

Abstract
INTRODUCTION
The LMA Supreme™, i-gel® and LMA ProSeal™ are second-generation supraglottic airway devices. We tested the hypothesis that these devices differ in performance when used for spontaneous ventilation during anaesthesia.
METHODS
150 patients who underwent general anaesthesia for elective surgery were randomly allocated into three groups. Data was collected on oropharyngeal leak pressures, ease and duration of device insertion, ease of gastric tube insertion, and airway safety.
RESULTS
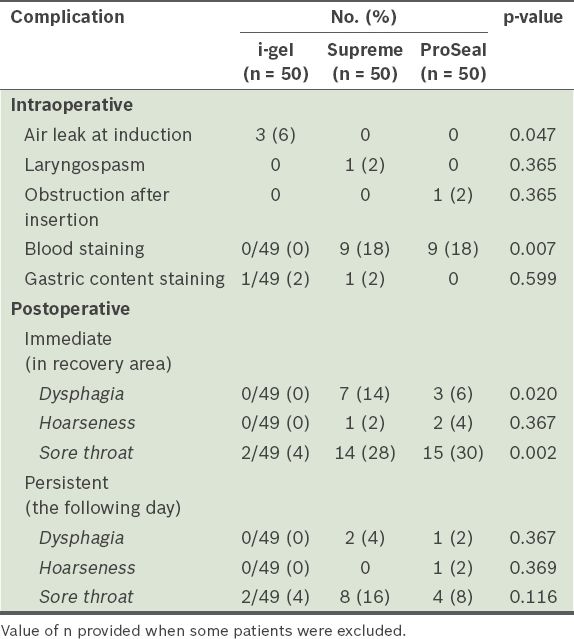
Leak pressure, our primary outcome measure, was found to be higher for the i-gel than the Supreme and ProSeal (mean ± standard error of the mean: 27.31 ± 0.92 cmH2O, 23.60 ± 0.70 cmH2O and 24.44 ± 0.70 cmH2O, respectively; p = 0.003). Devices were inserted on the first attempt for 90%, 82% and 72% of patients in the i-gel, Supreme and ProSeal groups, respectively (p = 0.105); mean device placement times were 23.58 seconds, 25.10 seconds and 26.34 seconds, respectively (p = 0.477). Gastric tubes were inserted on the first attempt in 100% of patients in the Supreme group, and 94% of patients in the i-gel and ProSeal groups (p = 0.100). There was blood staining on removal in 9 (18%) patients in each of the Supreme and ProSeal groups, with none in the i-gel group (p = 0.007). The incidence of postoperative sore throat, dysphagia and hoarseness was lowest for the i-gel.
CONCLUSION
The three devices were comparable in terms of ease and duration of placement, but the i-gel had higher initial oropharyngeal leak pressure and lower airway morbidity compared with the ProSeal and Supreme.
INTRODUCTION
The classic laryngeal mask airway (LMA), introduced by Brain in 1988, revolutionised the practice of airway management and is now routinely utilised in clinical anaesthesia.(1) Nevertheless, there are still limitations associated with the classic LMA, such as controlled ventilation being relatively contraindicated (due to its moderate oropharyngeal seal) and its unsuitability for patients at risk of aspiration.(2) Second-generation supraglottic airway devices (SADs) were designed to address these issues. The newer SADs have additional safety features that enhance the oesophageal and pharyngeal seals; the risk of aspiration is also minimised with the introduction of the gastric channel, which enables gastric suctioning, venting and passage of a nasogastric tube.
Second-generation SADs that are commonly used are the LMA ProSeal™ (Teleflex Medical Europe Ltd, County Westmeath, Ireland), LMA Supreme™ (LMA-S™; The Laryngeal Mask Company Pte Ltd, Singapore) and i-gel® (Intersurgical Ltd, Wokingham, UK). The ProSeal is a reusable device made of silicone with an inbuilt gastric port, an inflatable posterior pharyngeal cuff for better airway seal and a rigid bite block. The Supreme, introduced commercially in 2007, is a single-use SAD made of polyvinyl chloride with a gastric drain tube, large inflatable plastic cuff and preformed semi-rigid tube. The i-gel, also clinically introduced in 2007, is a single-use device comprising a soft gel-like cuffless mask, a narrow-bore gastric drain tube and an integral bite block. Numerous previous studies of these airway devices have demonstrated their easy, reliable insertion and low morbidity rate.(3-7)
However, comparative studies involving all three aforementioned airway devices are lacking. One study testing the three devices used the laryngoscope-guided and gastric tube-guided methods of insertion, while another was conducted on paralysed, ventilated patients undergoing laparoscopic surgery.(8,9) In contrast, our randomised clinical study employed the standard, manufacturer-recommended insertion techniques. We compared the clinical efficacy of all three devices in non-paralysed patients undergoing elective surgery, taking oropharyngeal leak pressure as the primary outcome measure. In addition, we tested secondary variables such as the ease and speed of SAD insertion, ease of gastric tube passage and perioperative airway complications.
