Author Information >Copyright and License information >
1Department of Gastroenterology and Hepatology, Changi General Hospital, Singapore 2Central 24-HR Clinic Group, Singapore Correspondence: Adj A/Prof Tiing Leong Ang, Chief and Senior Consultant, Department of Gastroenterology and Hepatology, Changi General Hospital, 2 Simei Street 3, Singapore 529889. tiing_leong_ang@cgh.com.sg
Helicobacter pylori (H. pylori) is an infection that has a role in causing dyspepsia and complications such as peptic ulcer disease and gastric malignancies. In the primary care setting, one can adopt a stepwise approach with the ‘test-and-treat’ strategy to manage H. pylori-associated dyspepsia in young patients without alarm symptoms. Empiric first-line therapies should be for a two-week duration; options include clarithromycin-containing triple therapy alone or with the addition of bismuth, concomitant therapy and bismuth quadruple therapy. Post-treatment carbon urea breath test must be performed at least four weeks after the end of treatment to confirm the cure. Options for empiric second-line treatment include bismuth quadruple therapy and levofloxacin-containing triple therapy. Patients with persistent or alarm symptoms should be referred for further evaluation. Patients with persistent infection should be referred for gastroscopy so that gastric biopsies can be obtained for H. pylori culture and antibiotic susceptibility testing.
Keywords: acid suppression, antibiotic resistance, dyspepsia, H. pylori
Jonathan, a 22-year-old undergraduate, has been troubled by dyspepsia in the past few weeks. He initially attributed it to stress from studying for his upcoming university examinations. However, when the symptom persisted, he decided to seek advice from his family physician. He was positive for H. pylori on serological testing and was started on seven-day clarithromycin-based triple therapy. Upon its completion, Jonathan returned for repeat serology, which remained positive. As his symptoms were persistent, his family physician referred him to a gastroenterologist for further management.
HOW RELEVANT IS THIS TO MY PRACTICE?
Helicobacter pylori (H. pylori) is a common chronic bacterial infection that is present in over 50% of the world’s population, although its prevalence has been gradually declining in the Asia-Pacific region.(1) In Singapore, the seroprevalence rate is 31%.(2)
The majority of people infected with H. pylori never experience any symptoms or complications. However, the increasing use of H. pylori serology by family physicians during health screening prompts further investigation for H. pylori. Symptoms include dyspepsia, bloating, and nausea or vomiting. Colonisation with H. pylori is a major risk factor for peptic ulcer disease, as well as gastric malignancies such as gastric adenocarcinoma and lymphoma involving mucosa-associated lymphoid tissue.(3) Successful eradication is essential for primary and secondary prevention of peptic ulcer disease and gastric malignancy.(4,5)
WHAT CAN I DO IN MY PRACTICE?
Diagnosis of H. pylori infection
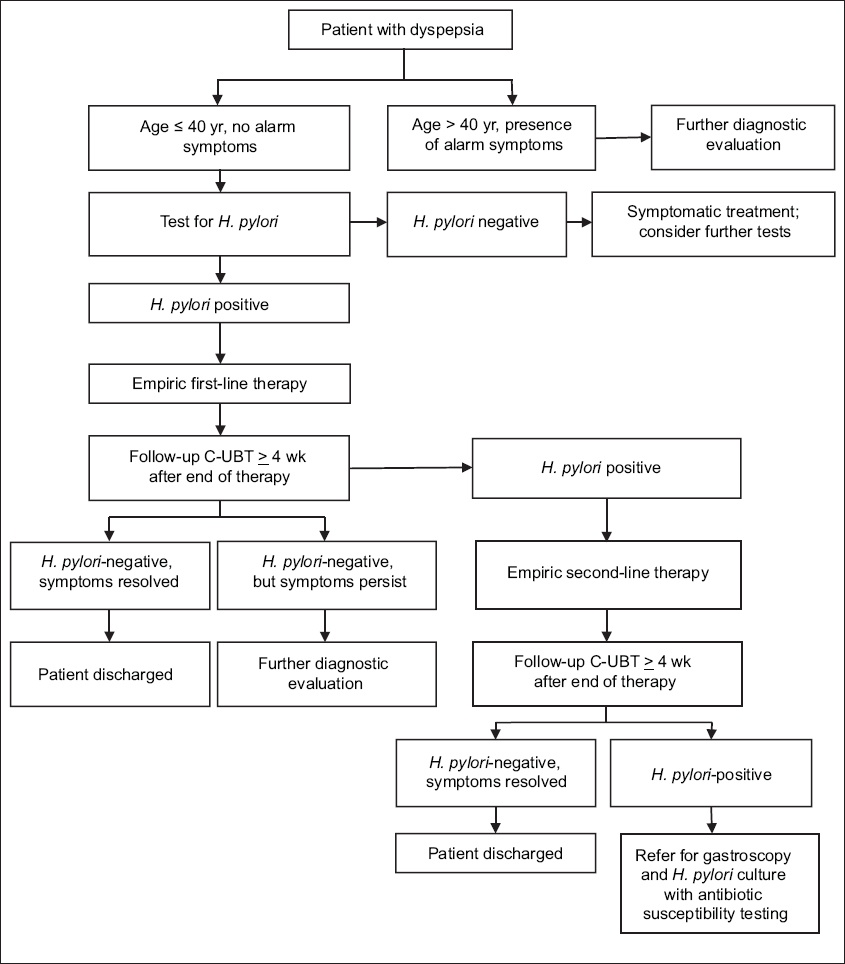
In managing patients with dyspepsia, primary care physicians can take a stepwise approach (Fig. 1). Endoscopy is the first-line investigation in patients with dyspepsia. It can diagnose peptic ulcer disease, gastric malignancies and H. pylori infection through biopsy-based tests such as the rapid urease test and histology. While endoscopy has a high diagnostic yield, its disadvantages include the need for referral to a specialist (i.e. for open-access gastroscopy or formal specialist review), cost, procedure-related risk and the discomfort experienced by patients. General practitioners and family physicians serve an important role in the first-line treatment for such patients, as they can use a noninvasive diagnostic strategy: ‘test and treat’. This is a reasonable option in younger patients without alarm features such as anaemia, loss of weight, anorexia, recent onset of progressive symptoms, melaena or haematemesis, and dysphagia.(6-10) The age threshold depends on the local prevalence of gastric malignancies. In Singapore, the ‘test-and-treat’ strategy is a reasonable option for patients who are aged 40 years and below.
