

Abstract
Hydrocoele of the canal of Nuck is a rare condition in adult women caused by a failure of complete obliteration of the canal of Nuck. It may be likened to a patent processus vaginalis in men. In most cases, the diagnosis is made during surgery as it is often mistaken for an inguinal hernia. We report a case where the diagnosis of this condition was made preoperatively on imaging. The salient anatomy, clinical features, radiological images and surgical management are discussed and the medical literature reviewed.
CASE PRESENTATION
A 31-year-old Chinese woman with no significant medical or surgical history initially presented to the general surgery service with right groin swelling of one month’s duration. The swelling became more prominent with exertion and prolonged standing, and was associated with mild discomfort. On palpation, there was a non-tender, soft cystic swelling at the right groin, but no classical expansile cough impulse was present. The swelling was not manually reducible upon lying down.
In view of the above clinical findings, ultrasonography of the right groin was ordered in the outpatient setting (Figs.
Fig. 1
Longitudinal US image of the right groin.
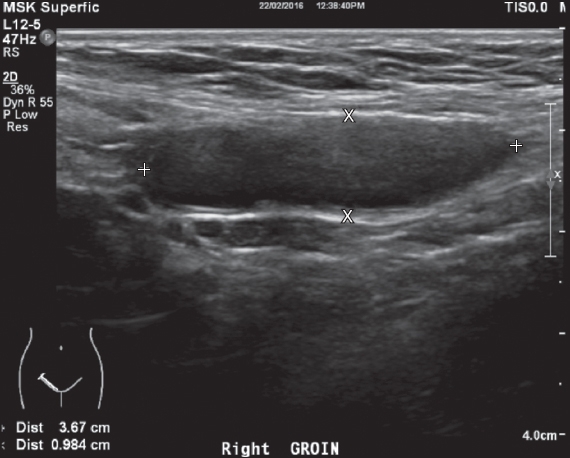
Fig. 2
Colour Doppler US image of the right groin. IEA: inferior epigastric artery; MED: medial
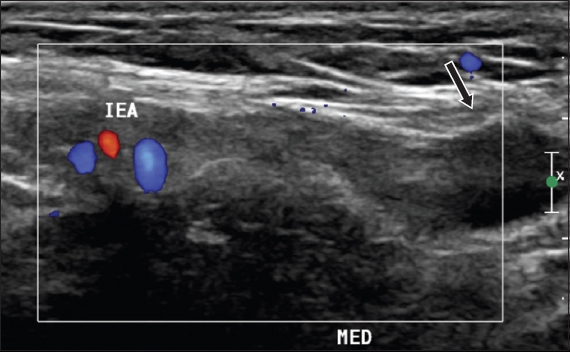
IMAGE INTERPRETATION
Ultrasonography of the right groin shows a well-circumscribed elongated cystic structure in the right inguinal region measuring 3.7 cm × 1.8 cm × 0.9 cm (
DIAGNOSIS
Right hydrocoele of the canal of Nuck.
CLINICAL COURSE
This patient eventually underwent an elective laparoscopic excision of the right hydrocoele of the canal of Nuck. Laparoscopy revealed a right patent processus vaginalis with the round ligament exiting the peritoneal cavity into the canal of Nuck lateral to the inferior epigastric vessels. There were no contents in the canal. The peritoneal sac and round ligament were excised, and the wide, deep inguinal ring defect was reinforced with a mesh in a manner similar to the transabdominal preperitoneal (TAPP) mesh repair technique. The mesh was anchored in place using absorbable tackers, and the peritoneal flap was anchored back in place with absorbable tackers to cover the mesh. The patient recovered well postoperatively.
DISCUSSION
Hydrocoele of the canal of Nuck is a rare condition in adult women caused by a failure of complete obliteration of the canal of Nuck. We herein report the case of a female patient with a hydrocoele of the canal of Nuck who was diagnosed using ultrasonography and treated with laparoscopic mesh repair. Cystic groin masses in women are rare, and the anatomic and embryologic characteristics of the groin area are complex. Hence, a good understanding of the local anatomic characteristics of the groin allows characterisation of pathologic conditions in the groin. We focus on the female anatomy in this article, as the male inguinal anatomy is well-described.