METHODS
We recruited a total of 150 patients who were (a) aged 21–80 years; (b) of American Society of Anesthesiologists Grades I–III; and (c) due to undergo elective superficial or peripheral surgery in our tertiary hospital in the supine position, with an operation duration of more than 30 minutes. Exclusion criteria were body mass index > 35 kg/m2, history of known or predicted difficult airway, and known risk of aspiration. The study was approved by the SingHealth Centralised Institutional Review Board (reference: 2014/393/D) and written informed consent was obtained from all patients.
Patients were randomly allocated into three groups: Supreme, ProSeal and i-gel. Randomisation was performed using a random number table (
Standard monitoring (i.e. noninvasive blood pressure taking, pulse oximetry and electrocardiography) was applied before anaesthetic induction. After three minutes of preoxygenation, anaesthetic induction was initiated with intravenous fentanyl 1–2 µg/kg and intravenous propofol 2–3 mg/kg. The lungs were then manually ventilated via face mask and oral airway if required, using sevoflurane 2% in oxygen 100%, until there was a lack of response to jaw thrust and the jaw was adequately relaxed; additional intravenous boluses of propofol up to 0.5 mg/kg were administered if required. After post-induction apnoea occurred, the chosen SADs were lubricated and inserted according to the manufacturers’ recommendations. The Supreme and i-gel SADs were inserted using the rotational technique, whereas the ProSeal SAD was inserted using the index finger. The cuffs of the inflatable SADs, i.e. Supreme and ProSeal, were inflated with air to 60 cmH2O. Maintenance of anaesthesia was achieved using a mixture of oxygen and air with 1–1.5 minimum alveolar concentration sevoflurane. The patients were either spontaneously breathing or were temporarily placed on the ventilator with tidal volume set at 6 mL/kg and respiratory rate at 10–14 breaths/minute until spontaneous ventilation occurred.
All the SAD insertions were performed by the experienced co-investigators. The speed of SAD insertion was obtained by recording the time from which the SAD was picked up to the time it was correctly placed with two effective end-tidal capnography waveforms. The ease of insertion was classified based on insertion attempts (1 = first attempt, 2 = second attempt, 3 = third attempt, 4 = intubated and 5 = size change required). Following SAD insertion, a lubricated gastric tube was inserted though the gastric channel (size 12 FG for i-gel, and size 14 FG for both ProSeal and Supreme). Ease of gastric tube insertion was graded on a three-point scale (1 = first attempt, 2 = second attempt and 3 = impossible). If the gastric tube was successfully inserted, gastric content would be aspirated and the amount was recorded. Immediately after correct SAD placement, the oropharyngeal leak pressure was measured once. This was done following full closure of the adjustable pressure valve with a fresh gas flow of 3 L/min. The leak pressure was measured using auscultation, i.e. airway pressure when there is a detectable leak sound in the throat or mouth; the maximum pressure allowed was 40 cmH2O. Patients who were spontaneously breathing during the leak pressure tests were excluded from the study.
Perioperative adverse events and complications (i.e. dental, lip or tongue injury; oxygen desaturation; ventilation problems; laryngospasm; and aspiration/regurgitation) were also documented. At the end of the procedure, the SAD was removed upon eye opening by the patient. The airway device was inspected for any evidence of blood or gastric content. The patient was then asked, one hour later in the recovery room and the following day, to report any sore throat, hoarseness of voice or dysphagia. These symptoms were graded as mild, moderate or severe.
