Author Information >Copyright and License information >
1Department of General Psychiatry, Institute of Mental Health, Singapore 2School of Psychiatry, University of New South Wales, Sydney, Australia 3Black Dog Institute, Sydney, Australia 4Department of Psychological Medicine, Tan Tock Seng Hospital, Singapore 5Department of Psychological Medicine, National University Hospital, Singapore 6Department of Psychological Medicine, Singapore General Hospital, Singapore 7Department of Psychological Medicine, Changi General Hospital, Singapore 8Department of Psychiatry, St George Hospital, Sydney, Australia Correspondence: Dr Verònica Gálvez, Visiting Fellow, School of Psychiatry, University of New South Wales, Hospital Road, 2031, Randwick, Sydney, New South Wales, Australia. vgalvezortiz@gmail.com
The use of electroconvulsive therapy (ECT) in Singapore dates back to 1947. However, there is little local information on the clinical practice of ECT and its standards. We aimed to conduct a comprehensive national survey of ECT practice in Singapore.
METHODS
A cross-sectional structured questionnaire assessing the types of ECT (e.g. electrode placement, stimulus parameters), indications, anaesthetic technique, dosing methods, monitoring of outcomes and credentialing was sent in 2015 to all ECT centres in Singapore via email to collect qualitative and quantitative data regarding ECT.
RESULTS
Data was obtained from all ECT centres (n = 6), which represented that ECT was available in 23.1% of all hospitals and 50.0% of all psychiatric specialist centres. The rate of ECT was 5.89 treatments per 10,000 residents per year, and each patient received an average of 5.4 ECT per course. Only 7.0% of ECT was administered for continuation/maintenance ECT. The most common indication for ECT was depression in 5 (83.3%) out of six centres, with schizophrenia being the second most common. In 5 (83.3%) out of six centres, ECT was brief (0.5 ms) bitemporal ECT with age-based dosing, and 93.0% of the sessions were conducted in an inpatient setting. All ECT was conducted under general anaesthesia, with propofol (66.7%) being the most common type of anaesthetic used.
CONCLUSION
The practice of ECT in Singapore was highly uniform. The rates and indications for ECT were consistent with those of other developed countries, with greater use of ECT for schizophrenia. Future advances for ECT in Singapore include the use of individualised dosing based on empirical seizure threshold titration, expanded electrode placements and increased utilisation of continuation/maintenance ECT.
Electroconvulsive therapy (ECT) is a safe and effective treatment for mood disorders(1,2) and schizophrenia.(3) The mechanism of ECT is not completely understood but is likely to involve changes in cerebral noradrenaline, serotonin and dopamine activities, permeability of the blood-brain barrier and neurogenesis.(4) Common side effects include headache, myalgia and transient cognitive impairment,(5) with an estimated mortality rate of 2.4 per 100,000 treatments.(6) Many surveys have been conducted in several countries and regions worldwide, reflecting that ECT practice is highly heterogeneous.(7) For instance, in Europe and Australia,(8-11) ECT is primarily used for the treatment of depression, while in Asia, it is also frequently used for psychotic disorders(12-15) and high suicide risk.(16) The United States and most Asian countries use bitemporal ECT,(7,17-20) while in Europe and Australia, the most prevalent electrode placement is right unilateral.(7,21) While this information is valuable, specific data on ECT parameters (e.g. pulse width), anaesthetic technique, methods of dosing, monitoring of ECT outcomes and credentialing is still lacking. For this reason, we developed a questionnaire exploring detailed information about ECT practice. This survey was conducted in Singapore to provide insights into current ECT practice and identify areas for future clinical improvement.
