Singapore Med J 2018; 59(10): 550-554 doi: https://doi.org/10.11622/smedj.2018128
Clinics in diagnostic imaging (191)
Mark Christopher Pearce1, MD, Garry Choy2, MD, Robert Chun Chen3, MD
Author Information >Copyright and License information >
1Department of Medical Imaging, Saskatoon Health Region, Saskatoon, Saskatchewan, Canada 2Department of Radiology, Massachusetts General Hospital, Boston, Massachusetts, USA 3Department of Diagnostic Radiology, Singapore General Hospital, Singapore Correspondence: Dr Robert Chen, Consultant Radiologist, Department of Diagnostic Radiology, Singapore General Hospital, Outram Road, Singapore 169608. robert.chen@sgh.com.sg
A 49-year-old Chinese man was evaluated for progressive uncoordinated movements, dysphagia and urinary symptoms. Magnetic resonance imaging demonstrated a cruciform pattern of T2-weighted hyperintensity within the pons and selective atrophy of the cerebellar hemispheres and pons. The clinical history and radiological findings were consistent with a diagnosis of multiple system atrophy-cerebellar type. This article discussed the background, proposed mechanisms, diagnosis, radiological characteristics, prognosis and management of multiple system atrophy-cerebellar type.
Keywords: multiple system atrophy cerebellar type, sporadic olivopontocerebellar atrophy, type C
CASE PRESENTATION
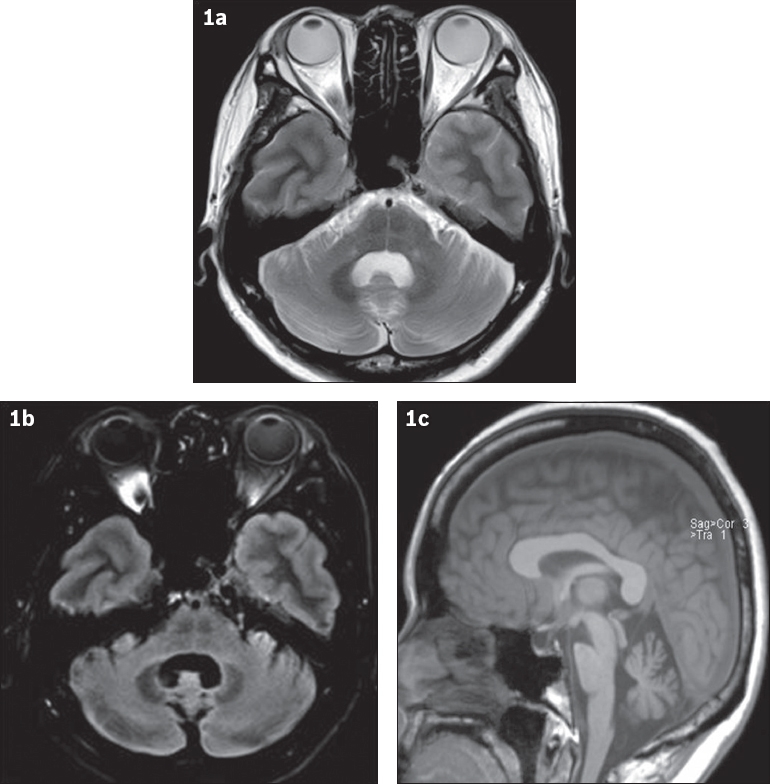
A 49-year-old Chinese man with no significant past medical history was evaluated for a two-year history of progressive uncoordinated movements, dysphagia and urinary symptoms. According to his wife, he had given up badminton over a year ago and was increasingly unsteady on his feet. Faced with an extended leave of absence from work, he sought the attention of a neurologist. Clinical examination confirmed marked gait and limb ataxia as well as significant orthostatic hypotension and slightly garbled speech. What do the magnetic resonance (MR) images (Fig. 1) show?
Axial T2-weighted (Fig. 1a) and T2-weighted fluid-attenuated inversion recovery (Fig. 1b) MR images at the level of the cerebellum demonstrate a cruciform pattern of hyperintensity within the pons, representing a hot cross bun sign. Enlargement of the fourth ventricle, with atrophy of the cerebellum and ventral flattening of the pons, is best demonstrated on the sagittal T1-weighted sequence (Fig. 1c).
DIAGNOSIS
Multiple system atrophy-cerebellar type (MSA-C).