The inguinal region encompasses two adjacent but anatomically distinct areas: the inguinal canal and the femoral triangle. The inguinal canal is a 4-cm oblique passage that passes inferomedially from the internal to the external inguinal rings, and lies parallel to and immediately above the inguinal ligament. The inguinal canal contains the round ligament (i.e. spermatic cord in the male) and its fascial coverings. The round ligaments are bilateral structures arising from the uterine horns, where the uterus and fallopian tubes meet. They course laterally from the uterus through the broad ligament and extend laterally and anteriorly along the pelvic wall, hooking around the inferior epigastric artery before leaving the abdomen through the deep inguinal ring. The round ligament traverses the inguinal canal with the round ligament artery and ilioinguinal nerve, and terminates in the labia majora.(1-2) The round ligament consists mainly of muscular tissue derived from the uterus, fibrous and areolar tissue, and blood vessel and nerves. These are enclosed in a double fold of peritoneum which, in the fetus, is a tubular process extending for a short distance into the inguinal canal, called the canal of Nuck. It is generally obliterated in adults but sometimes remains patent even into adulthood, as in this patient’s case.
Hydrocoele of the canal of Nuck in the adult woman may be likened to a patent processus vaginalis in men. The processus vaginalis is an evagination of parietal peritoneum that occurs before the descent of the testes. In women, the same evagination accompanies the round ligament of the uterus as it descends into the labia majora through the inguinal canal. The canal of Nuck is usually obliterated at around the eighth month of fetal life. (3-4) Hydrocoeles of the canal of Nuck typically present as an irreducible, painless swelling in the inguinolabial region that is sometimes transilluminable. (5) They can also present as a painful lump and cause an erythematous swelling extending to the labia majora in rare cases of infection. (3) However, the diagnosis of a hydrocoele in women is seldom made on clinical examination alone. In one-third of patients, a concomitant inguinal hernia is found. (4-6) Therefore, imaging is crucial in making a diagnosis for groin lumps.
The use of ultrasonography supported by colour Doppler imaging has increased in recent years due to its advantage as a noninvasive and dynamic assessment of soft tissues, which is difficult to achieve with other imaging modalities. In this patient, ultrasonography showed a well-circumscribed, elongated cystic structure in the right inguinal region with no internal vascularity noted on colour Doppler examination. It is prudent for clinicians to consider other diagnoses of cystic lesions in the inguinal region on ultrasonography.
Although not harmful, a canal of Nuck cyst can cause discomfort and pain. The symptoms are usually more pronounced on prolonged standing. As in our patient’s case, clinical history showed that the groin swelling slowly disappeared at night when the patient was lying down and reappeared gradually during the day when the patient was ambulating, ruling out the diagnosis of a mesothelial cyst. This characteristic was more suggestive of a groin hernia. Furthermore, this swelling did not have the classical expansile cough impulse associated with inguinal hernias and also could not be manually reduced. Cystic consistency coupled with the above symptoms and signs should remind clinicians to include this condition in their differential diagnosis when encountering groin lumps in women. In our case, it led to ultrasonography of the groin to further ascertain the nature and contents of the groin swelling. Ho et al have mentioned some rare instances of abnormal pathology involving the canal of Nuck, including endometriosis, infection and neoplasm. However, most cases are benign.(7)
There are a few conditions that can be confused with hydrocoele of the canal of Nuck on sonography. Oh et al described a cystic groin mass in a woman as rare and highlighted seven masses they encountered in their patients. Interestingly, a cyst of the canal of Nuck was not mentioned, likely due to its comparative rarity.(2) Sonographic features of groin masses were also discussed by Shadbolt et al.(8) Their paper also described radiological features of various groin masses on computed tomography and magnetic resonance imaging, which is not covered in the scope of this paper.