Singapore is a small nation state at the tip of the Malaysian archipelago. It has a population of approximately 5.5 million people consisting of 74.3% ethnic Chinese, 13.3% Malays and 9.1% Indians. The average per capita gross domestic product in 2015 was USD 53,947.93.(22) The lifetime prevalence of depression in Singapore is 5.8%, with a 12-month prevalence of 2.2%(23) and mean annual cost of treatment of USD 7,638.(24) Treatment of depression is estimated to give a 5.7-to-1 benefit-to-cost ratio.(25) While equivalent figures for schizophrenia are not available in Singapore, it is widely accepted that the economic burden of schizophrenia is significant, estimated between 0.02% and 1.65% of gross domestic product.(26)
ECT is a highly effective short-term treatment for depression and should be considered for patients who have not responded to standard antidepressant therapy.(27) There are currently 26 general hospitals and specialist centres, of which 12 offer specialist psychiatry services.(28) ECT was introduced in Singapore in 1947;(29) however, ECT practice has been little studied since then. Data on Singapore has been included in general Asian surveys on ECT practice,(18,30,31) and suggests that the usage of ECT for schizophrenia in Singapore decreased in 2000–2009 and that continuation ECT was performed by some centres in Singapore. Another survey published in 1992 examined the medicolegal implications of ECT practice in Singapore in a particular hospital.(32) However, despite seven decades of ECT practice, specific data at a national level on the matter remains insufficient to guide further development of ECT services and policy in Singapore.
METHODS
A structured, detailed questionnaire containing 54 questions (available upon request) was developed by two experienced ECT practitioners and researchers. The questionnaire was emailed to all ECT centres in Singapore, private and public, in 2015 and addressed to the head of department or head of ECT unit in these six public and private Singapore hospitals and specialist centres. Data was provided by one clinician per centre after conducting an audit of ECT data at five of six sites. Data collection lasted approximately six months. Hospitals were identified through inquiries to the Singapore Psychiatric Association and College of Psychiatrists, Academy of Medicine, Singapore. The following data was collected in the questionnaire: ECT governance, prescription, application (types of ECT – electrode placement and pulse width), anaesthesia technique, initial and subsequent ECT dosing methods, clinical monitoring, clinical indications, ECT rates, continuation/maintenance ECT, and credentialing and privileging in 2015.
Descriptive analysis of the data was performed using IBM SPSS Statistics version 21 (IBM Corp, Armonk, NY, USA).
RESULTS
Six centres were surveyed, with a response rate of 100.0%. This represented that ECT was available in 23.1% of the medical facilities in Singapore and 50.0% of psychiatric specialist facilities.(33) A total of 3,264 sessions of ECT were done for 602 patients in 2015. Among these, 3,034 (93.0%) sessions were inpatient acute sessions, while 230 (7.0%) sessions were outpatient maintenance ECT for 98 patients. This gave a treated person rate (TPR), defined as number of persons treated with ECT per 10,000 resident population per year, for ECT of 1.09 out of 10,000 resident population per year in a country of 5.54 million residents.(34) Each patient received an average of 5.4 sessions of ECT. There was a wide variation in the number of patients treated with ECT and number of ECT sessions conducted at each centre, with the largest centre performing 64.5% of all ECTs in Singapore. The other centres performed 17.9%, 6.9%, 5.1%, 4.2% and 2.5% of the ECT sessions. The largest centre had approximately 1,900 inpatient psychiatric beds, while the other centres had 10–24 inpatient psychiatric beds each. There were 14–413 patients per centre and 81–2,072 ECT sessions annually. Continuation or maintenance ECT was done at four centres with 1–93 patients and 9–204 sessions.
The two main indications for ECT were treatment-resistant depression (50.0% non-melancholic unipolar depression and 50.0% melancholic/psychotic unipolar depression) and treatment-resistant schizophrenia. 5 (83.3%) out of six centres reported depression as the main indication, with the remaining centre, which was also the largest ECT centre, reporting schizophrenia as the main indication. Other indications for ECT included mania, schizoaffective disorder, catatonia and neuroleptic malignant syndrome. Diagnosis was made by clinicians using either the Diagnostic and Statistical Manual of Mental Disorders (fourth edition text revision or fifth edition) or International Statistical Classification of Diseases and Related Health Problems (tenth revision) criteria. ECT was performed on adolescents aged ≥ 13 years in two centres, and all centres offered ECT to both adult and geriatric populations. All patients were on concomitant psychotropic medication at the time of ECT.