Fig. 1
Flow chart shows the stepwise approach to management of H. pylori-associated dyspepsia in the primary care setting. C-UBT: carbon urea breath test
As its name suggests, this strategy is based on investigating for the presence of H. pylori and its subsequent eradication when detected. The patient is assessed for symptom resolution and no further diagnostic evaluation (with endoscopy or referral) is needed if the symptoms have fully resolved. The carbon urea breath test (C-UBT) is considered the best approach for the initial diagnosis and subsequent confirmation of the cure, as it has high sensitivity and specificity, excellent performance, and is cost-effective.(11,12) C-UBT is based on the principle that H. pylori will hydrolyse orally administered labelled urea to produce carbon dioxide that is isotopically labelled and can be measured in exhaled breath. As H. pylori is the most common urease-containing gastric pathogen, the presence of urea hydrolysis confirms a H. pylori infection. Two types of C-UBT are available: 13C-UBT and 14C-UBT. 13C-UBT is preferred as it is non-radioactive and based on mass spectrometry, whereas 14C-UBT is radioactive.
Routine ‘test and treat’ is not recommended for patients with gastro-oesophageal reflux disease.(13) An alternative to C-UBT is stool antigen testing, which is particularly useful for children who may not be able to comply with C-UBT. The monoclonal stool antigen test has high sensitivity and specificity, and has been shown to be the most effective noninvasive test for children.(14,15) For adults, C-UBT is preferred.
Serological assays are inexpensive and easy to conduct in the primary care setting.(16,17) However, the performance of these tests is dependent on the antigenic composition of circulating strains and thus, they need to be validated for the local population. Furthermore, as these tests cannot differentiate between active and past infection, they are not recommended for diagnosis of active infection or confirmation of eradication. False positive tests may result in overuse of antibiotics and potentially contribute to antimicrobial resistance.(4,18)
Empiric first-line treatment
The determinants of treatment efficacy are adequate treatment duration, at least two different antibiotics, potent acid suppression, compliance to treatment and antibiotic resistance. When the first set of Ministry of Health Clinical Practice Guidelines for H. pylori treatment was published, one-week triple therapy was recommended, comprising twice-daily proton pump inhibitor (PPI), amoxicillin and clarithromycin.(19) These guidelines are now obsolete and have been withdrawn. Since then, studies have shown that a two-week clarithromycin-containing triple-therapy regimen increases cure rates compared to both ten-day and one-week therapy regimens.(20) Potent acid suppression is an important element of triple therapy. Twice-daily PPI therapy increases the efficacy of triple therapy, because H. pylori enters a replicative state after gastric pH is raised and thus, becomes more susceptible to amoxicillin and clarithromycin.(21-24) However, compliance to treatment is very important and clinicians must educate patients on the consequences of noncompliance; a compliance rate of less than 80% has been shown to lower treatment efficacy.
An important cause of treatment failure is H. pylori antibiotic resistance, which is increasing in most parts of the world.(25) Resistance to clarithromycin, in particular, is responsible for a decrease in the efficacy of current triple-therapy regimens.(25-27) As antibiotic resistance profiles vary across geographical regions, knowledge of local resistance patterns and treatment outcomes is important.(26,28) A recent study of H. pylori resistance profiles in Singapore found that in the time periods of 2000–2002 and 2012–2014, resistance rates to clarithromycin (7.9% to 17.1%), metronidazole (24.8% to 48.2%) and levofloxacin (5.0 to 14.7%) have increased, whereas resistance to amoxicillin (3.0% to 4.1%) and tetracycline (5.0% to 7.6%) remained low. Multidrug resistance rates were low during these periods.(2)
The recently published Maastricht V/Florence Consensus Report recommended that in areas of high clarithromycin resistance (> 15%), bismuth quadruple therapy or a non-bismuth quadruple therapy called concomitant therapy (PPI, amoxicillin, clarithromycin and a nitroimidazole) be recommended.(4) It is also generally regarded that in the context of quadruple therapies, the effect of metronidazole resistance can be overcome if a higher dose of 500 mg three times a day is used for two weeks.(4) The Toronto Consensus Report further clarified the issue by including outcome data, stating that to continue using clarithromycin-containing triple therapy, the clarithromycin resistance rate should either be less than 15%, or there should be local data demonstrating high eradication rates (> 85%).(29)
A recent randomised controlled study in Singapore compared concomitant (PPI, amoxicillin, clarithromycin and metronidazole), sequential (PPI, amoxicillin for the first five days, followed by PPI, clarithromycin and metronidazole for the subsequent five days) and triple (PPI, amoxicillin and clarithromycin) therapies for ten days. All three regimens achieved high eradication rates of more than 90% even though the rate of clarithromycin resistance in Singapore had risen to 17.1% during the study period.(30) This suggests that two-week clarithromycin-containing triple therapy is currently a viable first-line empiric treatment option in Singapore, despite the rise in the clarithromycin resistance rate. However, the efficacy is likely to decrease should clarithromycin resistance rates increase further and exceed 20%.
