

INTRODUCTION
The COVID-19 pandemic originated in Wuhan, China, in December 2019.(1) It has since developed into a global pandemic, with a total of 2,475,723 cases reported globally and 169,151 confirmed deaths as of 23 April 2020.(2) The effects of this global pandemic are far-reaching, and the challenges faced by orthopaedic surgery globally amid this pandemic have been well described.(3-6) One of the most important considerations during the pandemic has been to reduce transmission risk to both the patient and the surgeon. As such, surgical organisations such as the American Academy of Orthopaedic Surgeons and American College of Surgeons have recommended that elective orthopaedic surgeries be postponed.(4,7) In addition, there has been a significant drain on surgical and protective equipment as well as personnel, with some orthopaedic surgeons redeployed to screening centres.(8)
Singapore identified its first case of COVID-19 on 23 January 2020.(9) The government response to this now global pandemic has been guided by the Disease Outbreak Response System Condition (DORSCON).(10) First formulated after the experience with severe acute respiratory syndrome (SARS), the DORSCON system is used to describe features of the disease outbreak and provide corresponding guidelines on the level of measures that may be required. On 7 February 2020, in view of rising COVID-19 cases, DORSCON Orange was implemented in Singapore to reflect a growing severity.(11) In line with this, our institution’s orthopaedic surgeons were advised to reduce any new listings for elective orthopaedic surgery during this time. On 7 April, to further contain COVID-19, a nationwide embargo on elective surgery for stable sports conditions and joint replacement surgeries was implemented.
There is some existing literature on the knowledge and attitudes of physicians regarding COVID-19.(6,12-14) Likewise, there have also been large-scale cross-sectional studies assessing levels of knowledge and perceptions of the public toward COVID-19.(15-17) Most of these studies have found a generally high understanding of COVID-19 among both medical personnel and the general population. However, there is a paucity of information regarding the knowledge and attitudes of patients who have been scheduled for elective orthopaedic surgery during the COVID-19 pandemic. This is important information, considering that as the COVID-19 pandemic situation improves, there is likely to be a graduated return to performing elective orthopaedic surgeries. Understanding patients’ perceptions will provide better insight on how to manage expectations as well as plan logistics during the surgical backlog.
In Singapore, the DORSCON structure guided a graduated response regarding elective surgery. While some institutions chose to completely cease elective surgeries, in our institution, elective orthopaedic surgeries were permitted up to 3 April. This provided a unique perspective for patients who were undergoing elective surgeries and gave us an opportunity to investigate patients’ knowledge and attitudes towards elective orthopaedic surgery amid a global pandemic. To our knowledge, no study has explored patients’ knowledge and attitudes towards undergoing elective orthopaedic surgery during the COVID-19 pandemic.
This study aimed to assess the knowledge of COVID-19 and attitudes towards elective surgery in a cohort of orthopaedic patients who were planned for elective surgery. The secondary aim was to determine whether there are differences in demographics, knowledge of COVID-19, attitudes towards COVID-19 and health risk-taking attitudes between patients who opted to proceed with surgery and those who chose to cancel their surgery.
METHODS
This was a questionnaire-based cohort study. The study group consisted of consecutive orthopaedic patients (under the care of the three authors) who were planned for elective surgery from 7 February 2020 to 1 April 2020. All patients who were scheduled to undergo elective surgery (i.e. joint arthroplasty and sports surgery procedures) during the study period were included. Patients who were due for emergency or urgent surgery and those whose surgery was cancelled owing to medical reasons were excluded. Ethics approval from the institutional review board was obtained for the study.
An anonymous questionnaire was administered to the patients at a single tertiary institution; patients were informed that the questionnaire was anonymous and voluntary. The questionnaire was completed within the outpatient clinic setting for those who were attending their outpatient clinic appointment, and via telephone for patients who were not in attendance.
The aim of the questionnaire was to assess patient demographics, level of objective knowledge of COVID-19, subjective assessment of COVID-19 severity, subjective assessment of the severity of the patients’ own orthopaedic condition, as well as their health risk attitude. The questionnaire was designed by all the authors, and a consolidated list of questions was chosen by consensus. The questionnaire was tested on a sample pool of patients to determine the ease of understanding. Revisions were made before the final questionnaire was administered.