CLINICAL COURSE
Once diagnosed, the patient was subsequently referred to occupational and physical therapy for outpatient neurorehabilitation. His clinical symptoms of neurogenic bladder, recurrent urinary tract infections and orthostatic hypotension were managed by the neurology department to provide symptomatic relief. The patient continued to deteriorate over the next seven years, eventually becoming bedbound and fully dependent on home care for activities of daily living. He eventually passed away from aspiration pneumonia.
DISCUSSION
MSA-C, also referred to as sporadic olivopontocerebellar atrophy, is a rare and unfortunately fatal neurodegenerative disease. According to Fanciulli and Wenning, the combined prevalence of both MSA-C and MSA-P (multiple system atrophy with Parkinson’s subtype) is only around 4.4 cases in 100,000.(1) The peak incidence typically occurs in the sixth decade of life, with no known gender predilection. There are no proven environmental risk factors for MSA-C, although exposure to pesticides, organic solvents and metal dust are classically thought to be associated with the disease.(1) The accumulation of alpha-synuclein glial cytoplasmic inclusions in the pons, cerebellum and inferior olives is thought to result in dysfunction of neurons and oligodendrocytes, which ultimately leads to cellular death.(2) The precise mechanism behind the increase in alpha-synuclein remains unknown, although mutations in several genetic loci, including the COQ2 and GBA genes, have been investigated.(3)
The disease typically manifests with prodromal autonomic symptoms, including urinary incontinence, sexual dysfunction and orthostatic hypotension; cerebellar symptoms typically occur later in the disease course. As the disease progresses, patients typically develop limb and gait ataxia, action tremor and abnormal posturing. Dysarthria, dysphagia and drooling generally characterise more advanced disease.(3) MSA-C may also be associated with sleep breathing disorders and rapid-eye movement sleep behavioural disorder. Ultimately, a definitive diagnosis of MSA requires histopathology and is often only obtained post-mortem. The diagnostic criteria for probable and possible MSA-C are shown in Table I. Supporting features may include additional clinical and radiological findings from the second consensus statement on the diagnosis of MSA by Gilman et al.(4) Nevertheless, even with consensus criteria, the clinical presentation of MSA-C (i.e. adult-onset ataxia with autonomic symptoms) can remain a diagnostic challenge, requiring consideration of toxic causes, vitamin deficiency, infectious states, immune-mediated pathology and other neurodegenerative disorders.(5) Clinical history to determine the chronicity of symptoms, family history, a full neurologic examination and autonomic function testing, including tilt-table testing, are essential. Laboratory investigations should be guided by history and physical findings, but may include testing for Vitamin B1, E or B12, alcohol levels, complete blood count, renal function, liver function tests, human immunodeficiency virus, venereal disease research laboratory or select autoantibodies depending on the clinical picture.
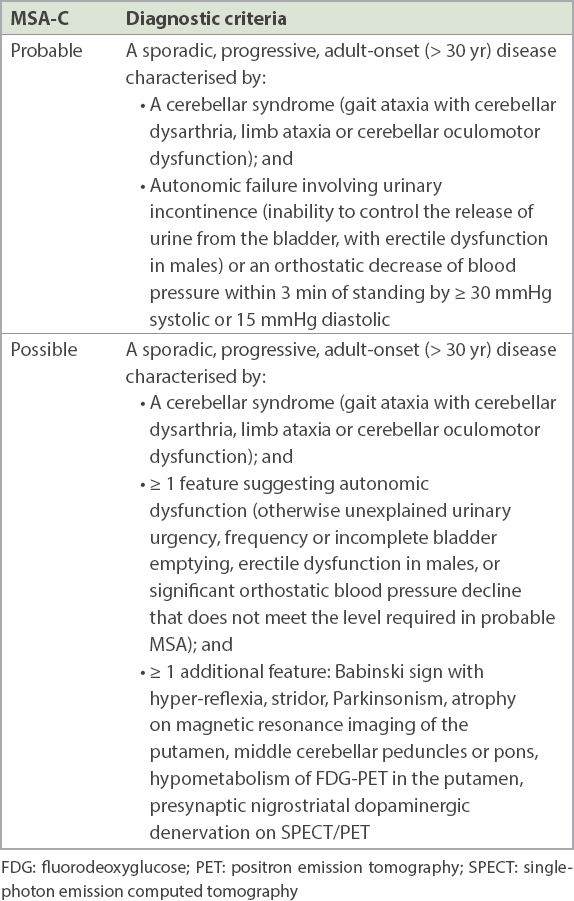
Table I
