

Abstract
Chronic obstructive pulmonary disease (COPD) is a condition commonly encountered by primary care practitioners. The disease should be detected in its early stages to prevent disease progression and to reduce the burden of symptoms. Early treatment also results in improved mortality and reduced morbidity. COPD should be differentiated from other similar conditions such as asthma, as the basis of treatment differs in these conditions, and misdiagnosis can lead to poorer patient outcomes. Non-pharmacological treatment such as smoking cessation and vaccinations are important in the management of COPD, while pharmacotherapy such as bronchodilators and antimuscarinics are the mainstay of therapy in COPD. Referral to a specialist is recommended when there is progression of the disease or uncertainty regarding the diagnosis.
Mr Ng chose to transfer his chronic respiratory disease care to your clinic after learning that your clinic participates in the Community Health Assist Scheme (CHAS). You reviewed the transfer medical memo, which stated that Mr Ng was a smoker and required follow-up for the collection of his high-dose inhaled steroids and standby beta agonists (salbutamol) every 1–2 months. You also noted that there were no clear plans or diagnoses stated in the memo, but the visit history recorded for the past two years suggested an increase in episodes of breathlessness.
WHAT IS CHRONIC OBSTRUCTIVE PULMONARY DISEASE?
Chronic obstructive pulmonary disease (COPD) is characterised by airflow limitation that is usually progressive, and is associated with an enhanced chronic inflammatory response to noxious particles or gases in the airways and lungs. Exacerbations and comorbidities contribute to the overall severity of the condition in individual patients.(1)
HOW COMMON IS THIS IN MY PRACTICE?
COPD is the fourth leading cause of death in the world and a major cause of chronic morbidity. The disease is also among the top seven causes of hospitalisation and death in Singapore in 2011; the prevalence rates of moderate to severe COPD in Singapore is estimated at 3.5%.(2)
WHAT CAN I DO IN MY PRACTICE?
Making an early diagnosis
COPD is a preventable and treatable disease. Early diagnosis and appropriate treatment may improve symptoms, reduce the rate and severity of exacerbations, improve quality of life and exercise capacity, and prolong survival in patients.(3) Patients in early stages of COPD may have undetected activity limitations, such as walking slower than their peers or experiencing difficulties in performing activities that could easily be completed previously; such limitations may lead to lifestyle changes and deconditioning.(4) Hence, early diagnosis is critical in preventing worsening of COPD and reducing the burden of symptoms.
Clinical features of COPD
Clinical features of COPD include: (a) progressive dyspnoea, which typically worsens with exercise; (b) chronic cough, which may or may not be productive; and (c) risk factors such as passive or active smoking and family history of COPD. The more severe form of COPD is associated with weight loss, anorexia, depression, coronary heart disease, lung cancer and cognitive dysfunction. Physical examination typically reveals a prolonged expiratory phase in mild cases of COPD and features of hyperinflation as the severity of airway obstruction increases. Spirometry usually shows obstruction (forced expiratory volume in 1 second/forced vital capacity [FEV1/FVC] < 0.7) and no bronchodilator response.
Misdiagnosis of COPD
It is challenging to diagnose COPD, especially with mimickers such as asthma; a study has shown that primary care physicians have difficulties in correctly classifying up to 19.8% of patients.(5) Differentiating between asthma and COPD is important, as the treatment algorithms, choices and objectives differ in each condition.(6) In persistent asthma, inhaled steroids are the basis of treatment, while in COPD, bronchodilators are the mainstay of treatment, with inhaled steroids only recommended in patients with severe COPD.(1,7,8) However, steroid therapy may come with adverse effects; for instance, a study has shown that there is a higher risk of pneumonia in patients with COPD treated via inhaled steroids.(9) Misdiagnosis of COPD as pulmonary tuberculosis will similarly lead to a lack of appropriate treatment, resulting in a progression of the disease in the individual and further spread in the community. As such, correct diagnosis is pertinent, as misdiagnosis will lead to inappropriate treatment and suboptimal patient outcomes.(10)
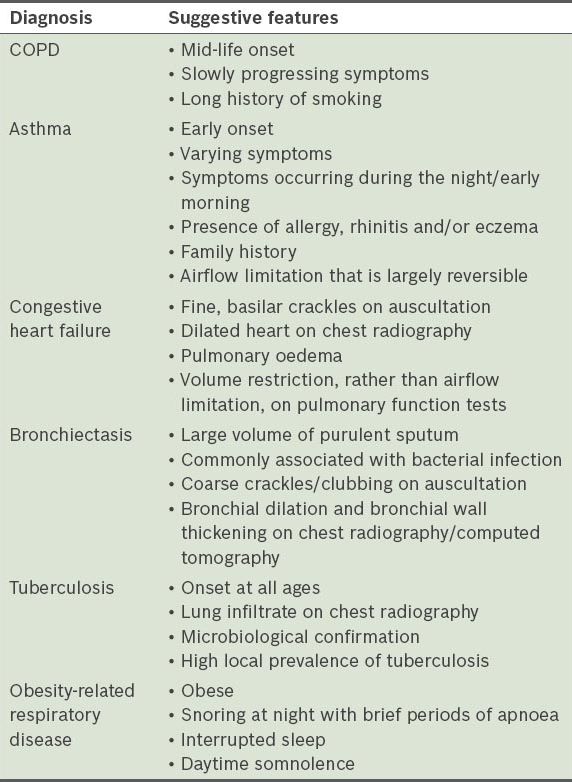
COPD vs. differential diagnosis
Differential diagnoses for COPD include asthma, obesity-related respiratory disease, ischaemic heart disease, congestive heart failure, bronchiectasis and tuberculosis.