The patient demographics that were assessed included age, gender, race, occupation, highest level of education, total household income and whether the respondent or family member had ever worked in healthcare. Respondents were asked a series of questions designed to assess their attitudes towards the severity of COVID-19 and the adequacy of the government response, scored on a five-point scale (1 = agree to a large extent, 2 = agree, 3 = neutral, 4 = disagree, 5 = disagree to a large extent). Respondents were then asked questions to assess their level of knowledge of COVID-19. These questions determined whether the respondents were aware of the symptoms, population at risk and mortality rate of COVID-19. The next segment of questions assessed how respondents viewed the severity and/or urgency of their own condition. An open-ended question was also posed to respondents regarding their reasons for proceeding or cancelling their elective orthopaedic surgery. Finally, the patients completed the Health-Risk Attitude Scale (HRAS),(18) a validated scale that assesses an individual’s attitude towards risk, specifically when dealing with matters of health. We chose this instrument over others such as the Domain-Specific Risk-Taking (DOSPERT) scale because of its ease of administration (13 questions vs. 35 questions for DOSPERT) and the fact that the HRAS has been shown to be internally consistent (Cronbach alpha = 0.83) and reliable (test-retest intraclass correlation coefficient = 0.86), with good construct and convergent validity.(19) This instrument consists of 13 questions scored from 1 (agree) to 7 (disagree), with a total score ranging from 13 to 91. A higher score reflects a more risk-averse attitude.
Descriptive statistics were calculated for the demographics and background variables. Univariate comparisons of means were conducted using Student’s t-test. Chi-square test was used for comparison of proportions between the two groups. Differences were considered significant when p-values were below 0.05. All analyses were performed in Stata version 15.0 (Stata Corp, College Station, TX, USA).
RESULTS
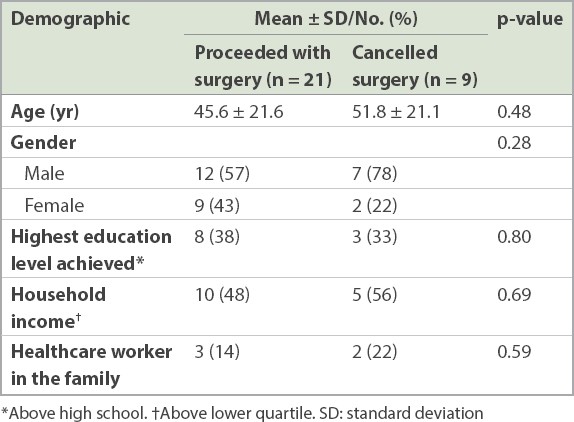
A total of 34 patients met the inclusion criteria. Of these, 30 (88%) completed the questionnaire. The median patient age was 51 (18–82) years, and 19 (63%) of the 30 patients were male. The total monthly household income of 15 (50%) patients was below the lower quartile, as per the national census.(20) 5 (17%) patients had a family member who was a healthcare worker. Of the 30 patients, 9 (30%) chose to cancel their surgery and 21 (70%) opted to proceed. No significant differences were observed in demographics such as age, gender, education level or household income between patients who chose to cancel their surgery and those who opted to proceed (
Table I
Demographic information of patients (n = 30)
In terms of perceptions of COVID-19, 24 (80%) patients thought that it was very easy or easy for a normal individual to get infected with COVID-19. 14 (47%) patients thought that transmission of COVID-19 within the hospital was very likely or likely, while 16 (53%) felt worried about contracting COVID-19. Although the majority (87%, n = 26) considered COVID-19 to be a national threat, most patients (87%, n = 26) felt that the government was handling the situation well.
In terms of knowledge of COVID-19 infection, all the patients were able to identify the at-risk groups (such as the elderly and those with underlying comorbidities) that are more susceptible to infection. 22 (73%) patients were able to correctly select the symptoms associated with COVID-19 infection. Patients with poorer knowledge tended to be less worried about contracting COVID-19 (p = 0.06). There was no significant effect of socioeconomic status or education level on the degree of knowledge of COVID-19. The presence of a healthcare worker in the family did not significantly improve the degree of knowledge of COVID-19, nor did it affect patients’ perception of the severity of COVID-19.
