

Abstract
A 26-year-old male patient was referred for exercise-induced claudication that had interfered with his military duties for the past two years. He was an occasional smoker with no other significant cardiovascular risk factors. Initial Doppler ultrasonography showed narrowing of the popliteal artery. Further evaluation with magnetic resonance angiography demonstrated a short segment occlusion of the popliteal artery secondary to an anomalous origin of the medial head of the gastrocnemius muscle from the lateral femoral condyle. Based on the clinical presentation and imaging findings, he was diagnosed with popliteal artery entrapment syndrome. In this article, we discussed the typical presenting signs and symptoms of popliteal artery entrapment syndrome, the different imaging modalities available to aid diagnosis, classification of the condition and the available treatment options.
CASE PRESENTATION
A 26-year-old male patient was referred for suspected exercise-induced claudication, which had interfered with his military duties over the past two years. He complained of right calf pain after walking approximately 200 m, which was relieved by rest. He was an occasional smoker with no other significant cardiovascular risk factors or past medical history. Physical examination was unremarkable.
The patient underwent Doppler ultrasonography and magnetic resonance (MR) angiography of the right lower limb (
Fig. 1
(a & b) Doppler US images of the right popliteal artery and (c) reconstructed three-dimensional MR angiogram of the right popliteal artery.
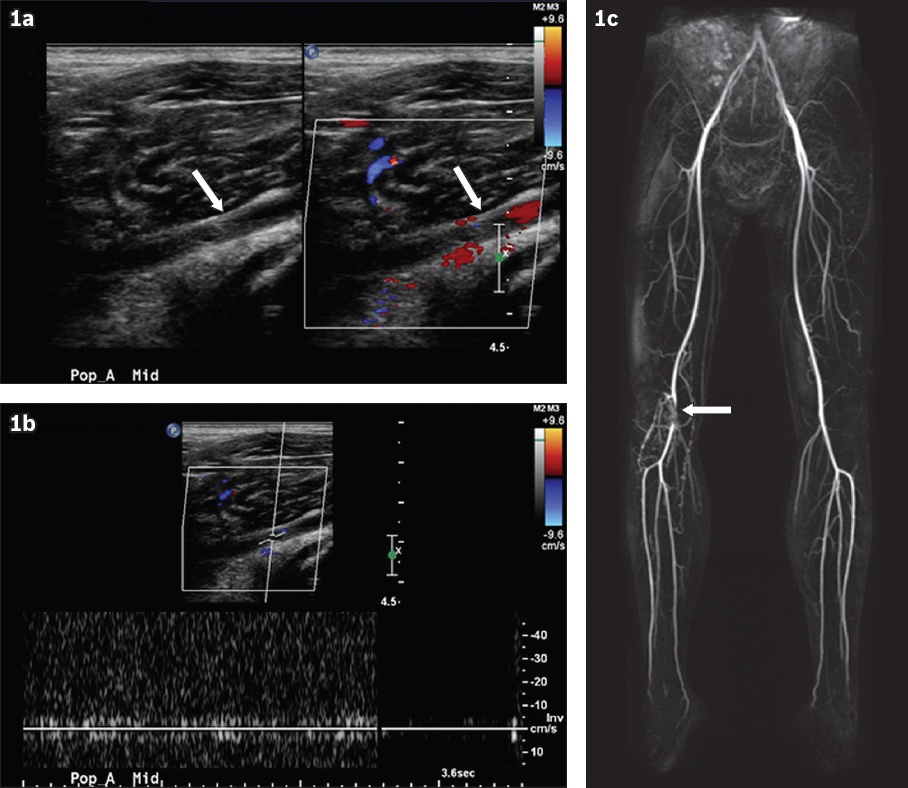
Fig. 2
Serial (a–d) axial and (e & f) coronal T2-W MR images from superior to inferior show the course of the gastrocnemius tendon.