There were formal processes for the credentialing of doctors who could prescribe ECT for all but one centre, the most common credential being psychiatrist qualifications (83.3%). All centres had formal credentialing procedures for doctors who administered ECT, either requiring attendance at a formal ECT training course (66.7%) or qualification as a psychiatrist (50.0%). ECT was administered by a mixture of psychiatrists (50.0%), psychiatry trainees and psychiatry medical officers (50.0%). Medical officers were fully registered medical doctors without postgraduate psychiatric qualifications.
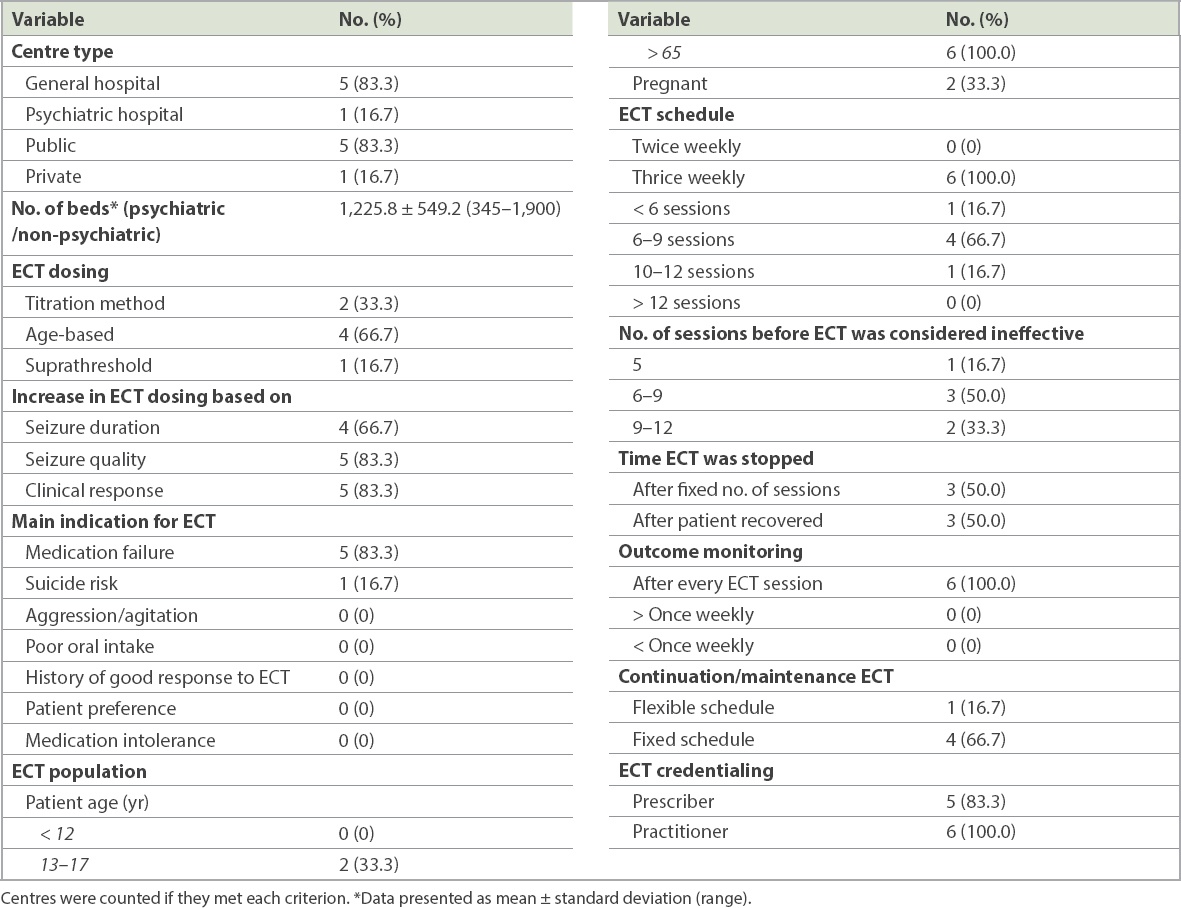
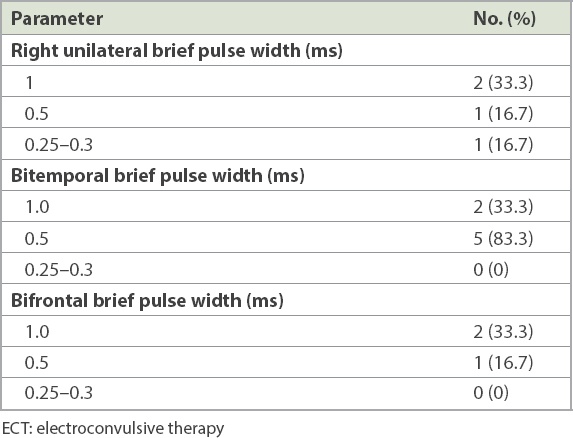
The most common type of initial ECT dosing (83.3%) was age-based dosing (half age, full age, age 10 or suprathreshold method), with only 2 (33.3%) sites using empirically derived seizure titration (Table I). The most common form of ECT prescribed was bitemporal ECT given with a brief pulse (83.3%, bitemporal 0.5 ms). Other forms were only used by a few hospitals (Table II). Subsequent ECT dosing was generally increased by 5%–10% machine energy if the electroencephalogram quality decreased or the patient was not responding to treatment, using a combination of patient response, seizure quality and seizure duration. This was determined based on the ECT practitioner’s individual experience and clinical assessment. ECT was generally prescribed as a fixed number of treatments, generally 6–12 sessions (88.3%) thrice weekly (100.0%).
Table I
Information on centres in Singapore practising electroconvulsive therapy (ECT) (n = 6).
Table II
ECT electrode placement and pulse width in Singapore centres (n = 6).
The primary anaesthetics used were propofol (66.7%, n = 4) and thiopentone (33.3%, n = 2), although ketamine, remifentanil and etomidate were also used by one centre. All centres used succinylcholine with anaesthesia. All anaesthesia was given by a consultant anaesthetist or an anaesthesia trainee under supervision by a consultant.