Diagnostic criteria for probable and possible multiple system atrophy-cerebellar type (MSA-C).(4)
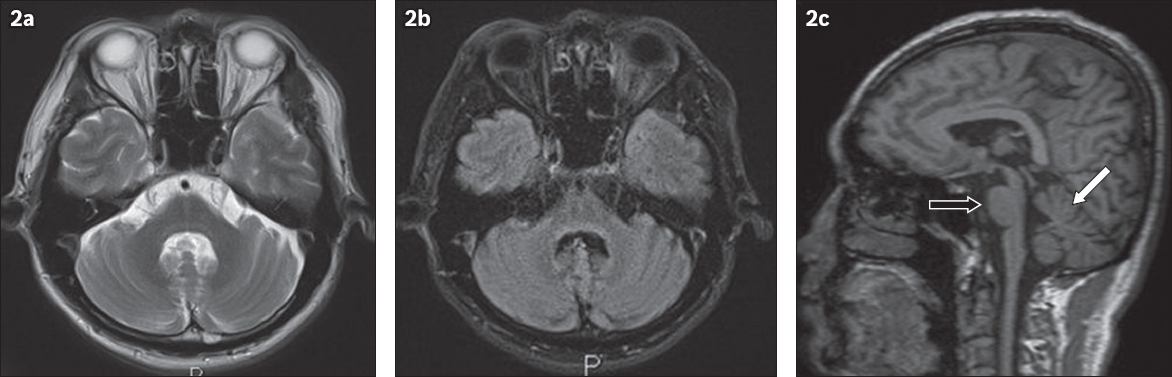
Magnetic resonance (MR) imaging and, infrequently, positron emission tomography (PET) are the primary neuroimaging modalities when MSA-C is suspected. As expected for a disease affecting gait and limb ataxia, multi-sequence MR imaging typically reveals atrophy of the cerebellum, but may also involve selective atrophy of the ventral pons, putamen, middle cerebellar peduncles (MCPs) and inferior olives.(6) Most characteristic for this entity is a cruciform pattern of T2 hyperintensity within the pons (hot cross bun sign), which is seen in up to 96% of probable MSA-C cases (Fig. 2);(7) this radiologic pattern is the result of selective degeneration of the myelinated transverse pontocerebellar fibres and pontine neurons, with conservation of the craniocaudally oriented corticospinal tracts.(1,7) Increased signal on the apparent diffusion coefficient map within the MCPs, cerebellum, pons and putamen may also aid in the diagnosis of MSA-C.(8) Furthermore, PET imaging may also reveal fluorodeoxyglucose hypometabolism within the cerebellum and MCPs.(9)
Fig. 2
Multi-sequence multi-planar MR images from a 59-year-old man with chronic alcohol abuse. (a) Axial T2-W; (b) axial T1-W; and (c) sagittal T1-W images show atrophy of the cerebellum (white arrow) with relative sparing of the pons (black arrow). In contrast, the pons in an MSA-C patient is typically flattened. No hot cross bun sign is seen on the axial T2-W images in the pons.
The radiologic differential diagnosis of cerebellar atrophy is broad but typically includes more commonly encountered processes such as chronic alcohol ingestion and Dilantin-induced cerebellar atrophy (Fig. 3). These entities will not demonstrate a hot cross bun sign, preferentially result in cerebellar atrophy and typically do not result in pontine flattening.(10) Clinical history is often more helpful in making the diagnosis than imaging. When presented with MR findings suspicious for MSA-C (cruciform T2 hyperintensity of the pons and selective atrophy of the posterior fossa contents), the differential diagnosis is limited to a select few rare entities for which only a handful of cases have been reported in the literature. Spinocerebellar ataxia, in particular Subtypes 2, 3 and 6, can be radiologically indistinguishable from MSA-C.(11) In these instances, genetic testing can help differentiate this inherited neurodegenerative disease from MSA. Additionally, there have been rare case reports of hot cross bun signs occurring in variant Creutzfeldt-Jakob disease (vCJD) and vasculitis, although this is certainly not their typical radiologic presentation. vCJD classically presents with signal abnormality in the posterior thalamus, which is known as the hockey stick sign,(12) while vasculitis may present with supratentorial and infratentorial areas of ischaemia, infarction and vessel wall irregularity.(13) It is important to note that while neuroimaging findings may be highly suggestive of MSA-C, they are ultimately not essential, as the current diagnostic criteria of MSA-C are solely based on clinical findings. As such, neuroimaging may be used in instances of clinical diagnostic uncertainty.