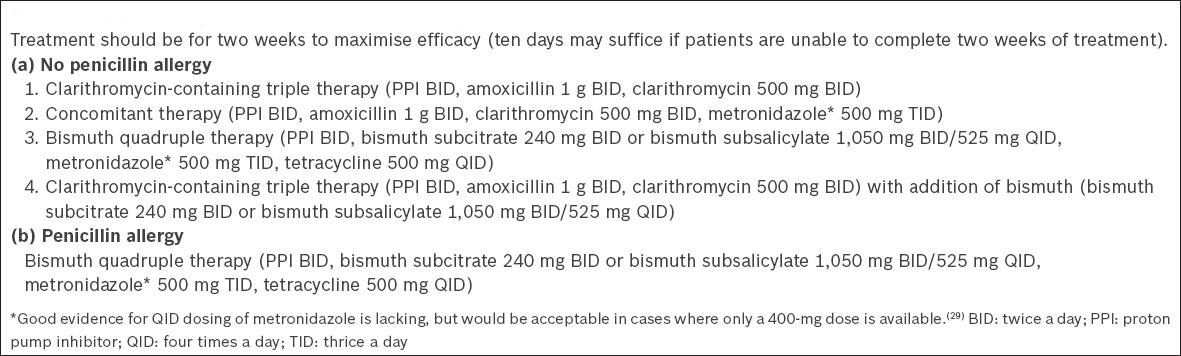
Other first-line options include concomitant therapy and bismuth quadruple therapy. Sequential therapy is not recommended. Interestingly, in countries with high antibiotic resistance rates, the addition of bismuth to standard triple therapy further increased treatment efficacy due to the bactericidal properties of bismuth, although no local data is available.(31) Issues with these alternative regimens include added costs and lower patient tolerability. Vigilance and follow-up C-UBT are important when triple therapy is used. In cases of penicillin allergy, it is theoretically possible to replace amoxicillin with metronidazole in clarithromycin-containing triple therapy, but this is not ideal given the high local antibiotic resistance rates, and bismuth quadruple therapy should be preferred. The options for empiric first-line treatment in Singapore are summarised in Box 1.
Box 1
Options for empiric first-line treatment of H. pylori.
Testing for H. pylori eradication
C-UBT is the test of choice for confirming successful eradication of H. pylori infection after treatment. False negative C-UBT results can occur in patients taking PPI and antibiotics.(32) Therefore, it is advisable to perform C-UBT at least four weeks after completion of antibiotic therapy; patients should also have discontinued PPI therapy for at least two weeks.(33) As with diagnosis of H. pylori, the stool antigen test is an acceptable alternative. However, serological testing should not be used for confirmation of eradication, as the levels will remain positive.(4)
WHEN SHOULD I REFER FOR GASTROSCOPY?
Referral for gastroscopy should be considered when patients present with alarm symptoms, or when the ‘test-and-treat’ strategy is unsuccessful and persistent infection is suspected. There are several endoscopy-based biopsy tests for H. pylori infection. Among these, the rapid urease test is recommended as a first-line test, as it has a high sensitivity and specificity of 90% and 95%–100%, respectively, and results are quickly confirmed.(34,35) If the test is positive, treatment can be started immediately after endoscopy. Biopsies can also be obtained for histology, for diagnosis of H. pylori infection and topographical mapping of the extent and severity of gastritis, including the presence and severity of gastric atrophy and intestinal metaplasia. This information allows risk stratification for development of subsequent gastric dysplasia.(36,37,38) However, histology is not routinely required nor performed, given the additional costs involved and longer turnaround time. Biopsies from both the antrum and corpus are recommended to increase the sensitivity of the rapid urease test.(39)
When patients are referred for gastroscopy and a rapid urease test is likely to be performed, they should be advised to avoid taking antibiotics or bismuth for four weeks and PPI therapy for two weeks.(4) When there is a concern that the rapid urease test might return a false negative due to recent use of PPI or antibiotics, additional biopsies for histology can be obtained.
WHAT ARE THE SECOND-LINE TREATMENT OPTIONS?