The primary comparison parameter was oropharyngeal leak pressure. Sample size was estimated from a previous similar study that detected oropharyngeal leak pressure differences among the i-gel (mean ± standard deviation [SD] = 28.3 ± 2.4 cmH2O), ProSeal (mean ± SD = 25.0 ± 2.3 cmH2O) and Supreme (mean ± SD = 25.0 ± 1.9 cmH2O) SADs, p < 0.001; that study used a sample size of 35 patients in each group at 30 minutes upon insertion.(9) Therefore, we recruited 50 patients for each group and expected a similar effect size at the 0.05 level of significance with a power of 100%. Statistical analysis was performed using IBM SPSS Statistics version 20.0 for Macintosh (IBM Corp, Armonk, NY, USA). Continuous variables were reported as mean ± standard error of the mean (SEM) and categorical variables were reported as number (percentage). Normality for continuous variables in groups was determined by Shapiro-Wilk test. One-way analysis of variance, Dunnett’s test and Kruskal-Wallis analysis of variance with post hoc analysis were used for comparison of continuous variables among groups. Pearson’s chi-square test was used to compare categorical variables among studied groups. A value of p < 0.05 was deemed statistically significant.
RESULTS
A total of 150 patients were included in the study and no patients dropped out. Their demographic data and airway characteristics, as well as surgery information, are summarised in
Table I
Characteristics of patients and surgery (n = 150).
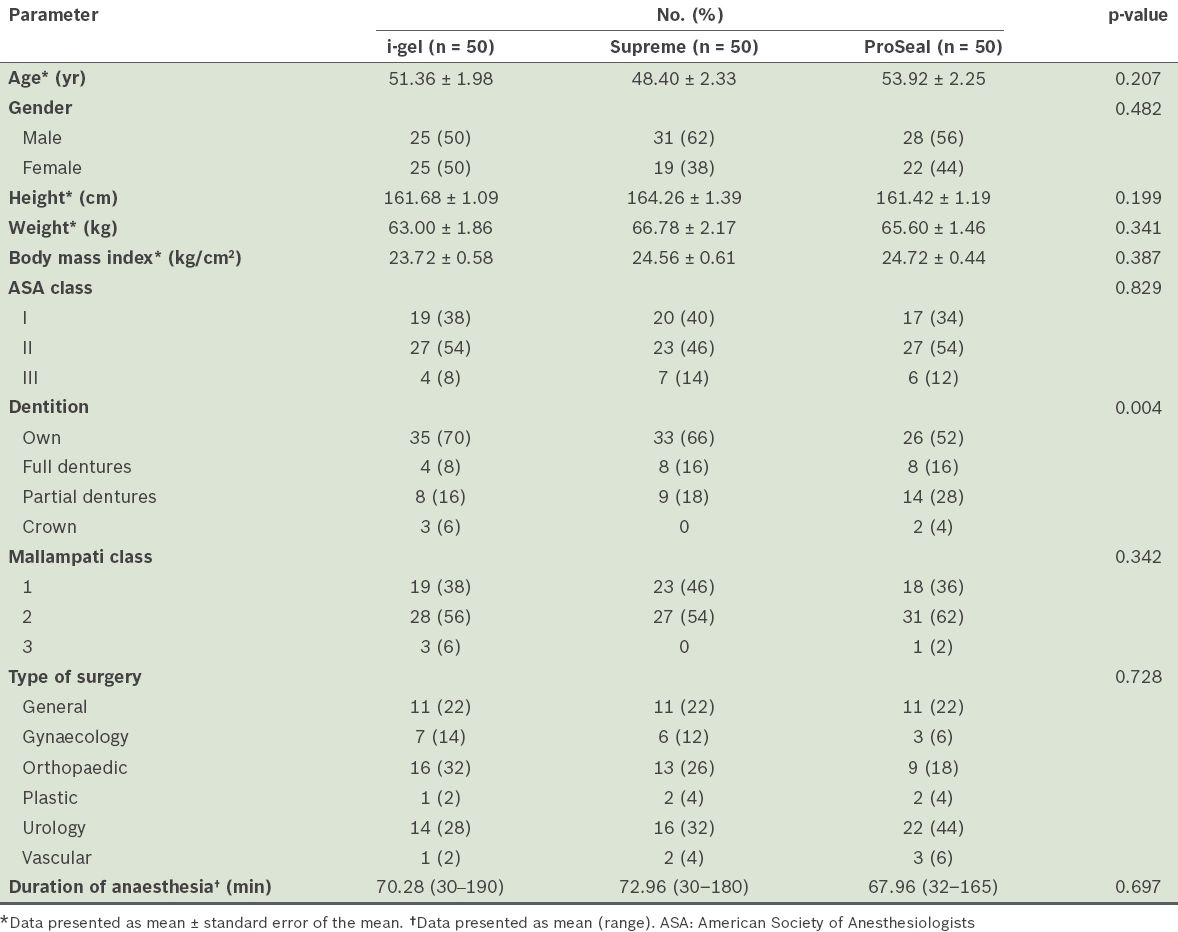
Table II
Airway insertion characteristics, oropharyngeal leak pressure and ventilatory parameters of the supraglottic airway devices (SADs) (n = 150).