Pre-ECT assessments were fairly uniform across the centres, with full blood count, renal panel, electrocardiography and chest radiography being routinely ordered. All centres monitored patients’ blood pressure, pulse rate, electrocardiogram and electroencephalogram during the ECT procedure, with one centre doing carbon dioxide monitoring and electromyogram monitoring as well. Cognitive and efficacy rating scales were used in 83.3% (n = 5) and 66.7% (n = 4) of centres, respectively.
All ECTs were done using the Thymatron System IV. 50.0% of the ECTs were conducted in a dedicated ECT facility, with the rest being performed in a general operating theatre recovery room. All centres offered ECT on an inpatient basis although outpatient ECT was available at 50.0% (n = 3) of the centres. 66.7% (n = 4) of the centres offered maintenance ECT; involuntary ECT was also available in 66.7% (n = 4) of centres.
DISCUSSION
The present ECT survey provided cross-sectional detailed information on ECT practice in Singapore in 2015. The main strengths of this survey included complete responses from all ECT centres in Singapore and the eliciting of detailed information about the types of ECT provided, anaesthesia used, dosing strategies, ECT monitoring, credentialing and rates.
ECT was first performed in Singapore at the Institute of Mental Health (IMH).(29) Dr James Brown is credited with bringing ECT to Singapore in 1947 at IMH (then called Woodbridge Hospital).(29) In 1949, 5,220 ECT treatments were delivered at IMH to 420 patients, most of whom had schizophrenia. It was reported that 130 patients were discharged with a recovery rate of 30.9%.(29) The absolute number and TPR of ECT has fallen significantly since 1949, when the resident population was estimated at 940,824,(35) giving a TPR of 4.46, which is almost four times higher than that in 2015, which was 1.09.
