

Abstract
Major depression is a common condition seen in the primary care setting. This article describes the suicide risk assessment of a depressed patient, including practical aspects of history-taking, consideration of factors in deciding if a patient requires immediate transfer for inpatient care and measures to be taken if the patient is not hospitalised. It follows on our earlier article about the approach to management of depression in primary care.
Judy, your regular patient, visited your clinic for follow-up of her diabetic condition. Throughout the consultation, you noticed that her head was lowered. She was not her usual cheerful self and avoided eye contact with you. You recalled that she had recently undergone a divorce and had been struggling to get back into the workforce for the past three months. You probed further and found out that she was depressed. You were concerned that she might be suicidal.
HOW RELEVANT IS THIS TO MY PRACTICE?
Major depression is a risk factor for suicide, accounting for up to 60% of suicides.(1-4) The literature has shown that a large proportion of patients who died by suicide had made contact with a primary care health provider within the three months preceding their deaths.(5-7) Patients who died by suicide were also more likely to visit their primary care practitioner than a psychiatrist.(6) This suggests that primary care practitioners are in a unique position to identify at-risk individuals and possibly intervene.(6,8,9) Primary care practitioners have been identified as one of the key potential gatekeepers in suicide prevention efforts.(10) Despite this, not all primary care practitioners routinely ask about suicide in depressed patients.(11)
WHAT CAN I DO IN MY PRACTICE?
There are concerns that enquiring about suicide in patients who are depressed may trigger suicide, but evidence has shown this to be untrue.(12) Acknowledging and discussing suicide may reduce, instead of aggravate, suicidal ideation. Asking about suicide may help primary care physicians to identify high-risk patients who require urgent intervention (such as hospitalisation) and to uncover risk factors, some of which are amenable to intervention.(9)
There are numerous tools to screen for suicide risk. One of the more widely used suicide assessment tools is the SAD PERSONS scale. This is a ten-item mnemonic, which was first developed as a tool for medical students and non-psychiatrist physicians to guide suicide risk assessment.(13) The use of the tool has been found to improve identification of persons with suicidal ideation.(14) The letters in the mnemonic represent demographic, behavioural and psychosocial risk factors for suicide (
Box 1
SAD PERSONS scale for assessment of suicide risk:
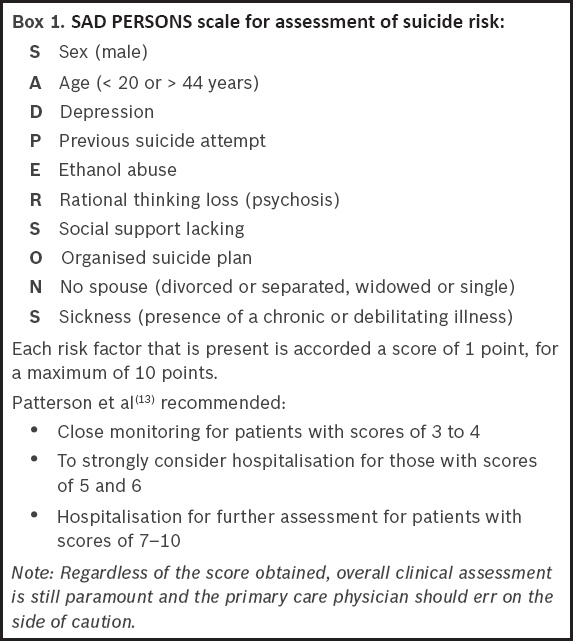
Information acquired via such assessment tools can add to the overall information obtained during a thorough suicide assessment. However, a systematic review concluded that there was insufficient evidence for the usefulness of suicide risk screening tools and that suicide assessment tools should not replace a thorough suicide assessment.(16) According to the recommendations of the Royal College of Psychiatrists, suicide risk assessment tools “should be seen as part of routine assessment and not as a separate exercise”.(17)