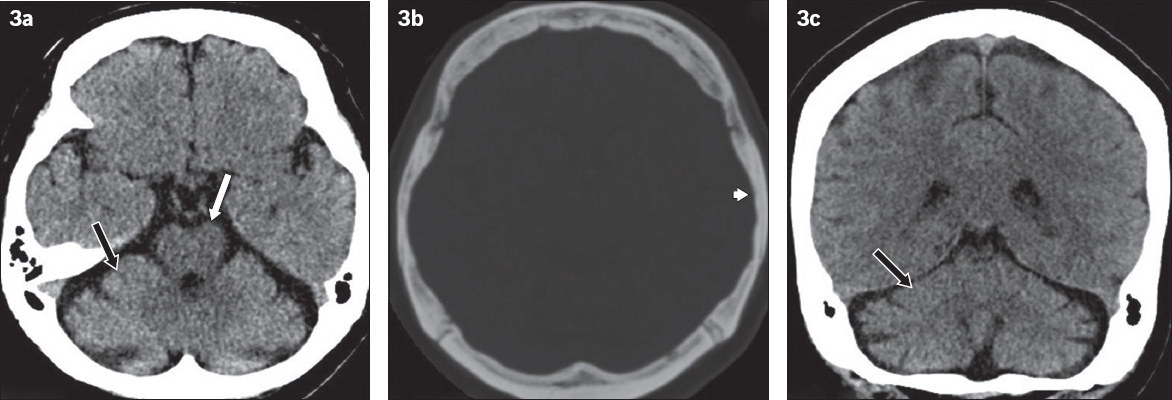
Fig. 3
Multi-planar (a) axial; (b) axial bone window; and (c) coronal CT images in a patient with epilepsy and chronic Dilantin use. There is preferential atrophy of the cerebellum (black arrow in a & c) with relative sparing of the pons (white arrow) and supratentorial brain. Diffuse bone marrow expansion is also seen (white arrowhead), secondary to chronic Dilantin use.
Unfortunately, the prognosis for MSA-C is dismal and includes a slow and progressive period of decline over 5–10 years before death.(14) Interventions are directed at alleviating symptoms and improving quality of life, as there is no effective disease-modifying treatment for its progressive cerebellar ataxia. Medications such as fludrocortisone, oxybutynin and selective serotonin reuptake inhibitors may be used to address commonly encountered symptoms such as orthostatic hypotension, overactive bladder and concomitant depression, respectively.(15)
References Fanciulli A, Wenning GK. Multiple-system atrophy.N Engl J Med. 2015;372:1375-6. Ozawa T, Paviour D, Quinn NP, et al. The spectrum of pathological involvement of the striatonigral and olivopontocerebellar systems in multiple system atrophy: clinicopathological correlations.Brain. 2004;127:2657-71. Laurens B, Vergnet S, Lopez MC, et al. Multiple system atrophy: state of the art.Curr Neurol Neurosci Rep. 2017;17:41. Gilman S, Wenning GK, Low PA, et al. Second consensus statement on the diagnosis of multiple system atrophy.Neurology. 2008;71:670-6. Barsottini OG, Albuquerque MV, Braga-Neto P, Pedroso JL. Adult onset sporadic ataxias: a diagnostic challenge.Arq Neuropsiquiatr. 2014;72:232-40. Matsusue E, Fujii S, Kanasaki Y, et al. Cerebellar lesions in multiple system atrophy: postmortem MR imaging-pathologic correlations.AJNR Am J Neuroradiol. 2009;30:1725-30. Deguchi K, Ikeda K, Kume K, et al. Significance of the hot-cross bun sign on T2*-weighted MRI for the diagnosis of multiple system atrophy.J Neurol. 2015;262:1433-9. Kanazawa M, Shimohata T, Terajima K, et al. Quantitative evaluation of brainstem involvement in multiple system atrophy by diffusion-weighted MR imaging.J Neurol. 2004;251:1121-4. Lee PH, An YS, Yong SW, Yoon SN. Cortical metabolic changes in the cerebellar variant of multiple system atrophy: a voxel-based FDG-PET study in 41 patients.Neuroimage. 2008;40:796-801. Arora R. Imaging spectrum of cerebellar pathologies: a pictorial essay.Pol J Radiol. 2015;80:142-50. Okamoto K, Tokiguchi S, Furusawa T, et al. MR features of diseases involving bilateral middle cerebellar peduncles.AJNR Am J Neuroradiol. 2003;24:1946-54. Collie DA, Summers DM, Sellar RJ, et al. Diagnosing variant Creutzfeldt-Jakob disease with the pulvinar sign: MR imaging findings in 86 neuropathologically confirmed cases.AJNR Am J Neuroradiol. 2003;24:1560-9. Abdel Razek AA, Alvarez H, Bagg S, Refaat S, Castillo M. Imaging spectrum of CNS vasculitis.Radiographics. 2014;34:873-94. Low PA, Reich SG, Jankovic J, et al. Natural history of multiple system atrophy in the USA: a prospective cohort study.Lancet Neurol. 2015;14:710-9. Maaß S, Levin J, Höglinger G. Current treatment of multiple system atrophy.Curr Treat Options Neurol. 2016;18:51.