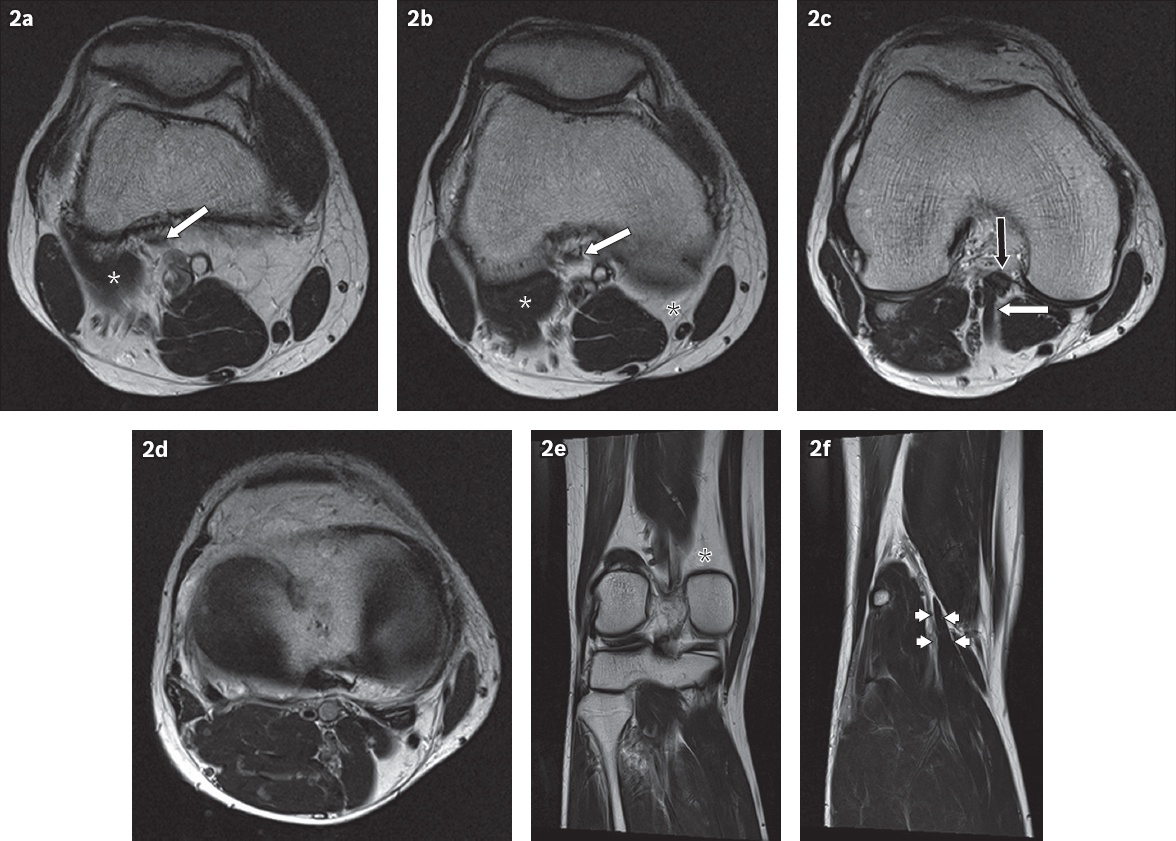
IMAGE INTERPRETATION
Doppler ultrasonography demonstrates loss of normal arterial flow and waveform in the popliteal artery (arrow, Figs.
Serial axial T2-weighted (T2-W) MR images from the superior (
DIAGNOSIS
Popliteal artery entrapment syndrome (PAES) Type II.
CLINICAL COURSE
The patient’s case was discussed at a vascular surgery and radiology multidisciplinary team meeting. In view of the patient’s young age and significant clinical symptoms, surgical decompression was offered.