Second-line treatment may be prescribed empirically in primary care or specialist settings. If endoscopy is scheduled, gastric biopsies may be obtained for H. pylori culture and antibiotic susceptibility testing to guide the choice of antibiotic therapy.(4)
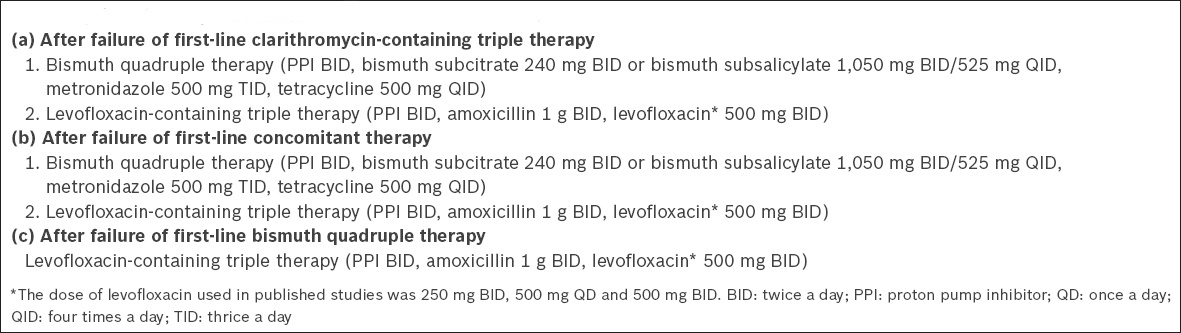
For patients who fail treatment with clarithromycin-containing triple therapy, clarithromycin resistance should be suspected, and second-line therapy should be considered.(4) Bismuth quadruple therapy or levofloxacin-containing therapy (PPI, amoxicillin and levofloxacin) are both acceptable second-line therapies for these patients.(40) However, high resistance rates to levofloxacin in the local setting may affect the efficacy of levofloxacin-based regimens.(2,41)
For patients who fail initial treatment with non-bismuth quadruple therapy, meta-analyses have shown PPI-levofloxacin-amoxicillin therapy to be the most effective rescue therapy, with a 78% eradication rate.(4) However, the efficacy of this regimen is reduced in the presence of fluoroquinolone resistance,(41) which appears to be rising in Singapore.(2) A quadruple regimen with the addition of bismuth has been shown to be useful, likely due to the synergistic effect of bismuth with antibiotics in overcoming clarithromycin and levofloxacin resistance.(42,43) The options for empiric second-line treatment in Singapore are summarised in Box 2.
Box 2
Options for empiric second-line treatment of H. pylori.
Failure of second-line treatment
Referral to a specialist for assessment and antibiotic susceptibility testing is indicated for patients who fail second-line treatment. Gastroscopy will have to be performed and biopsies obtained for H. pylori culture.(44,45) It is important that treatment compliance is explored with these patients and any barriers to compliance are addressed.
As treatments for H. pylori infection are constantly evolving, there is a need to maintain an up-to-date approach in our management. The profile of antibiotic resistance in Singapore should be re-evaluated at regular intervals, as it may affect the efficacy of empiric first-line treatment regimes. For instance, recent data revealed that the clarithromycin resistance in Singapore is above the threshold level of 15%, suggesting that the use of clarithromycin as first-line empirical therapy may need to be reconsidered.(2) However, despite this increase in the resistance rate, clarithromycin-containing triple therapy was demonstrated to achieve eradication rates of more than 90% in the local context in a randomised controlled study. Hence, it can still be recommended as first-line therapy.(30) Post-treatment C-UBT must be performed routinely in all patients at least four weeks after treatment to confirm the cure, as no regimen can consistently achieve a 100% treatment success rate.
CONCLUSION
Generally, vaccination is the best public health measure against infections. In the context of H. pylori infection, vaccination is not universally available and the efficacy is limited, although a promising field trial in China has recently been reported.(46) In the primary care setting, one can adopt a stepwise approach to the management of H. pylori-associated dyspepsia (Fig. 1). The ‘test-and-treat’ strategy can be considered in younger patients without alarm symptoms; however, further evaluation must be performed should symptoms persist. Clarithromycin-containing triple therapy for two weeks can still be an empiric first-line therapy for H. pylori infection in Singapore. For patients unable to tolerate two-week therapy, ten days may suffice in the local context.(30) Other options for empiric first-line treatment include bismuth quadruple therapy and concomitant therapy. Referral for gastroscopy is indicated in patients with alarm symptoms or those with persistent infection. Confirmation of eradication is mandatory for all patients after treatment. Patient education is important and clinicians should reinforce the importance of treatment compliance and educate patients on the risks and complications of persistent H. pylori infection.
TAKE HOME MESSAGES
H. pylori infection is a common condition, and treatment is important for the primary and secondary prevention of complications, which range from peptic ulcer disease to gastric malignancy.
‘Test and treat’ is an acceptable strategy for younger patients who have uninvestigated dyspepsia without alarm symptoms. C-UBT has high sensitivity and specificity for active infection.
Patients with alarm symptoms or persistent infection should be referred for gastroscopy.
Clarithromycin-containing triple therapy for two weeks is an acceptable first-line empirical treatment for H. pylori infection in Singapore. Patients who fail to respond to treatment should be prescribed bismuth quadruple therapy. C-UBT should be performed at least four weeks after treatment to confirm the cure.
Bismuth quadruple therapy and concomitant therapy are recommended first-line treatment options in regions of high clarithromycin resistance.
Local antibiotic resistance patterns must be re-evaluated at regular intervals to guide the choice of empiric treatment. Compliance to treatment is important and clinicians must reinforce this by actively educating and engaging the patient.
Jonathan underwent gastroscopy, which showed non-erosive antral gastritis. Biopsies were taken and the rapid urease test confirmed the presence of persistent H. pylori infection. Upon further questioning, Jonathan revealed that he had not been compliant to the initial course of clarithromycin-based triple therapy, as he had often forgotten to take his medications when he was studying. He was counselled on the risks of persistent H. pylori infection and agreed to start on bismuth-based quadruple therapy for 14 days. A repeat carbon urea breath test performed by his family physician confirmed successful eradication of H. pylori.