2. Ozawa T, Paviour D, Quinn NP, et al. The spectrum of pathological involvement of the striatonigral and olivopontocerebellar systems in multiple system atrophy: clinicopathological correlations. Brain 2004; 127:2657-71. https://doi.org/10.1093/brain/awh303
PMid:15509623
3. Laurens B, Vergnet S, Lopez MC, et al. Multiple system atrophy: state of the art. Curr Neurol Neurosci Rep 2017; 17:41. https://doi.org/10.1007/s11910-017-0751-0
PMid:28378233
4. Gilman S, Wenning GK, Low PA, et al. Second consensus statement on the diagnosis of multiple system atrophy. Neurology 2008; 71:670-6. https://doi.org/10.1212/01.wnl.0000324625.00404.15
PMid:18725592 PMCid:PMC2676993
6. Matsusue E, Fujii S, Kanasaki Y, et al. Cerebellar lesions in multiple system atrophy: postmortem MR imaging-pathologic correlations. AJNR Am J Neuroradiol 2009; 30:1725-30. https://doi.org/10.3174/ajnr.A1662
PMid:19541777
7. Deguchi K, Ikeda K, Kume K, et al. Significance of the hot-cross bun sign on T2*-weighted MRI for the diagnosis of multiple system atrophy. J Neurol 2015; 262:1433-9. https://doi.org/10.1007/s00415-015-7728-1
PMid:25845765
8. Kanazawa M, Shimohata T, Terajima K, et al. Quantitative evaluation of brainstem involvement in multiple system atrophy by diffusion-weighted MR imaging. J Neurol 2004; 251:1121-4. https://doi.org/10.1007/s00415-004-0494-0
PMid:15372256
9. Lee PH, An YS, Yong SW, Yoon SN. Cortical metabolic changes in the cerebellar variant of multiple system atrophy: a voxel-based FDG-PET study in 41 patients. Neuroimage 2008; 40:796-801. https://doi.org/10.1016/j.neuroimage.2007.11.055
PMid:18203624
10. Arora R. Imaging spectrum of cerebellar pathologies: a pictorial essay. Pol J Radiol 2015; 80:142-50. https://doi.org/10.12659/PJR.892878
PMid:25806100 PMCid:PMC4364256
11. Okamoto K, Tokiguchi S, Furusawa T, et al. MR features of diseases involving bilateral middle cerebellar peduncles. AJNR Am J Neuroradiol 2003; 24:1946-54.
PMid:14625215
12. Collie DA, Summers DM, Sellar RJ, et al. Diagnosing variant Creutzfeldt-Jakob disease with the pulvinar sign: MR imaging findings in 86 neuropathologically confirmed cases. AJNR Am J Neuroradiol 2003; 24:1560-9.
PMid:13679271
14. Low PA, Reich SG, Jankovic J, et al. Natural history of multiple system atrophy in the USA: a prospective cohort study. Lancet Neurol 2015; 14:710-9. https://doi.org/10.1016/S1474-4422(15)00058-7
15. Maaß S, Levin J, Höglinger G. Current treatment of multiple system atrophy. Curr Treat Options Neurol 2016; 18:51. https://doi.org/10.1007/s11940-016-0435-0
PMid:27787721