DISCUSSION
PAES represents an anomalous relationship between the popliteal musculotendinous structures and the artery. It is a rare but well-described cause of intermittent claudication, typically in young patients with no cardiovascular risk factors or atherosclerosis.(1) It represents a developmental abnormality with several known variations in the popliteal fossa that leads to entrapment of the artery. PAES is a progressive condition that, if left untreated, can lead to premature arteriosclerosis and stenosis secondary to repeated chronic compression and microvascular trauma.(2) In addition, turbulent flow through a tight stenosis can lead to poststenotic aneurysm formation. Hence, early diagnosis or exclusion of PAES is of paramount importance in a young adult presenting with intermittent claudication.(3)
PAES has a reported clinical prevalence of approximately 0.17% in young males entering military service, although the true incidence may be much higher, with anatomical PAES having a reported prevalence of 3.5% in autopsy cases.(4,5) PAES can also occur bilaterally in approximately 27%–67% of affected patients.(6) Several classification systems exist, one of which is a widely used classification system proposed by Love and Whelan in 1965 that classified PAES into six main subtypes (
Box 1
Classification of popliteal artery entrapment syndrome.
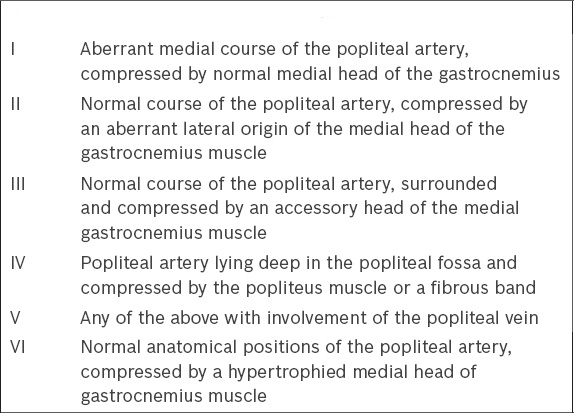
PAES Types I–V involve an abnormal relationship between the vessels, musculotendinous structures or fibrous bands.(7)
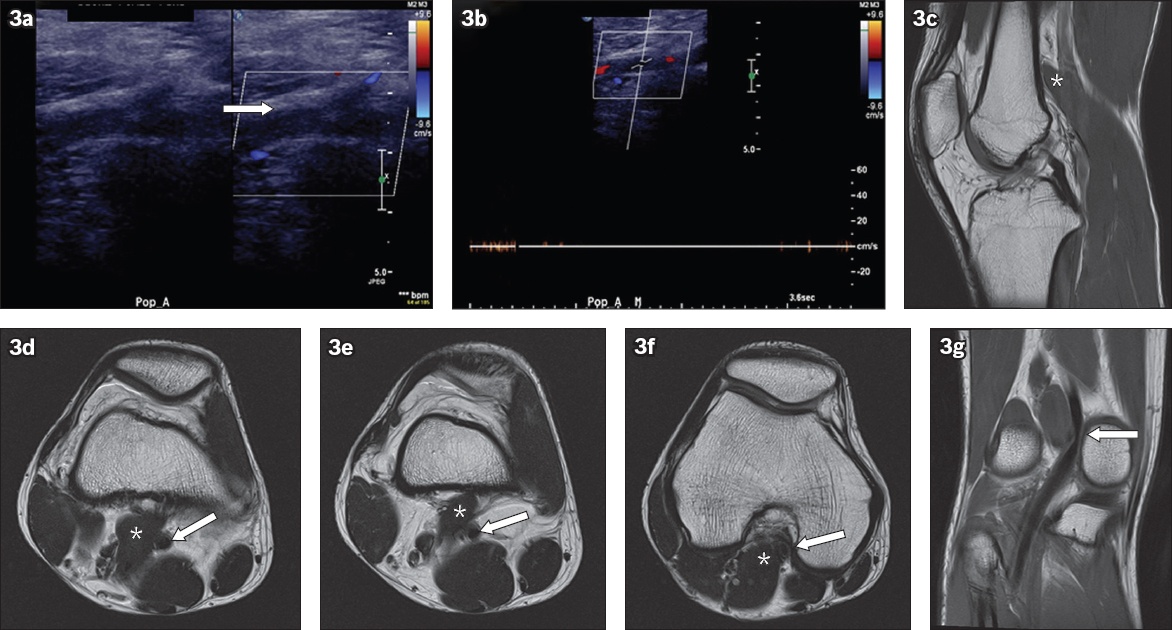
Fig. 3
A 23-year-old female patient presented with exercise-induced claudication of the right lower limb. (a & b) Doppler US images of the right knee show loss of normal arterial flow and waveform in the right popliteal artery. (c) Sagittal T2-W MR image shows the normal origin of the medial head of the gastrocneumius muscle (white asterisk in 3c). (d–f) Axial T2-W MR images show an aberrant medial course of the popliteal artery (white arrows in Figs.