References Tonkic A, Tonkic M, Lehours P, Mégraud F.Epidemiology and diagnosis of Helicobacter pylori infection.Helicobacter. 2012; 17:Suppl 11-8. Ang TL, Fock KM, Ang D, et al. The changing profile of Helicobacter pylori antibiotic resistance in Singapore: a 15-year study.Helicobacter. 2016; 21:261-5. Suerbaum S, Michetti P.Helicobacter pylori infection.N Engl J Med. 2002; 347:1175-86. Malfertheiner P, Megraud F, O’Morain CA, et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report.Gut. 2017; 66:6-30. Gisbert JP, Khorrami S, Carballo F, et al. Meta-analysis: Helicobacter pylori eradication therapy vs. antisecretory non-eradication therapy for the prevention of recurrent bleeding from peptic ulcer.Aliment Pharmacol Ther. 2004; 19:617-29. Ford AC, Qume M, Moayyedi P, et al. Helicobacter pylori ‘test and treat’ or endoscopy for managing dyspepsia: an individual patient data meta-analysis.Gastroenterology. 2005; 128:1838-44. Arents NLA, Thijs JC, van Zwet AA, et al. Approach to treatment of dyspepsia in primary care: a randomized trial comparing ‘test-and-treat’ with prompt endoscopy.Arch Intern Med. 2003; 163:1606-12. Duggan AE, Elliott CA, Miller P, Hawkey CJ, Logan RF.Clinical trial: a randomized trial of early endoscopy, Helicobacter pylori testing and empirical therapy for the management of dyspepsia in primary care.Aliment Pharmacol Ther. 2009; 29:55-68. Lassen AT, Pedersen FM, Bytzer P, Schaffalitzky de Muckadell OB.Helicobacter pylori test-and-eradicate versus prompt endoscopy for management of dyspeptic patients: a randomised trial.Lancet. 2000; 356:455-60. McColl KE, Murray LS, Gillen D, et al. Randomised trial of endoscopy with testing for Helicobacter pylori compared with non-invasive H pylori testing alone in the management of dyspepsia.BMJ. 2002; 324:999-1002. Gisbert JP, Calvet X.Helicobacter pylori ‘test-and-treat’ strategy for management of dyspepsia: a comprehensive review.Clin Transl Gastroenterol. 2013; 4:e32. Nocon M, Kuhlmann A, Leodolter A, et al. Efficacy and cost-effectiveness of the 13C-urea breath test as the primary diagnostic investigation for the detection of Helicobacter pylori infection compared to invasive and non-invasive diagnostic tests.GMS Health Technol Assess. 2009; 5:Doc14. Fock KM, Katelaris P, Sugano K, et al. Second Asia-Pacific conferenceSecond Asia-Pacific Consensus Guidelines for Helicobacter pylori infection.J Gastroenterol Hepatol. 2009; 24:1587-600. Gisbert JP, de la Morena F, Abraira V.Accuracy of monoclonal stool antigen test for the diagnosis of H. pylori infection: a systematic review and meta-analysis.Am J Gastroenterol. 2006; 101:1921-30. Kato S, Ozawa K, Okuda M, et al. Accuracy of the stool antigen test for the diagnosis of childhood Helicobacter pylori infection: a multicenter Japanese study.Am J Gastroenterol. 2003; 98:296-300. Feldman RA, Deeks JJ, Evans SJ.Multi-laboratory comparison of eight commercially available Helicobacter pylori serology kits. Helicobacter pylori Serology Study Group.Eur J Clin Microbiol Infect Dis. 1995; 14:428-33. Burucoa C, Delchier JC, Coallon-Mallet A, et al. Comparative evaluation of 29 commercial Helicobacter pylori serological kits.Helicobacter. 2013; 18:169-79. Duggan AE, Elliott C, Logan RF.Testing for Helicobacter pylori infection: validation and diagnostic yield of a near patient test in primary care.BMJ. 1999; 319:1236-9. Fock KM, Yeoh KG, Lim CC, et al. Clinical practice guidelines: management of Helicobacter pylori infection.Ministry of Health Clinical Practice Guidelines 9 [online]. Available at: https://www.moh.gov.sg/content/dam/moh_web/HPP/Doctors/cpg_medical/withdrawn/cpg_Management%20of%20Helicobacter%20pylori%20Infection-Sep%202004.pdf. Accessed April 21 2017. Calvet X, García N, López T, et al. A meta-analysis of short versus long therapy with a proton pump inhibitor, clarithromycin and either metronidazole or amoxycillin for treating Helicobacter pylori infection.Aliment Pharmacol Ther. 2000; 14:603-9. Labenz J.Current role of acid suppressants in Helicobacter pylori eradication therapy.Best Pract Res Clin Gastroenterol. 