Evaluation should be customised and performed in a manner that is sensitive to the patient’s culture and religion. It should also take into consideration any risk factors and warning signs. Clinical judgement is important, and the clinician should err on the side of caution. Thorough documentation and communication of details is important to ensure adequate monitoring and the safety of the person.(18) Assessing the patient’s suicide risk involves: (a) checking for known risk factors of suicide; (b) eliciting suicidal ideation from the patient (or corroborative sources); and (c) deciding if the patient is at imminent risk of suicide, based on the patient’s current ideation and existing risk factors.(19)
Checking for suicide risk factors
Some of the risk factors for suicide are amenable to intervention, whereas others are not. A large prospective study identified hopelessness, higher levels of suicidal ideation, recurrent episodes of depression, presence of personality disorders, previous psychiatric hospitalisation, older age, unemployed status and a family history of suicide as significant markers for suicide.(20) Having one or more previous suicide attempts is a very strong predictor of suicide risk.(21) Having pervasive thoughts of hopelessness has also been identified as a very important risk factor.(22,23) Additional risk factors include the presence of other psychiatric comorbidities such as anxiety disorders and substance misuse,(10,24) chronic physical illnesses,(25) a recent stressful life event,(26) and social isolation,(27) which includes living alone, coming from a broken family, divorce and spousal bereavement. Access to lethal means is another risk factor; the most common mode of suicide in Singapore is jumping from heights, followed by hanging and poisoning.(28) The risk factors for suicide are summarised in
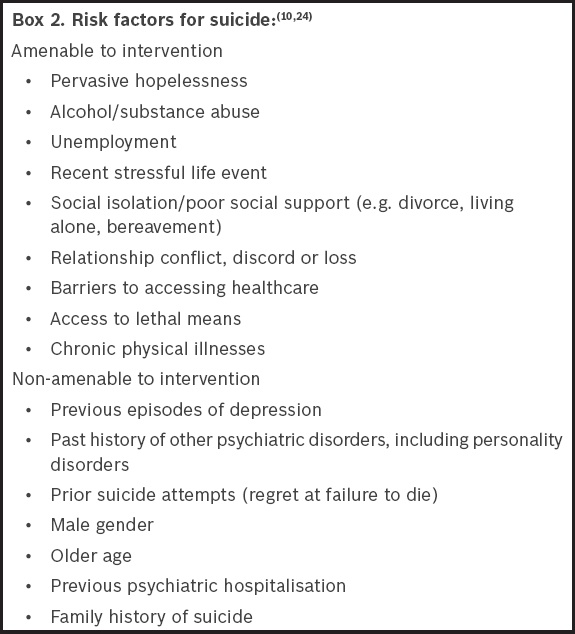
In contrast to risk factors, protective factors lower the risk of suicide. Therefore, apart from strategies to reduce the risk factors for suicide, interventions should aim to strengthen factors that protect against suicide. These include strong interpersonal relationships, religious faith, positive coping strategies such as effective stress management and healthy lifestyle choices, including diet and exercise.(10,29)
Eliciting suicidal ideation
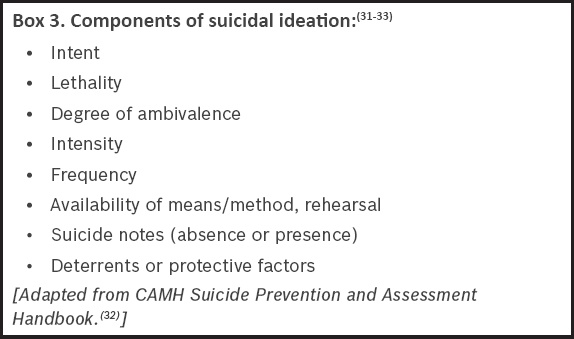
There are no fixed methods to elicit suicidal ideation. Some patients may inform the doctor without the need for prompting, while others may view it with shame. Therefore, it is prudent to raise the topic carefully in a sensitive and respectful manner, by first using open-ended questions and gradually focusing on direct ones. It may be easier to broach the subject while exploring mood symptoms or discussing negative feelings. One should be mindful not to overreact even if there is a cause for concern.(30) Important components of suicidal ideation that should be explored are listed in
A step-wise approach (
Fig. 1
Step-wise approach to assessing suicidal ideation.