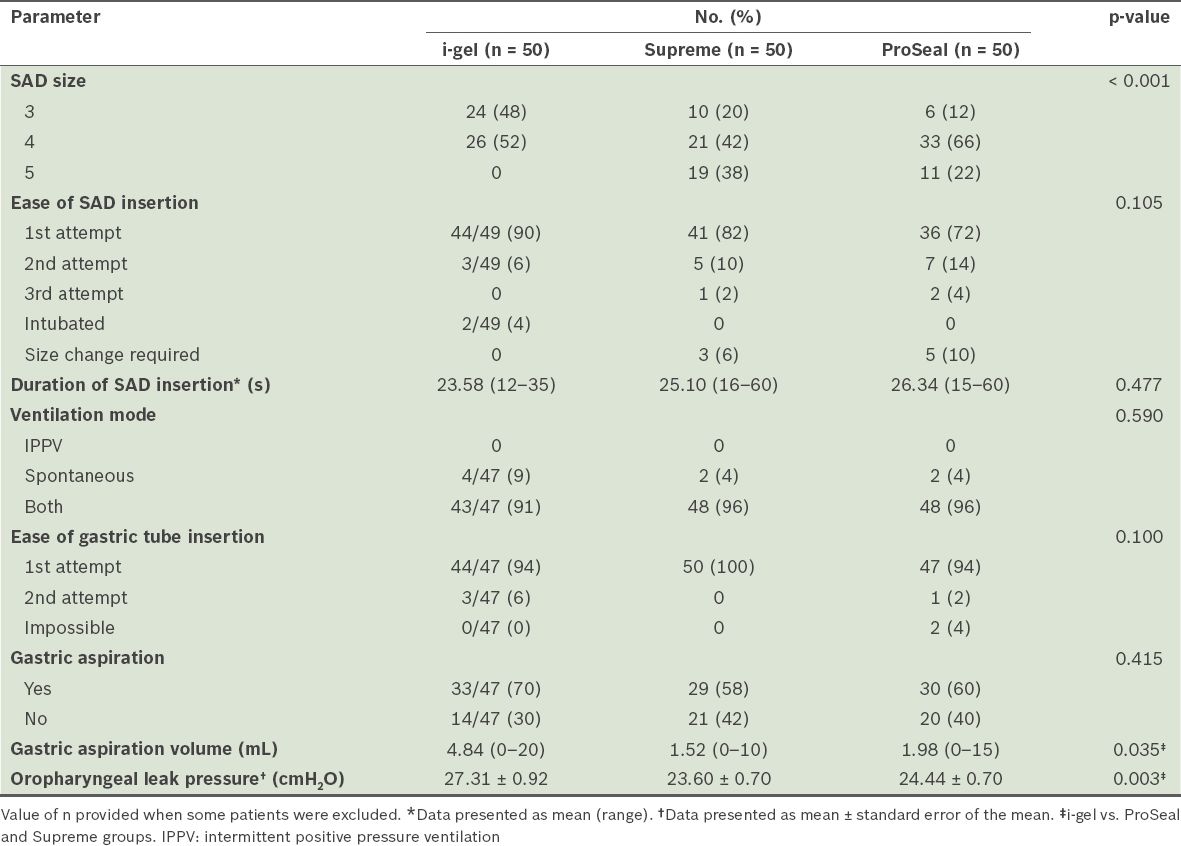
Most airway insertion characteristics and ventilatory parameters were similar among the three groups (
Intraoperative and postoperative complications among the groups are compared in
Table III
Intraoperative and postoperative complications of each group (n = 150).