2001; 15:413-31. Villoria A, Garcia P, Calvet X, et al. Meta-analysis: high-dose proton pump inhibitors vs. standard dose in triple therapy for Helicobacter pylori eradication.Aliment Pharmacol Ther. 2008; 28:868-77. Vallve M, Vergara M, Gisbert JP, Calvet X.Single vs. double dose of a proton pump inhibitor in triple therapy for Helicobacter pylori eradication: a meta-analysis.Aliment Pharmacol Ther. 2002; 16:11490-56. Huang J, Hunt RH.The importance of clarithromycin dose in the management of Helicobacter pylori infection: a meta-analysis of triple therapies with a proton pump inhibitor, clarithromycin and amoxycillin or metronidazole.Aliment Pharmacol Ther. 1999; 13:719-29. Fischbach L, Evans EL.Meta-analysis: the effect of antibiotic resistance status on the efficacy of triple and quadruple first-line therapies for Helicobacter pylori.Aliment Pharmacol Ther. 2007; 26:343-57. Ierardi E, Giorgio F, Losurdo G, Di Leo A, Principi M.How antibiotic resistances could change Helicobacter pylori treatment: a matter of geography?.World J Gastroenterol. 2013; 19:8168-80. Graham DY, Lee YC, Wu MS.Rational Helicobacter pylori therapy: evidence-based medicine rather than medicine-based evidence.Clin Gastroenterol Hepatol. 2014; 12:177-86. Ghotaslou R, Leylabadlo HE, Asl YM.Prevalence of antibiotic resistance in Helicobacter pylori: a recent literature review.World J Methodol. 2015; 5:164-74. Fallone CA, Chiba N, van Zanten SV, et al. The Toronto Consensus for the treatment of Helicobacter pylori infection in adults.Gastroenterology. 2016; 151:51-69. Ang TL, Fock KM, Song M, et al. Ten-day triple therapy versus sequential therapy versus concomitant therapy as first-line treatment for Helicobacter pylori infection.J Gastroenterol Hepatol. 2015; 30:1134-9. Dore MP, Lu H, Graham DY.Role of bismuth in improving Helicobacter pylori eradication with triple therapy.Gut. 2016; 65:870-8. Gatta L, Vakil N, Ricci C, et al. Effect of proton pump inhibitors and antacid therapy on 13C urea breath tests and stool test for Helicobacter pylori infection.Am J Gastroenterol. 2004; 99:8239. Shirin H, Levine A, Shevah O, et al. Eradication of Helicobacter pylori can be accurately confirmed 14 days after termination of triple therapy using a high-dose citric acid-based 13C urea breath test.Digestion. 2005; 71:208-12. el-Zimaity HM, al-Assi MT, Genta RM, Graham DY.Confirmation of successful therapy of Helicobacter pylori infection: number and site of biopsies or a rapid urease test.Am J Gastroenterol. 1995; 90:1962-4. Woo JS, el-Zimaity HM, Genta RM, Yousfi MM, Graham DY.The best gastric site for obtaining a positive rapid urease test.Helicobacter. 1996; 1:256-9. Dixon MF, Genta RM, Yardley JH, et al. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994.Am J Surg Pathol. 1996; 20:1161-81. Rugge M, Meggio A, Pennelli G, et al. Gastritis staging in clinical practice: the OLGA staging system.Gut. 2007; 56:631-6. Capelle LG, de Vries AC, Haringsma J, et al. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis.Gastrointest Endosc. 2010; 71:1150-8. Weston AP, Campbell DR, Hassanein RS, et al. Prospective, multivariate evaluation of CLOtest performance.Am J Gastroenterol. 1997; 92:1310-15. Marin AC, McNicholl AG, Gisbert JP.A review of rescue regimens after clarithromycin-containing triple therapy failure (for Helicobacter pylori eradication).Expert Opin Pharmacother. 2013; 14:843-61. Chen PY, Wu MS, Chen CY, et al. Systematic review with meta-analysis: the efficacy of levofloxacin triple therapy as the first- or second-line treatments of Helicobacter pylori infection.Aliment Pharmacol Ther. 2016; 44:427-37. Malfertheiner P.Infection: Bismuth improves PPI-based triple therapy for H. pylori eradication.Nat Rev Gastroenterol Hepatol. 2010; 7:538-9. Liao J, Zheng Q, Liang X, et al. Effect of fluoroquinolone resistance on 14-day levofloxacin triple and triple plus bismuth quadruple therapy.Helicobacter. 2013; 18:373-7. Liou JM, Chen CC, Chang CY, et al. Efficacy of genotypic resistance-guided sequential therapy in the third-line treatment of refractory Helicobacter pylori infection: a multicentre clinical trial.J Antimicrob Chemother. 2013; 68:450-6. Cosme A, Lizasoan J, Montes M, et al. Antimicrobial susceptibility-guided therapy versus empirical concomitant therapy for eradication of Helicobacter pylori in a region with high rate of clarithromycin resistance.Helicobacter. 2016; 21:29-34. Zeng M, Mao XH, Li JX, et al. Efficacy, safety, and immunogenicity of an oral recombinant Helicobacter pylori vaccine in children in China: a randomised, double-blind, placebo-controlled, phase 3 trial.Lancet. 2015; 386:1457-64.