The current TPR in Singapore is in the lower range of rates reported from other developed countries, such as the United States (range 2.39–5.1), Australia (range 1.6–4.4), Norway (range 2.4–4.3) and Belgium (range 4.3–4.7).(7) This decrease in Singapore’s ECT TPR parallels the worldwide decrease in ECT usage after the advent of chlorpromazine for schizophrenia, combined with the stigma associated with physical treatments in psychiatry (e.g. lobotomy), which carried connotations of coercion and infringement of human rights in the period between the 1960s and 1980s.(36) The past 50 years have seen significant advances in psychopharmacology that offered alternatives to ECT.(37) This global trend may have reached Singapore, as seen in how Singapore psychiatrists have similar attitudes to other psychiatrists in the world towards the usefulness of ECT for depression and schizophrenia. In the year 2000, only 40% of Singapore psychiatrists believed ECT was useful for schizophrenia and 59% felt it was useful for depression.(38)
ECT has been mostly practised as an inpatient procedure in Singapore despite evidence that it can be done safely and effectively as an outpatient procedure.(39,40) One consequence of this was the discarding of ECT by newer psychiatric departments that did not have inpatient wards, as it was largely regarded as an inpatient procedure. Personal conversations with clinicians in the newer specialist psychiatric centres also reveal the perceived lack of need for ECT as a treatment modality when psychiatric practice is outpatient focused. This initial perception is slowly evolving, with some of the newer psychiatric units establishing formal relationships with ECT centres to provide ECT to their outpatients. However, access to ECT is limited for increasing numbers of psychiatric patients due to the difficulties involved in transferring care to a facility with ECT capability as well as psychiatrists tending not to prescribe or consider treatment that is not available at their own centre. In Singapore, only the more established psychiatric departments have ECT facilities, and the three newest public psychiatric departments in Singapore did not have ECT capabilities at the time of this study.
For several decades, there was little variability in ECT practice (age-based bitemporal ECT). This changed in 2015, when seizure titration-based right unilateral treatment was introduced in two centres and empirically based seizure titration in one centre, suggesting that ECT practice had spread from IMH to the more established psychiatric departments from the 1980s and stayed constant in the ensuing decades. While age-based ECT is known to result in higher ECT doses(41,42) and have more cognitive side effects than ECT dosing based on empirically derived individual patient seizure thresholds,(43) it was traditionally considered an effective and acceptable form of ECT, especially for bilateral electrode placements(44,45) and easier to implement than seizure titration-based ECT methods.(44) In Singapore, a majority of ECT sessions have been performed using age-based strategies. This is probably a reflection of the perceived ease of use of age-based protocols and the absence of specialists trained in titration procedures. One possible consequence of this is the relatively low level of continuation/maintenance ECTs, with only 7% of ECTs conducted for continuation/maintenance ECT in our study. Continuation/maintenance ECT is uncommon in Asia,(7) despite good evidence of its efficacy for patients(46) who fail maintenance pharmacotherapy.