For patients with suspected PAES, there is no widely accepted consensus for the ideal diagnostic workup. In our centre, we used Doppler ultrasonography for the initial evaluation of the popliteal artery, followed by MR angiography/imaging for a more detailed evaluation. MR imaging has several advantages. (a) There is no radiation exposure for the patient compared with computed tomography (CT) and conventional digital subtraction angiography (DSA). (b) MR imaging has superior soft tissue contrast to clearly delineate any aberrant popliteal fossa anatomy. This will help guide any surgical intervention. (c) Complications such as poststenotic aneurysm formation can be readily identified. (d) It can differentiate PAES from other differential diagnoses, including vasculitis or cystic adventitial disease, which are also rare vascular (predominantly arterial) pathologies that occur in young adults with no cardiovascular risk factors.
Our MR angiography/imaging protocol utilises gadolinium-enhanced MR angiography of both lower limbs from the common femoral arteries to the distal leg. This is performed at rest in a neutral position. Non-contrast time-of-flight images are another option but, in our experience, are not as robust as contrast-enhanced images and more prone to motion artefacts. Anatomical T2-W axial and coronal images are then acquired to demonstrate the origins and alignment of the medial and lateral heads of the gastrocnemius and popliteus muscles and their associations with the popliteal artery, vein and nerves. These images are acquired at rest. If vascular compression is not observed, additional T2-W two-dimensional steady state images are acquired across the popliteal fossa using provocative manoeuvres. Patients are instructed to perform continuous plantar flexion and dorsiflexion of the feet to recreate their claudication symptoms, after which they maintain plantar flexion while the scan is performed. This may help to accentuate any vascular compression. The main problem with this imaging method is the difficulty in maintaining the forced plantar flexion due to patient discomfort and exhaustion, which may result in motion artefacts that degrade the image quality.