REFERENCES
1. Tonkic A, Tonkic M, Lehours P, Mégraud F. Epidemiology and diagnosis of Helicobacter pylori infection. Helicobacter 2012; 17(Suppl 1):1-8. https://doi.org/10.1111/j.1523-5378.2012.00975.x
PMid:22958148
2. Ang TL, Fock KM, Ang D, et al. The changing profile of Helicobacter pylori antibiotic resistance in Singapore: a 15-year study. Helicobacter 2016; 21:261-5. https://doi.org/10.1111/hel.12291
PMid:26774006
4. Malfertheiner P, Megraud F, O'Morain CA, et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017; 66:6-30. https://doi.org/10.1136/gutjnl-2016-312288
PMid:27707777
5. Gisbert JP, Khorrami S, Carballo F, et al. Meta-analysis: Helicobacter pylori eradication therapy vs. antisecretory non-eradication therapy for the prevention of recurrent bleeding from peptic ulcer. Aliment Pharmacol Ther 2004; 19:617-29. https://doi.org/10.1111/j.1365-2036.2004.01898.x
PMid:15023164
6. Ford AC, Qume M, Moayyedi P, et al. Helicobacter pylori 'test and treat' or endoscopy for managing dyspepsia: an individual patient data meta-analysis. Gastroenterology 2005; 128:1838-44. https://doi.org/10.1053/j.gastro.2005.03.004
PMid:15940619
7. Arents NLA, Thijs JC, van Zwet AA, et al. Approach to treatment of dyspepsia in primary care: a randomized trial comparing 'test-and-treat' with prompt endoscopy. Arch Intern Med 2003; 163:1606-12. https://doi.org/10.1001/archinte.163.13.1606
PMid:12860586
8. Duggan AE, Elliott CA, Miller P, Hawkey CJ, Logan RF. Clinical trial: a randomized trial of early endoscopy, Helicobacter pylori testing and empirical therapy for the management of dyspepsia in primary care. Aliment Pharmacol Ther 2009; 29:55-68. https://doi.org/10.1111/j.1365-2036.2008.03852.x
PMid:18801056
9. Lassen AT, Pedersen FM, Bytzer P, Schaffalitzky de Muckadell OB. Helicobacter pylori test-and-eradicate versus prompt endoscopy for management of dyspeptic patients: a randomised trial. Lancet 2000; 356:455-60. https://doi.org/10.1016/S0140-6736(00)02553-8
10. McColl KE, Murray LS, Gillen D, et al. Randomised trial of endoscopy with testing for Helicobacter pylori compared with non-invasive H pylori testing alone in the management of dyspepsia. BMJ 2002; 324:999-1002. https://doi.org/10.1136/bmj.324.7344.999
PMid:11976239 PMCid:PMC102780
11. Gisbert JP, Calvet X. Helicobacter pylori 'test-and-treat' strategy for management of dyspepsia: a comprehensive review. Clin Transl Gastroenterol 2013; 4:e32. https://doi.org/10.1038/ctg.2013.3
PMid:23535826 PMCid:PMC3616453
12. Nocon M, Kuhlmann A, Leodolter A, et al. Efficacy and cost-effectiveness of the 13C-urea breath test as the primary diagnostic investigation for the detection of Helicobacter pylori infection compared to invasive and non-invasive diagnostic tests. GMS Health Technol Assess 2009; 5:Doc14.
PMid:21289901 PMCid:PMC3011289
13. Fock KM, Katelaris P, Sugano K, et al; Second Asia-Pacific conference. Second Asia-Pacific Consensus Guidelines for Helicobacter pylori infection. J Gastroenterol Hepatol 2009; 24:1587-600. https://doi.org/10.1111/j.1440-1746.2009.05982.x
PMid:19788600
14. Gisbert JP, de la Morena F, Abraira V. Accuracy of monoclonal stool antigen test for the diagnosis of H. pylori infection: a systematic review and meta-analysis. Am J Gastroenterol 2006; 101:1921-30. https://doi.org/10.1111/j.1572-0241.2006.00668.x
PMid:16780557
15. Kato S, Ozawa K, Okuda M, et al. Accuracy of the stool antigen test for the diagnosis of childhood Helicobacter pylori infection: a multicenter Japanese study. Am J Gastroenterol 2003; 98:296-300.
PMid:12591044
17. Burucoa C, Delchier JC, Courillon-Mallet A, et al. Comparative evaluation of 29 commercial Helicobacter pylori serological kits. Helicobacter 2013; 18:169-79. https://doi.org/10.1111/hel.12030
PMid:23316886
18. Duggan AE, Elliott C, Logan RF. Testing for Helicobacter pylori infection: validation and diagnostic yield of a near patient test in primary care. BMJ 1999; 319:1236-9. https://doi.org/10.1136/bmj.319.7219.1236
PMid:10550087 PMCid:PMC28273
20. Calvet X, García N, López T, et al. A meta-analysis of short versus long therapy with a proton pump inhibitor, clarithromycin and either metronidazole or amoxycillin for treating Helicobacter pylori infection. Aliment Pharmacol Ther 2000; 14:603-9. https://doi.org/10.1046/j.1365-2036.2000.00744.x
PMid:10792124
21. Labenz J. Current role of acid suppressants in Helicobacter pylori eradication therapy. Best Pract Res Clin Gastroenterol 2001; 15:413-31. https://doi.org/10.1053/bega.2001.0188
PMid:11403536
22. Villoria A, Garcia P, Calvet X, et al. Meta-analysis: high-dose proton pump inhibitors vs. standard dose in triple therapy for Helicobacter pylori eradication. Aliment Pharmacol Ther 2008; 28:868-77. https://doi.org/10.1016/s0016-5085(08)61572-3
23. Vallve M, Vergara M, Gisbert JP, Calvet X. Single vs. double dose of a proton pump inhibitor in triple therapy for Helicobacter pylori eradication: a metaanalysis. Aliment Pharmacol Ther 2002; 16:11490-56. https://doi.org/10.1046/j.1365-2036.2002.01270.x
24. Huang J, Hunt RH. The importance of clarithromycin dose in the management of Helicobacter pylori infection: a meta-analysis of triple therapies with a proton pump inhibitor, clarithromycin and amoxycillin or metronidazole. Aliment Pharmacol Ther 1999; 13:719-29. https://doi.org/10.1046/j.1365-2036.1999.00530.x
