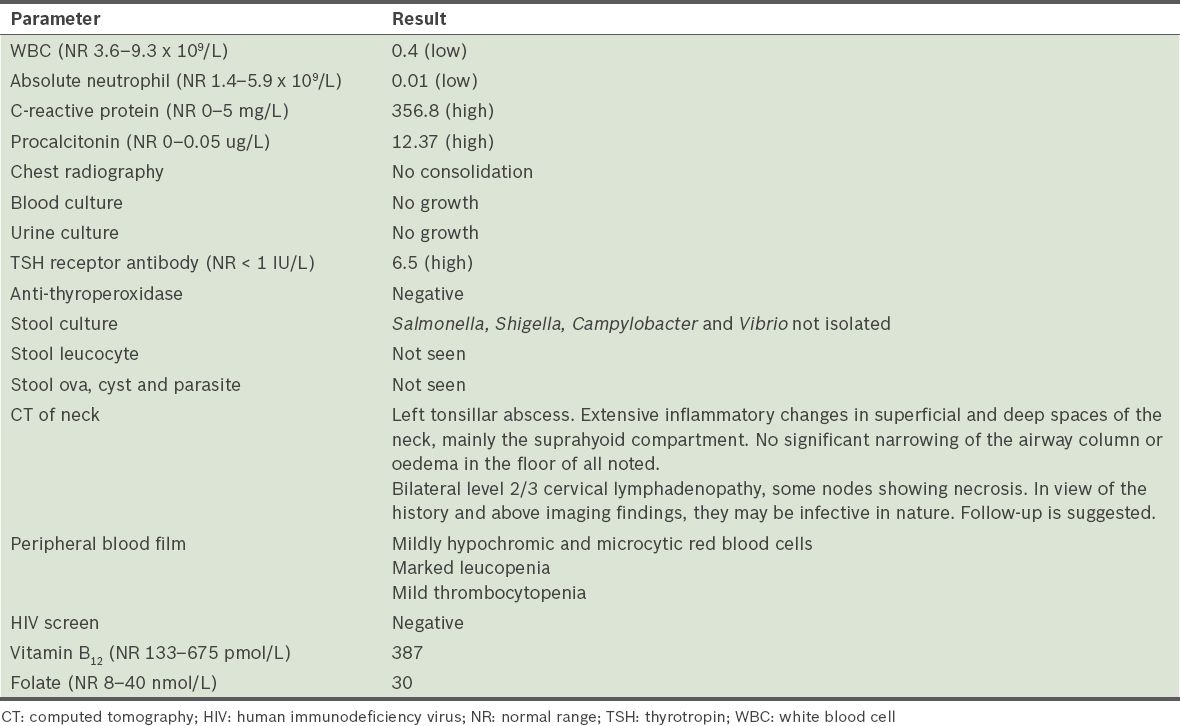
A 36-year-old Chinese woman presented to our hospital with two days of fever associated with diarrhoea and sore throat. She had been diagnosed with Graves’ disease one month prior to presentation and had been taking carbimazole 30 mg daily from the time of diagnosis. The patient had leucopenia neutropenia, and elevated C-reactive protein and procalcitonin. Computed tomography of the neck showed tonsillar abscess (Table I). The patient completed two weeks of piperacillin/tazobactam followed by three weeks of oral amoxicillin/clavulanic acid. The abscess resolved during the otorhinolaryngology follow-up.
Table I
Laboratory test results.