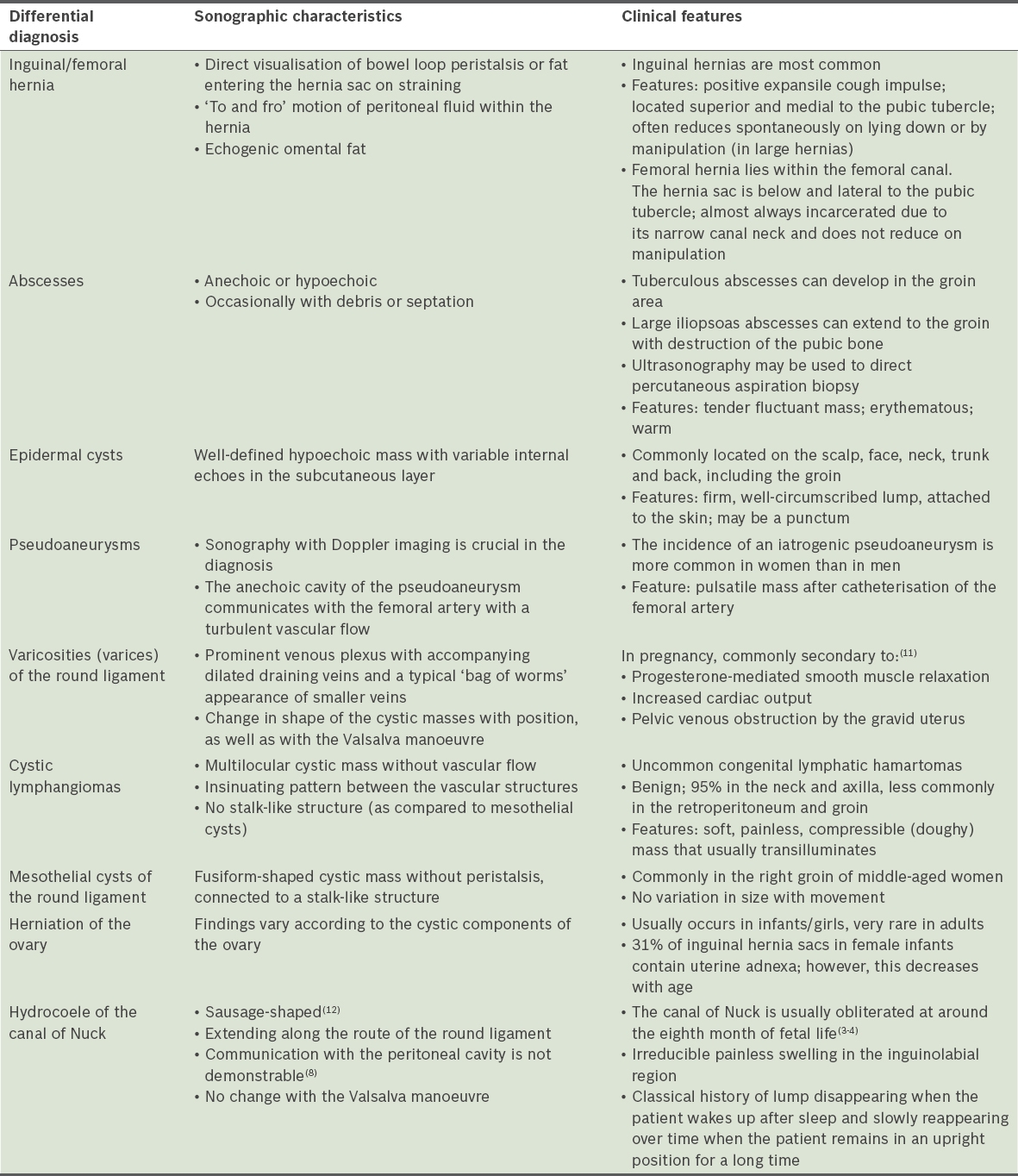
Table I
Sonographic and clinical features of cystic groin masses in women.
Traditionally, canal of Nuck cysts have been repaired through an open approach.(7) Very few published reports describe entirely laparoscopic management of canal of Nuck cysts. (10) As our patient was symptomatic, we offered diagnostic laparoscopy to confirm the radiological suspicion and to excise the canal of Nuck hydrocoele, followed by reinforcement of the inguinal canal with a mesh. Surgical treatment of canal of Nuck hydrocoeles, whether open or laparoscopic, involves excising the peritoneal hydrocoele sac entering the inguinal canal. Post-excision, the widened deep inguinal ring remains a potential site for future inguinal hernia formation. Hence, most surgeons repair and reinforce the inguinal canal. In open surgery, this can be performed using herniorrhaphy or hernioplasty technique. In laparoscopic repair, mesh reinforcement is the usual mode of covering the inguinal canal. Between the totally extraperitoneal (TEP) and TAPP repair laparoscopic approaches, we feel that the TAPP approach is a much better technique, as it allows proper visualisation of the anatomy and confirmation of the clinical diagnosis, for which entry to the peritoneal cavity is essential. Moreover, excising the hydrocoele sac invariably requires division of the peritoneum. In the TEP technique, this would invariably result in loss of the operative field due to escape of air into the peritoneal cavity, making further visualisation and mesh placement challenging.
In conclusion, there are various cystic masses, including those arising from the round ligament in the female groin, that can be differentiated by ultrasonography supported by colour Doppler imaging. Understanding the anatomy and embryology of the inguinal region improves the efficiency of the localisation and characterisation of masses in this area with imaging modalities.
SMJ-59-16.pdf