PMid:10383500
25. Fischbach L, Evans EL. Meta-analysis: the effect of antibiotic resistance status on the efficacy of triple and quadruple fi rst-line therapies for Helicobacter pylori. Aliment Pharmacol Ther 2007; 26:343-57. https://doi.org/10.1111/j.1365-2036.2007.03386.x
PMid:17635369
26. Ierardi E, Giorgio F, Losurdo G, Di Leo A, Principi M. How antibiotic resistances could change Helicobacter pylori treatment: a matter of geography? World J Gastroenterol 2013; 19:8168-80. https://doi.org/10.3748/wjg.v19.i45.8168
PMid:24363506 PMCid:PMC3857438
27. Graham DY, Lee YC, Wu MS. Rational Helicobacter pylori therapy: evidence-based medicine rather than medicine-based evidence. Clin Gastroenterol Hepatol 2014; 12:177-86. https://doi.org/10.1016/j.cgh.2013.05.028
PMid:23751282 PMCid:PMC3830667
28. Ghotaslou R, Leylabadlo HE, Asl YM. Prevalence of antibiotic resistance in Helicobacter pylori: a recent literature review. World J Methodol 2015; 5:164-74. https://doi.org/10.5662/wjm.v5.i3.164
PMid:26413490 PMCid:PMC4572030
29. Fallone CA, Chiba N, van Zanten SV, et al. The Toronto Consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology 2016; 151:51-69. https://doi.org/10.1053/j.gastro.2016.04.006
PMid:27102658
30. Ang TL, Fock KM, Song M, et al. Ten-day triple therapy versus sequential therapy versus concomitant therapy as first-line treatment for Helicobacter pylori infection. J Gastroenterol Hepatol 2015; 30:1134-9. https://doi.org/10.1111/jgh.12892
PMid:25639278
31. Dore MP, Lu H, Graham DY. Role of bismuth in improving Helicobacter pylori eradication with triple therapy. Gut 2016; 65:870-8. https://doi.org/10.1136/gutjnl-2015-311019
PMid:26848181
32. Gatta L, Vakil N, Ricci C, et al. Effect of proton pump inhibitors and antacid therapy on 13C urea breath tests and stool test for Helicobacter pylori infection. Am J Gastroenterol 2004; 99:8239. https://doi.org/10.1111/j.1572-0241.2004.30162.x
PMid:15128344
33. Shirin H, Levine A, Shevah O, et al. Eradication of Helicobacter pylori can be accurately confirmed 14 days after termination of triple therapy using a high-dose citric acid-based 13C urea breath test. Digestion 2005; 71:208-12. https://doi.org/10.1159/000087045
PMid:16024926
34. el-Zimaity HM, al-Assi MT, Genta RM, Graham DY. Confirmation of successful therapy of Helicobacter pylori infection: number and site of biopsies or a rapid urease test. Am J Gastroenterol 1995; 90:1962-4.
PMid:7485000
35. Woo JS, el-Zimaity HM, Genta RM, Yousfi MM, Graham DY. The best gastric site for obtaining a positive rapid urease test. Helicobacter 1996; 1:256-9. https://doi.org/10.1111/j.1523-5378.1996.tb00048.x
PMid:9398877
36. Dixon MF, Genta RM, Yardley JH, et al. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol 1996; 20:1161-81. https://doi.org/10.1097/00000478-199610000-00001
PMid:8827022
37. Rugge M, Meggio A, Pennelli G, et al. Gastritis staging in clinical practice: the OLGA staging system. Gut 2007; 56:631-6. https://doi.org/10.1136/gut.2006.106666
PMid:17142647 PMCid:PMC1942143
38. Capelle LG, de Vries AC, Haringsma J, et al. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis. Gastrointest Endosc 2010; 71:1150-8. https://doi.org/10.1016/j.gie.2009.12.029
PMid:20381801
39. Weston AP, Campbell DR, Hassanein RS, et al. Prospective, multivariate evaluation of CLOtest performance. Am J Gastroenterol 1997; 92:1310-15.
PMid:9260796
40. Marin AC, McNicholl AG, Gisbert JP. A review of rescue regimens after clarithromycin-containing triple therapy failure (for Helicobacter pylori eradication). Expert Opin Pharmacother 2013; 14:843-61. https://doi.org/10.1517/14656566.2013.782286
PMid:23537368
41. Chen PY, Wu MS, Chen CY, et al. Systematic review with meta-analysis: the efficacy of levofloxacin triple therapy as the first- or second-line treatments of Helicobacter pylori infection. Aliment Pharmacol Ther 2016; 44:427-37. 42. Malfertheiner P. Infection: Bismuth improves PPI-based triple therapy for H. pylori eradication. Nat Rev Gastroenterol Hepatol 2010; 7:538-9.
43. Liao J, Zheng Q, Liang X, et al. Effect of fluoroquinolone resistance on 14-day levofloxacin triple and triple plus bismuth quadruple therapy. Helicobacter 2013; 18:373-7. https://doi.org/10.1111/hel.12052
PMid:23581720 PMCid:PMC3974565
44. Liou JM, Chen CC, Chang CY, et al. Efficacy of genotypic resistance-guided sequential therapy in the third-line treatment of refractory Helicobacter pylori infection: a multicentre clinical trial. J Antimicrob Chemother 2013; 68:450-6. https://doi.org/10.1093/jac/dks407
PMid:23099849
45. Cosme A, Lizasoan J, Montes M, et al. Antimicrobial susceptibility-guided therapy versus empirical concomitant therapy for eradication of Helicobacter pylori in a region with high rate of clarithromycin resistance. Helicobacter 2016; 21:29-34. https://doi.org/10.1111/hel.12231
PMid:25982426
46. Zeng M, Mao XH, Li JX, et al. Efficacy, safety, and immunogenicity of an oral recombinant Helicobacter pylori vaccine in children in China: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2015; 386:1457-64. https://doi.org/10.1016/S0140-6736(15)60310-5