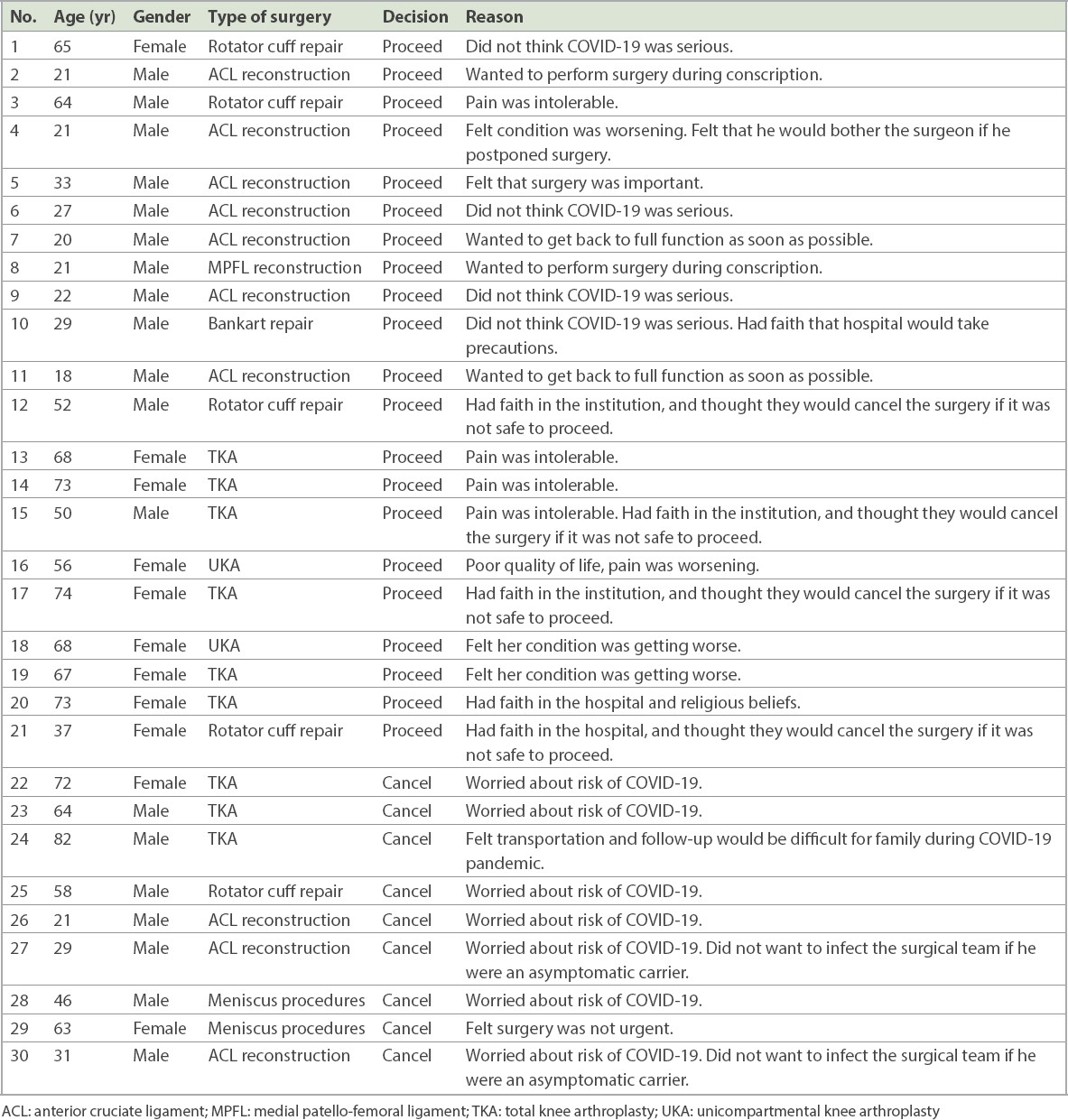
When assessing the severity of their own orthopaedic condition, 11 (37%) patients felt that surgery for their condition was urgent. Only 1 (3%) patient felt that surgery was risky, although 12 (40%) patients felt that their risk of surgery was elevated owing to the ongoing COVID-19 pandemic. Almost all (93%, n = 28) of the patients thought that the hospital would either postpone or cancel their surgery if there was an increased risk. When asked why they chose to proceed or cancel their surgery, some common themes surfaced. As expected, the majority (7/9, 78%) who cancelled their surgery cited the primary reason as “worried about the risk of COVID-19” (
Table II
Reasons for surgery decision in orthopaedic patients (n = 30).
DISCUSSION
COVID-19 is a global pandemic that has significantly affected healthcare systems. Its ripple effects on orthopaedic surgery are substantial. In particular, elective surgery has suffered over the last few months while healthcare systems were repositioning to better tackle the demands of the pandemic. The rationale for a complete embargo on elective surgery includes reducing unnecessary risks for both the patient and surgeon, as well as conservation of drugs and medical equipment.(5,8) However, there are also advantages to proceeding with previously listed electives. In addition to alleviating pain and disability in patients, it also reduces the likelihood of a mounting backlog of surgeries after the pandemic resolves. Any decision to proceed with elective surgery during a pandemic should be made relative to the disease curve and with consideration of hospital resources. In select healthcare systems that choose to proceed with elective surgery, it is important to understand the patients’ perceptions and knowledge of COVID-19, as it allows healthcare systems to better counsel patients and plan for their surgery. At the National Centre for Infectious Diseases, duties were split between staffing reserved for COVID-19 and maintaining some degree of ‘business as usual’. During the study period, our orthopaedic surgery department continued to clear previously listed electives and stopped all new listings. As of 3 April 2020, a complete embargo on elective surgeries was imposed.