Aberrant anatomy in the popliteal fossa may be incidentally diagnosed on MR imaging in asymptomatic patients (
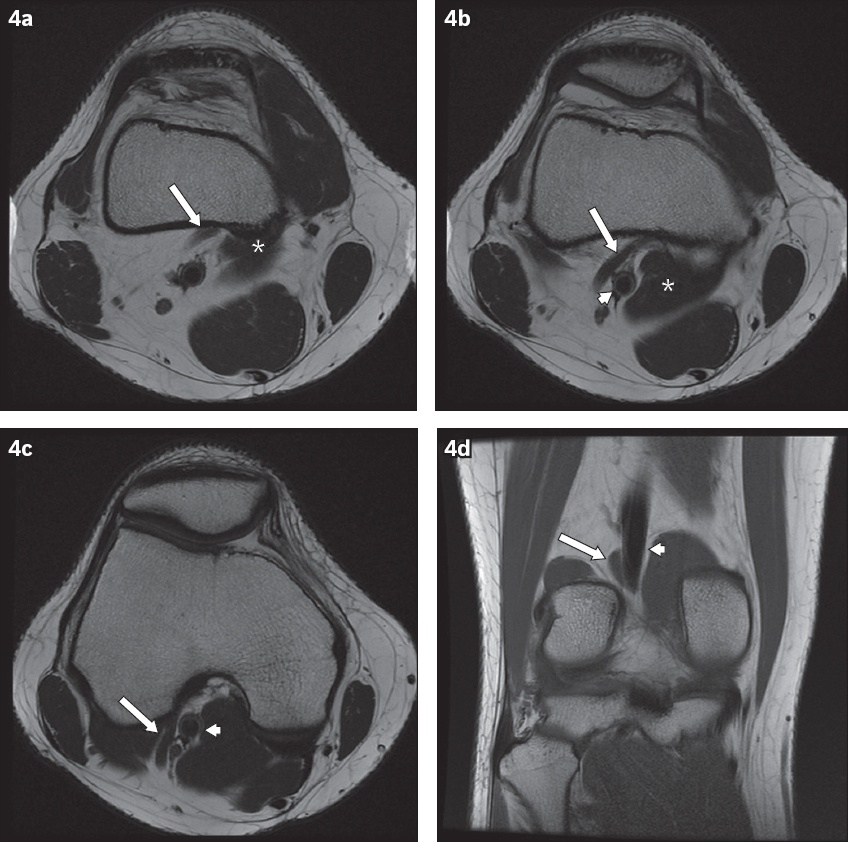
Fig. 4
Incidental finding of aberrant popliteal fossa anatomy with no entrapment of the popliteal artery. (a–c) Axial T2-W and (d) coronal T1-W MR images show an accessory head of the medial gastrocnemius muscle (arrow in Figs.
Potential differential diagnoses of PAES in young patients without vascular risk factors include cystic adventitial disease and other forms of vasculitis.
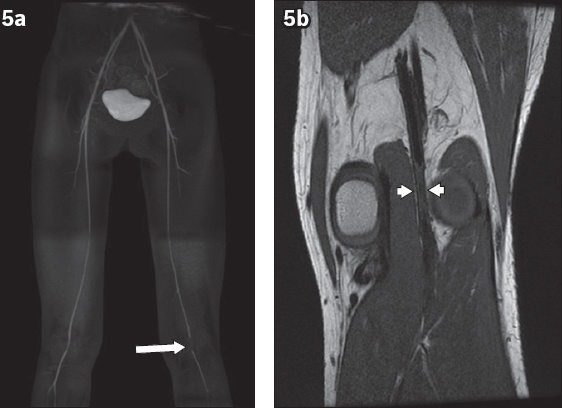
Fig. 5
A 26-year-old man presented with chronic left lower limb claudication. (a) Reconstructed MR angiogram of both lower limbs shows abrupt truncation of flow-related signal in the left popliteal artery (arrow). (b) Coronal T1-W image shows severe stenosis and mural thickening of a segment of the popliteal artery (arrowheads) with no evidence of popliteal artery entrapment.
Treatment for PAES involves a multidisciplinary surgical approach and depends on the degree of vascular compromise and the type of compression. The primary aim is to relieve the compression of the artery using musculotendinous section, restoring normal arterial flow to the limb.(9) Chronic occlusion and arteriosclerosis of the vessels may require additional vascular bypass or grafting, which commonly utilise the saphenous vein.(10) Endovascular repair alone is not recommended due to a high risk of re-occlusion, as the underlying cause of popliteal entrapment has not been addressed.
In conclusion, PAES is a rare cause of intermittent claudication or acute limb ischaemia that is especially relevant in young adults with no cardiovascular risk factors. Early diagnosis and treatment are important to prevent complications of this progressive condition. Radiologists play an essential role in the diagnosis of PAES. MR angiography/imaging can provide noninvasive detection of vascular stenosis, as well as an accurate assessment of aberrant popliteal fossa anatomy.
SMJ-59-344.pdf