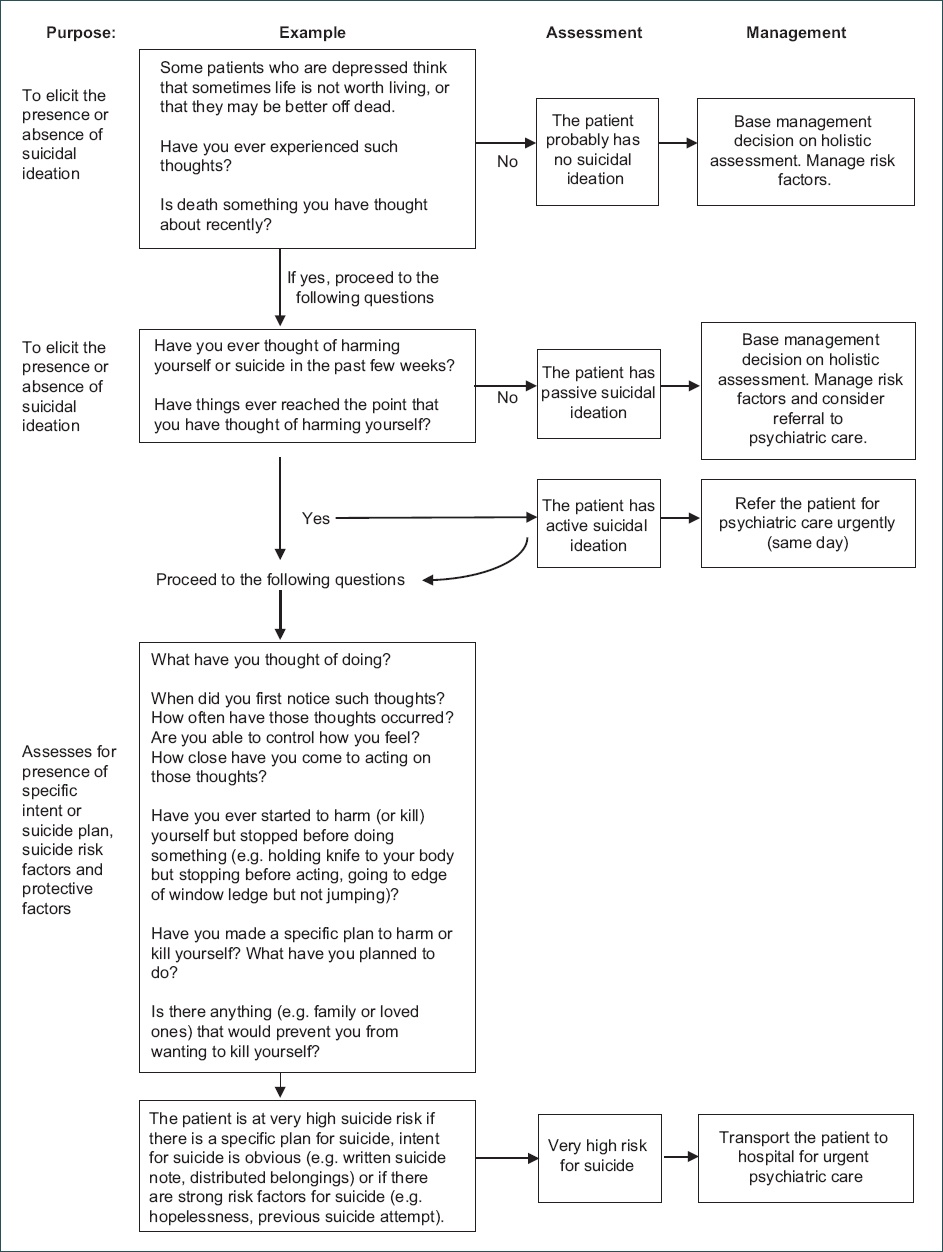
Conversely, if thoughts of self-harm are present, the patient is said to have active suicidal ideation and should be given a same-day psychiatric assessment. The primary care physician should ask further questions to look for behaviour that suggests intent (e.g. making a suicide note or distributing personal belongings), or whether there is a specific plan to carry it out. Any patient who communicates a specific intent or plan for suicide requires urgent psychiatric referral and should be transported to the emergency room.(24) Finally, the risk assessment should be documented as clearly and as thoroughly as possible to facilitate communication between healthcare providers, ongoing assessment and continuity of care.
Cultural aspects relevant to Asia
In Asian society, one may encounter patients who quickly deny or brush off thoughts of suicide due to the fear of stigma or judgement, or because their religious faith forbids them from entertaining such thoughts. Although religious faiths may seem protective, the fear of judgement about harbouring such ideas may serve as a barrier to reporting of suicidal ideation.(35) In such patients, it may be helpful to broach the topic in a gentle, sensitive and normalising manner. This is an example of what one might say to such patients: “This may be a sensitive topic in some religions, but when people are very unhappy or overwhelmed by sadness, they can sometimes experience thoughts that life is not worth living. These thoughts come automatically and are not always controllable. Have you ever experienced anything like this?”