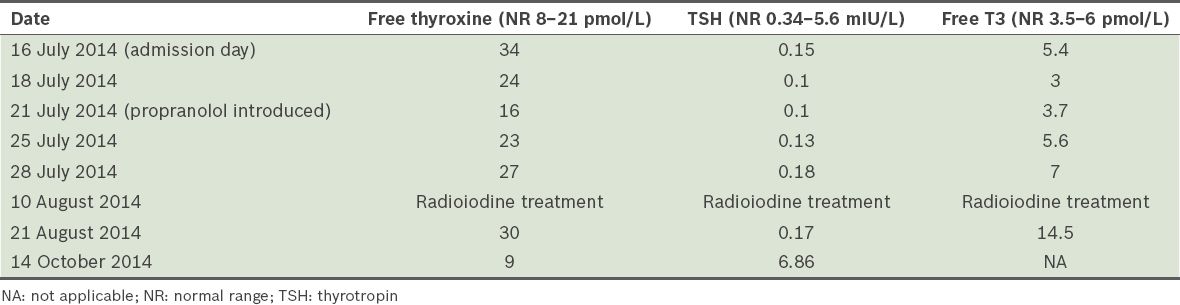
Thyroid function test showed primary hyperthyroidism. Due to the patient’s borderline blood pressure, beta blockers were not administered. Thionamides were contraindicated due to agranulocytosis. Cholestyramine 4 g every six hours was used to treat hyperthyroidism. Five days after admission, propranolol 10 mg twice daily was introduced when the patient’s blood pressure stabilised. Both medications were continued until the patient underwent radioiodine treatment. Her free thyroxine level improved significantly within five days, but her thyroid-stimulating hormone levels improved at a much slower rate (Table II). The patient’s condition improved without the use of thionamide and she was discharged after two weeks. She underwent radioiodine treatment ten days after discharge. Thyroxine replacement was started for post-radioiodine hypothyroidism.
Table II
Thyroid function test trend.
Studies have shown that in patients with Graves’ hyperthyroidism, cholestyramine used in combination with thionamide can lead to a more rapid decline in thyroid hormone levels than with standard therapy alone.(1,2) Cholestyramine was also effective in Graves’ hyperthyroidism and iodine contrast-induced hyperthyroidism that was refractory to conventional treatment.(3) However, data on cholestyramine as a monotherapy for hyperthyroidism is limited. De Luis et al reported the successful use of cholestyramine alone in treating thyroxine overdose-induced hyperthyroidism.(4) Lin et al reported a case of interferon alpha- and possibly iodine contrast-induced hyperthyroidism, which was successfully treated with cholestyramine alone.(5) Our literature search did not find any data on cholestyramine monotherapy for Graves’ hyperthyroidism.
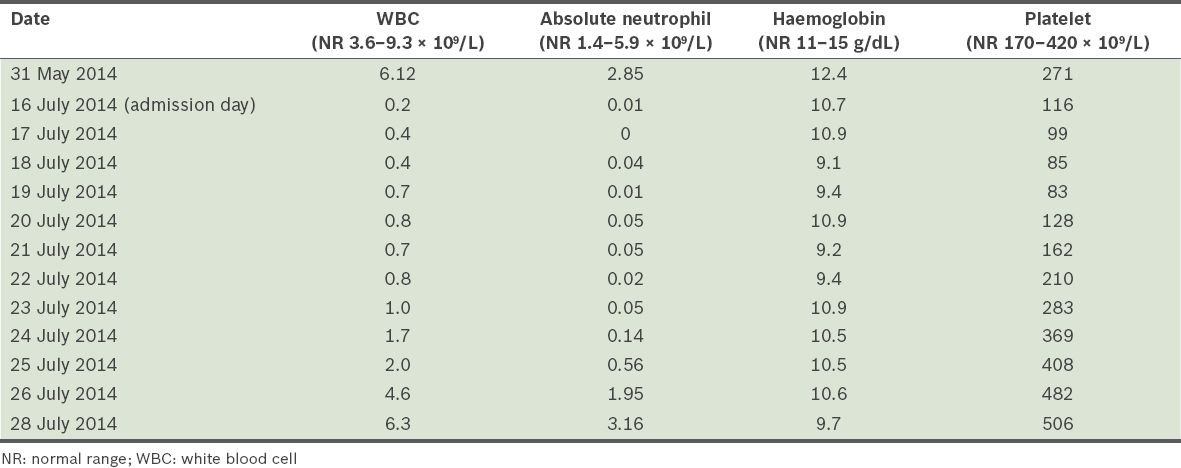
Cholestyramine enhances the enterohepatic excretion of thyroxine.(5) Lin et al stated that “complete normalisation of free thyroid hormones and notable symptom improvement have occurred within one week of instituting cholestyramine”.(5) The optimal dosage is 4 g 2–4 times daily for four weeks.(5) The patient was neutropenic for ten days (Table III) despite daily dosing of granulocyte colony-stimulating factor and cessation of carbimazole. Blood film showed no blast/dysplasia. Her neutrophil count prior to carbimazole initiation was normal. Agranulocytosis typically occurs within 1–2 months of thiamazole administration and resolves in 1–2 weeks after drug cessation.(6) Due to her presentation, drug-induced neutropenia was the most likely diagnosis. Improving cytopenia with sepsis treatment was possible but less likely.