Approximately 63.5% of the ECT sessions in Singapore were conducted in one centre (with 1,900 beds), the largest psychiatric hospital in the country, while the next busiest centre provided 17.9% of ECT sessions despite having only 12 beds. The largest ECT centre was a tertiary psychiatric institute that served as a referral site for the most severe cases of psychiatric disorders, and the second-largest site was the only private inpatient psychiatric ward that serves about a third of the psychiatrists in Singapore in private practice. The tertiary referral nature of the private psychiatric ward may account for the relatively high rates of ECT in that centre. This observation is consistent with recent evidence that in developed countries, ECT is preferentially available in private settings for non-minority patients with insurance coverage.(47) Approximately half of the ECT sessions at the largest centre were for schizophrenia, while the other centres primarily used ECT for the treatment of depression. This may reflect the development of mental health services in Singapore: the National Mental Health Blueprint(48) focused care for psychotic disorders in the largest psychiatric centre in Singapore with the aim of using limited resources effectively and improving care for psychotic disorders, leading to a higher percentage of patients with schizophrenia in this centre. This would suggest that almost one-third of ECT sessions in Singapore was performed for the treatment of schizophrenia, a figure that is much higher than in other developed countries(7) but in line with other Asian countries.(18) One reason for this is the potential effectiveness of ECT for treatment-resistant schizophrenia(3,49) and the lack of onerous legal barriers for patients with schizophrenia accessing ECT care(32) faced by other developed countries.(50) There is no specific legislation distinguishing ECT from other psychiatric treatment, and its involuntary application is governed by the Mental Health (Care and Treatment) Act,(51) which states, inter alia: “A designated medical practitioner at a psychiatric institution who has examined any person who is suffering from a mental disorder and is of the opinion that he should be treated, or continue to be treated, as an inpatient at the psychiatric institution may at any time sign an order for the admission of the patient into the psychiatric institution for treatment; or in the case of an inpatient, for detention and further treatment of the person.”
Outside of the psychiatric institution, ECT can be prescribed in the patient’s best interest by the treating psychiatrist and with the relative’s consent, if the patient is assessed to lack capacity regarding ECT treatment. The principles of patient’s best interest are described in the Singapore Mental Capacity Act.(52) They are, essentially, that a patient is assumed to have capacity unless it is established otherwise, and that the patient’s past and present wishes, feelings, beliefs and values are taken into account when considering what is in the patient’s best interest. ECT that is provided under conditions where patients lack capacity has been shown to be effective.(53)
We found that the method of ECT prescription was fairly consistent, with half of the centres prescribing a fixed number of ECT sessions (range 6–9) and only 7.0% of all ECTs being done as maintenance ECT despite growing evidence that maintenance ECT is useful for preventing relapse.(54-56) There is high variability in the average number of ECT sessions prescribed around the world, ranging from 22 in Sweden(57) to one in Africa.(58) In Asia, the average number of ECT sessions prescribed is 6–8 treatments.(7) This high variability is unlikely to result from differences in illness profiles or patient characteristics between different geographical areas and may instead be related to differences in resources or practice. Such variability may reflect both over- and under-treatment of patients, unless patient response is taken into account. Treatment guidelines such as the American Psychiatric Association Task Force’s report on ECT(59) recommend prescribing ECT treatments based on clinical response within a range of ECT sessions rather than a fixed number of ECT sessions. Similarly, different treatment guidelines(60,61) have different approaches towards pre-ECT investigations, such as chest radiography, which is uniformly performed prior to ECT for patients aged above 40 years in Singapore. The use of anaesthesia was restricted to propofol or thiopentone in our study, which is consistent with the practice in most of Europe and Australia.(31)
Depression is a significant predictor for elderly suicide in Singapore.(62) Thus, it is salutary that all ECT centres in Singapore offered ECT to patients above 65 years of age, as ECT is a highly effective treatment for geriatric depression(63) despite the higher incidence of cardiovascular diseases in depressed geriatric patients, which may confer a higher anaesthetic risk during ECT. Such patients should have a full medical assessment to assess fitness for ECT.
Our study was not without limitations. Data was gathered via a survey completed by the lead clinician at each site; hence, data at the individual patient level was unavailable and demographic details of the patient population were not included in our analysis. Opinions of the authors regarding ECT in Singapore are also not reflective of the official positions of professional psychiatric bodies in Singapore.
In Singapore, future challenges for ECT include maintaining patients’ access to ECT given that newer psychiatric departments lack ECT services, increasing the use of continuation/maintenance ECT, using consistent formal rating scales to document the effectiveness and cognitive side effects of ECT, and expanding the types of ECT available to patients beyond age-based bitemporal ECT to the use of empirically derived seizure titration methods to optimise the efficacy and side-effect profile of ECTs. A Section of Neurostimulation under the College of Psychiatrists, Academy of Medicine, Singapore, has been established and will help drive the development of ECT via specialist training, standardised data collection and research in ECT. Quality of life is lower for patients with depression in Singapore and has been shown to improve after ECT in other countries.(64) Further research on ECT is recommended, especially regarding its effect on patients’ quality of life and its local cost-effectiveness.