Managing patients with suicide risk
Suicide risk assessment is a complex and challenging process that relies on effective communication, and it is an ongoing process for the depressed patient.(18) Therefore, a holistic approach should be employed. Primary care physicians should base decision-making on clinical judgement and not rely solely on the cut-off scores of the suicidal ideation assessment tool.
The main challenge for the primary care physician is deciding whether the patient should be managed at primary care or referred for tertiary psychiatric care (and the urgency of the latter). All persons with clear-cut active suicidal ideation should be sent to the designated hospital (i.e. Institute of Mental Health in the Singapore context) for urgent psychiatric care. However, when it comes to managing cases that are less clear-cut – such as a patient with passive suicidal ideation following a recent stressor, who has poor support, a past history of self-harm and poor coping skills – decision-making can be difficult. The physician may still decide to send such patients for urgent assessment if the patient is deemed unsafe.
Another potential dilemma that may arise is the issue of confidentiality. Patients may not consent to the doctor informing their family members about their suicide risk. In such cases, if the patient is at imminent risk, the concerns of safety override the considerations of confidentiality.(4,31) However, it is prudent to inform the patient that, in the event of safety concerns, the doctor may be obligated to disclose the patient’s suicide risk to the family or relevant persons for his or her best interests.
Optimising treatment of underlying depressive disorder
For all depressed patients, the management of their underlying depressive disorder, which includes both pharmacological and psychological therapies, should be optimised; antidepressants should be commenced in patients who are not on any medication. Our previous article illustrated the approach to diagnosis of major depression in primary care.(36) The physician should make an effort to look out for any comorbid illnesses, such as chronic physical illnesses, anxiety, substance misuse or personality disorders, which may complicate management. To prevent harmful overdosing, adherence to medication should be checked and strictly supervised, if deemed necessary.
Information to be provided upon transfer
In cases where the patient is required to be transferred for urgent psychiatric care, salient information should be provided to facilitate continuity of care. This includes information on the level of suicide risk and the reason for it, pertinent demographic data, risk factors, mental state examination results, past medical history, medication, treatment plans and social contacts.
Safety plans
Safety plans should be discussed and developed with depressed patients who are at risk of suicide. This usually involves recognising signs of impending suicidal crisis (such as specific triggers or suicidal thoughts), planning coping methods in advance to deal with future suicidal urges, and identifying individuals or agencies (with their respective contact details) that the patient can contact to facilitate patient safety and lower the risk of imminent suicidal behaviour.(32,37) If there is already an existing safety plan, the primary care physician should actively discuss it with the patient, and revisit the plan when there is a change in suicide risk level. However, should the doctor or patient feel that the patient is at imminent risk and unable to remain safe, the patient should immediately be sent to the hospital for urgent psychiatric care.
Another intervention that is commonly used is the ‘no-suicide contract’ or ‘no-harm contract’. No-suicide contracts are not the same as safety plans. They involve statements from patients promising not to harm themselves or that they will contact someone in the event that they are unable to maintain their own safety. Although commonly used, the practice of forming no-suicide contracts should be discouraged, as there is no evidence to suggest that such contracts reduce suicide tendencies, but they may instead be used by patients to hide their actual suicidal intent.(32,38)
Linking patients to community resources
All persons who are depressed or suicidal should be connected to available community resources and crisis helplines.(4,31)
Three months later, you met Judy again and saw that she was visibly better. She told you that she was regularly seeing the psychiatrist that you had referred her to and was glad to have found a support group in the community. She sincerely thanked you for your concern and for providing a listening ear when she had most needed it.
TAKE HOME MESSAGES
-
Suicidal patients are more likely to see a primary care physician than a psychiatrist in the months preceding their death. Primary care physicians are therefore in a unique position to identify at-risk individuals and possibly intervene.
-
Acknowledging and discussing suicide may help to reduce suicidal ideation and identify high-risk patients who require urgent intervention.
-
There are numerous tools available to screen for suicide risk, such as the SAD PERSONS scale. The information acquired can add to the overall information obtained during a thorough suicide assessment.
-
Some suicidal risk factors are amenable to intervention, whereas some are not.
-
Apart from strategies to reduce the risk factors for suicide, interventions should also aim to strengthen the protective factors.
-
Eliciting suicidal ideation requires a step-wise approach, by first using open-ended questions and gradually focusing on direct ones.
-
All persons with clear-cut, active suicidal ideation should be sent to the designated hospital for urgent psychiatric care.
-
Safety plans should be discussed and developed with all patients who are at risk of suicide.
-
Depressed or suicidal patients should be connected to available community resources.
SMJ-58-77.pdf