Our study revealed that knowledge of COVID-19 was relatively high among our patients who were planned for elective orthopaedic surgery. This is consistent with other cross-sectional studies that have reflected a high level of COVID-19 knowledge among the public.(16,17) Interestingly, we found that traditionally vulnerable groups, such as the elderly(16) and socioeconomically disadvantaged individuals,(16,17) possessed a high level of COVID-19 knowledge. This is likely attributable to the considerable mainstream media coverage of this global pandemic, which also highlights the extensive efforts of the government in public education.
In terms of the patients’ view of COVID-19 as a personal threat, we found that the majority (80%) thought that it was very easy or easy for a normal individual to get infected. Despite this, only about half (47%) of the patients thought that transmission within the hospital would be very likely or likely. This perception affected whether a patient proceeded with surgery or not. Patients who proceeded with surgery were more likely to feel that the hospital was a safe environment, regardless of their concerns about COVID-19. This study also revealed that most patients (28/30, 93%) trusted that the hospital would cancel the surgery if there was an increased risk. This is consistent with the reasons given by patients who proceeded with surgery (i.e. “faith in the hospital system”). It is also important to note that patients who cancelled and those who proceeded with surgery had similar HRAS scores, as well as similar levels of concern about contracting COVID-19. Among patients who cancelled their surgery, the majority (7/9, 78%) cited the main reason as “worried about the risk of COVID-19”.
Altogether, these findings suggest that trust in the healthcare system is a key component of decision-making in patients. This information should guide patient counselling in a pandemic environment. Surgeons should be aware that despite concerns, patients who proceed with elective surgery often do so because they trust the hospital system and their surgeon. During a pandemic, the patient may have the expectation that the hospital would cancel the surgery if the risks are deemed to be high. As such, surgeons should be cognisant of this fact and proactively engage the patient in operative risk assessment about COVID-19 as part of preoperative counselling. Appropriate patient counselling regarding COVID-19 operative risk assessment is also likely to reduce the number of potential unnecessary surgical cancellations from patients. This is particularly critical to maximise surgical resources.
Patients who felt that their condition was worsening or severe were more likely to proceed with surgery. As healthcare systems ramp up towards ‘business as usual’, it is likely that most will face a backlog of surgeries. Perceived severity is a key concern for patients. This issue should be addressed in the event of delays in performing surgery. First, surgeons should consider appropriate patient education that is condition-centric. For example, in stable degenerative arthropathies, patients should be counselled that their surgery can be safely postponed because their condition is unlikely to worsen rapidly, and that similar surgical outcomes can be expected when the surgery is eventually performed. For patients who are in persistent pain, interim procedures such as nerve blocks or intra-articular injectables should be offered to reduce symptomology while awaiting surgery.
It is likely that the COVID-19 pandemic will have continued implications for elective surgery. This study has highlighted that while patients who are planned for elective surgery have high levels of knowledge about COVID-19, it is still prudent to offer counselling, specifically on any additional risks that COVID-19 may confer. In addition, condition-centric patient education, coupled with interim procedures aimed at reducing pain, can address some key concerns of patients with stable degenerative orthopaedic conditions. As we recover from the pandemic, it is important to continuously engage patients. If a patient’s key concerns are not well addressed, it is unlikely that the patient will accept continuous delays in elective surgery. Such actions will ultimately erode trust in the patient-doctor relationship.
Our study is not without limitations. First, we accept that the sample size in our study was small and no power analysis was performed owing to the absence of comparable published data. Second, this study was conducted in February and March 2020, when there were relatively low numbers of daily COVID-19 cases and fewer hospitalised COVID-19 patients in Singapore. These factors could have influenced our patients’ responses. Finally, we concede that our findings may not be generalisable to other populations. Thus, we recommend that further studies be undertaken to better define patients’ perceptions of elective surgery amid a global pandemic.
In conclusion, a high level of knowledge regarding COVID-19 was observed in our cohort of patients undergoing orthopaedic elective surgery. Key reasons for proceeding with surgery amid a pandemic include trust in the hospital system and patients’ self-perceived severity of their condition. It is important to address patients’ concerns with appropriate patient education and interim procedures when planning for elective orthopaedic surgery during a pandemic.