Table I
Differential diagnoses for chronic obstructive pulmonary disease (COPD) and their respective suggestive features.(3)
Management of mild COPD
Non-pharmacological therapies are important in controlling patient symptoms. Smoking cessation involves the use of pharmacotherapy such as nicotine replacement. Brief smoking cessation counselling sessions (3 minutes) have been shown to be effective, with cessation rates of 5%–10% reported.(1,11) The “5As” – Ask, Advise, Assess, Assist and Arrange – can be employed to help patients who are willing to quit. Counselling by physicians is also found to significantly increase quit rates as compared to self-initiated strategies.(1,12) The Singapore Health Promotion Board QuitLine offers advice and useful information on how to quit smoking.
Annual influenza vaccination has been reported to significantly reduce COPD exacerbations.(1,13) Nichol et al found that pneumococcal vaccination for elderly patients with chronic lung disease reduces mortality and hospitalisations for pneumonia, and has direct medical care cost savings.(14) Patients with COPD can also benefit from rehabilitation and physical activity maintenance, as they improve exercise capacity, minimise hospitalisation and mortality rates, and improve recovery after exacerbation and quality of life.(1,15) Pulmonary rehabilitation is currently organised in local hospitals. Preliminary evidence shows that yoga training may improve lung function and exercise capacity on a short-term basis.(16,17) However, further studies are needed to substantiate these positive effects of yoga in COPD patients.
Mild COPD can also be managed by pharmacotherapy. Bronchodilator therapy is central to symptom management in patients with COPD and should be maximised before inhaled steroids are considered. An aerochamber can be used in cases where patient inhaler technique is incompetent. Bronchodilators can be prescribed pro re nata or on regular basis to reduce symptoms. Examples of bronchodilators include beta2-adrenoceptor agonist (short- or long-acting beta2-adrenoceptor agonists [SABA or LABA]), antimuscarinic agent and methylxanthines. Combination therapy (SABA + antimuscarinic agent) produces more sustained effects with fewer side effects compared to increasing doses of single bronchodilators. Long-term treatment with inhaled corticosteroids (ICS) is only recommended in patients with severe COPD and frequent exacerbations that cannot be controlled using LABA. Combination therapy (LABA + ICS) is more effective than the respective individual drugs. Oral mucolytic agents may reduce the risk of COPD exacerbation in patients receiving little or no treatment.(18)
It is important to monitor the disease progression and development of complications such as pneumonia, pneumothorax, bronchiectasis and right heart failure, as well as screen for and manage any comorbidities associated with COPD, such as common cardiovascular and metabolic diseases, anxiety/depression and osteoporosis. The attending physician should be alert and have a high index of suspicion for the development of lung cancer in the natural progression of COPD. Short courses of antibiotics in the treatment of moderate, infective exacerbation of COPD may be considered when there is heightened breathlessness with increased sputum volume and purulence.
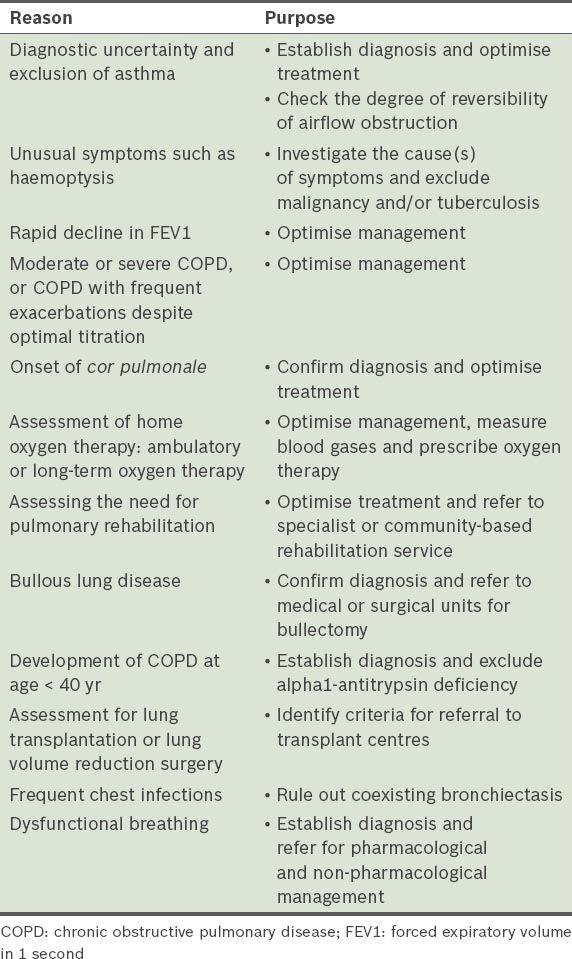
COMMON PITFALLS IN DIAGNOSING COPD
Referral to a specialist is recommended when there is progression of the disease or uncertainty regarding the diagnosis.
TAKE HOME MESSAGES
-
COPD is a common clinical condition and a major cause of morbidity.
-
COPD should be detected in its early stages, as early diagnosis and treatment can reduce disease progression and the burden of symptoms.
-
It is important to make a correct diagnosis, as misdiagnosis causes a delay in treatment and suboptimal patient outcomes.
-
Attending physicians should be aware of the importance of non-pharmacological therapies when managing patients with COPD.
-
Inhaled corticosteroid is not the mainstay of treatment for COPD.
You took a thorough clinical history for Mr Ng and noted that he had no family or personal history of atopy. The patient, however, remembered an episode of hospital admission for wheezing when he was very young. You referred him for spirometry, which excluded reversibility of airflow obstruction. At the six-month follow-up, you confirmed his diagnosis of COPD. You gave the patient pneumococcal and influenza vaccinations, stopped his inhaled steroid treatment and started him on regular community yoga classes. The patient subsequently felt more energetic with less dependence on inhalers, and you planned to continue working on his smoking cessation.