Table III
Full blood count trend.
Thionamides were contraindicated in this patient. Glucocorticoids, which are part of the standard treatment for thyroid storm, were an option. However, they could complicate the ongoing sepsis and thus were not used. This case showed that cholestyramine is an effective monotherapy for Graves’ hyperthyroidism when thionamides are contraindicated. Our study raises the question of whether cholestyramine should be introduced routinely and from the start as part of treatment for Graves’ hyperthyroidism or even thyroid storm.
Yours sincerely,
References Kaykhaei MA, Shams M, Sadegholvad A, Dabbaghmanesh MH, Omrani GR. Low doses of cholestyramine in the treatment of hyperthyroidism.Endocrine. 2008;34:52-5. Tsai WC, Pei D, Wang TF, et al. The effect of combination therapy with propylthiouracil and cholestyramine in the treatment of Graves’ hyperthyroidism.Clin Endocrinol (Oxf). 2005;62:521-4. Alswat KA. Role of Cholestyramine in Refractory Hyperthyroidism: A Case Report and Literature Review.Am J Case Rep. 2015;16:486-90. de Luis DA, Dueñas A, Martin J, et al. Light symptoms following a high-dose intentional L-thyroxine ingestion treated with cholestyramine.Horm Res. 2002;57:61-3. Lin D, Suwantarat N, Bornemann M. Cholestyramine for thyrotoxicosis?.J Fam Pract. 2013;62:E1-2. Mohan A, Joseph S, Sidharthan N, Murali D. Carbimazole-induced agranulocytosis.J Pharmacol Pharmacother. 2015;6:228-30.
1. Kaykhaei MA, Shams M, Sadegholvad A, Dabbaghmanesh MH, Omrani GR. Low doses of cholestyramine in the treatment of hyperthyroidism. Endocrine 2008; 34:52-5. https://doi.org/10.1007/s12020-008-9107-5
PMid:18946743
2. Tsai WC, Pei D, Wang TF, et al. The effect of combination therapy with propylthiouracil and cholestyramine in the treatment of Graves' hyperthyroidism. Clin Endocrinol (Oxf) 2005; 62:521-4. https://doi.org/10.1111/j.1365-2265.2005.02249.x
PMid:15853819
3. Alswat KA. Role of Cholestyramine in Refractory Hyperthyroidism: A Case Report and Literature Review. Am J Case Rep 2015; 16:486-90. https://doi.org/10.12659/AJCR.893821
PMid:26207323 PMCid:PMC4517850
4. de Luis DA, Due-as A, Martin J, et al. Light symptoms following a high-dose intentional L-thyroxine ingestion treated with cholestyramine. Horm Res 2002; 57:61-3. https://doi.org/10.1159/000057950
5. Lin D, Suwantarat N, Bornemann M. Cholestyramine for thyrotoxicosis? J Fam Pract 2013; 62:E1-2.
PMid:23570035
6. Mohan A, Joseph S, Sidharthan N, MuralI D. Carbimazole-induced agranulocytosis. J Pharmacol Pharmacother 2015; 6:228-30. https://doi.org/10.4103/0976-500X.171881
PMid:26813922 PMCid:PMC4714394