DISCUSSION
In the present study, we found that the mean oropharyngeal leak pressure following induction was higher in the i-gel group (27.31 cmH2O) than the Supreme (23.60 cmH2O) and ProSeal (24.44 cmH2O) groups. In general, it is thought that higher oropharyngeal leak pressures in SADs allow the use of safer controlled ventilation at higher airway pressures if required.(10) Our finding was in contrast to those of previous studies comparing all three devices. Van Zundert et al evaluated the three devices in 150 patients and demonstrated that the mean leak pressure of the i-gel, measured immediately after insertion, was the lowest (30 cmH2O) among the three airway devices.(8) Likewise, Mukadder et al, who also studied the three devices in 150 patients, similarly showed that the initial leak pressure was lower in the i-gel (21 cmH2O) group; however, the leak pressures of the Supreme and ProSeal groups were 24.90 cmH2O and 23.90 cmH2O, respectively, which were similar to the leak pressures recorded in our study.(9)
A possible reason for the i-gel’s higher leak pressure in our study, as compared with previous studies, is the modification applied to its weight-based size selection criteria to account for the 10-kg overlap between sizes 3 and 4. Nevertheless, there was a higher incidence of significant air leakage in the i-gel group, with three cases of the size 3 i-gel as opposed to none in the other devices. This could be due to the cuffless and gel-like nature of the i-gel, which makes it more prone to air leaks if the anatomical fit is insufficient for oesophageal and pharyngeal seals. Interestingly, a recent meta-analysis comparing the i-gel and ProSeal SADs demonstrated that when a neuromuscular blocker was used, the leak pressure of the ProSeal was higher than that of the i-gel SAD. However, there was no statistical difference in leak pressure when a neuromuscular blocker was not used.(11) Our study did not use neuromuscular blockers during anaesthetic induction, as the types of surgical cases in our study did not warrant their use for muscle relaxation or surgical access. All our patients were either spontaneously breathing from the outset or resumed spontaneous ventilation after a short period of controlled ventilation. Notably, there is some evidence in the literature that spontaneous ventilation can allow a malpositioned LMA to remain undetected until a check is conducted with controlled ventilation, and that the folded epiglottis is more likely to have high airway pressure and leakage with controlled than spontaneous ventilation.(12,13)
We found that the i-gel was easier to successfully insert at the first attempt. It was also associated with shorter effective airway time than the ProSeal and Supreme SADs (
The gastric tubes were inserted successfully at the first attempt in all patients in the Supreme group, and with a 94% success rate in both the i-gel and ProSeal groups. In 2 (4%) patients in the ProSeal group, gastric tube passage was impossible. The insertion of gastric tubes in the i-gel group was slightly more difficult than in the Supreme group despite the use of a smaller 12 FG tube, due to the narrower gastric port. Mukadder et al showed in their study that gastric tube insertion had a similar success rate for the i-gel and Supreme groups, but was more difficult with the ProSeal group.(9) Teoh et al demonstrated no difference in the success rate of gastric tube insertion for the Supreme and i-gel groups.(12) A number of other studies reported gastric tube insertion failure in patients who used ProSeal, although it has not been reported in i-gel patients.(16,17,22)
Less airway morbidity and fewer complications were observed in the i-gel group as compared with the other two devices in our study. Blood staining of the airway device, which could be indicative of airway mucosal trauma, was observed in the ProSeal and Supreme groups, but not in the i-gel group. Furthermore, postoperative complaints of sore throat, voice hoarseness and dysphagia were either less evident or not observed in the latter group. Similar to our findings, the i-gel group in Mukadder et al’s study had fewer reports of blood staining and other postoperative complications.(9) These findings have been demonstrated by other studies as well.(23,24) The i-gel SAD has a non-inflatable cuff that was designed to provide an anatomical fit over the perilaryngeal structures, minimising the risk of compression of neurovascular structures in these tissues and thereby reducing the incidence of airway complications.(25,26)
Our study had several limitations. Firstly, it was unblinded, as the investigators could not be blinded during airway management, hence presenting the possibility of researcher bias. Secondly, the oropharyngeal leak pressure was only measured once, at the start of the procedure, although the leak pressure may change over time. The reason for not measuring leak pressure repeatedly was that the unparalysed patients would only be ventilated for a short period of time before resuming spontaneous breathing, hence only the initial leak pressure was deemed important. In contrast to other similar studies, we did not perform bronchoscopy through the airway device to visualise the laryngeal image. We felt that it was logistically difficult and time-consuming to perform bronchoscopy for all patients; it was also not representative of the daily practice of our unit, given its high caseload and patient turnover. For the purpose of our study, SADs were not reinserted following failed gastric tube insertion if there were no ventilation issues. However, it must be noted that a failure to insert the gastric tube might indicate an incorrectly placed SAD, which might affect the oropharyngeal leak pressure.
In conclusion, our study demonstrated that the ProSeal, Supreme and i-gel SADs can provide a safe airway. We also showed that although the three devices were comparable in terms of ease and duration of placement, the i-gel SAD produced superior results in initial oropharyngeal leak pressure and airway morbidity compared with the ProSeal and Supreme SADs.