ACKNOWLEDGEMENTS
Dr Chan received an honorarium from Lundbeck. Dr Loo received an honorarium from MECTA for teaching an international ECT course.
References UK ECT, Review GroupEfficacy and safety of electroconvulsive therapy in depressive disorders:a systematic review and meta-analysis.Lancet. 2003;361:799-808. Mukherjee S, Sackeim HA, Schnur DB.Electroconvulsive therapy of acute manic episodes:a review of 50 years'experience.Am J Psychiatry. 1994;151:169-76. Tharyan P, Adams CE.Electroconvulsive therapy for schizophrenia.Cochrane Database Syst Rev. 2005;2:CD000076. Sienaert P.Mechanisms of ECT:reviewing the science and dismissing the myths.J ECT. 2014;30:85-6. Watts BV, Groft A, Bagian JP, Mills PD.An examination of mortality and other adverse events related to electroconvulsive therapy using a national adverse event report system.J ECT. 2011;27:105-8. Dennis NM, Dennis PA, Shafer A, Weiner RD, Husain MM.Electroconvulsive therapy and all-cause mortality in Texas 1998-2013.J ECT. 2017;33:22-5. Leiknes KA, Jarosh-von Schweder L, Høie B.Contemporary use and practice of electroconvulsive therapy worldwide.Brain Behav. 2012;2:283-344. Teh SP, Xiao AJ, Helmes E, Drake DG.Electroconvulsive therapy practice in Western Australia.J ECT. 2005;21:145-50. Gazdag G, Palinska D, Kloszewska I, Sobow T.Electroconvulsive therapy practice in Poland.J ECT. 2009;25:34-8. Schweder LJ, Lydersen S, Wahlund B, Bergsholm P, Linaker OM.Electroconvulsive therapy in Norway:rates of use, clinical characteristics, diagnoses, and attitude.J ECT. 2011;27:292-5. van Waarde JA, Verwey B, van den Broek WW, van der Mast RC.Electroconvulsive therapy in the Netherlands:a questionnaire survey on contemporary practice.J ECT. 2009;25:190-4. McCall WV.Electroconvulsive therapy in Asia.J ECT. 2010;26:1. Tang YL, Jiang W, Ren YP, et al. Electroconvulsive therapy in China:clinical practice and research on efficacy.J ECT. 2012;28:206-12. Chung KF, Ng YK, Yiu GC, Cheung HK.Electroconvulsive therapy in Hong Kong.Psychiatr Bull. 2003;27:102-4. Chanpattana W, Kramer BA.Electroconvulsive therapy practice in Thailand.J ECT. 2004;20:94-8. Wang ZM, Zhu H, Pan YL, et al. Electroconvulsive therapy and its association with demographic and clinical characteristics in Chinese psychiatric patients.J ECT. 2015;31:114-8. Chanpattana W.One hundred twenty years of mental health care in Thailand and the development of electroconvulsive therapy.J ECT. 2010;26:11-3. Chanpattana W, Kramer BA, Kunigiri G, et al. A survey of the practice of electroconvulsive therapy in Asia.J ECT. 2010;26:5-10. Chanpattana W, Kunigiri G, Kramer BA, Gangadhar B.Survey of the practice of electroconvulsive therapy in teaching hospitals in India.J ECT. 2005;21:100-4. Motohashi N, Awata S, Higuchi T.A questionnaire survey of ECT practice in university hospitals and national hospitals in Japan.J ECT. 2004;20:21-3. O'Dea JF, Mitchell PB, Hickie IB.Unilateral or bilateral electroconvulsive therapy for depression?A survey of practice and attitudes in Australia and New Zealand.Med J Aust. 1991;155:9-11. Department of Statistics, SingaporePer capita gross domestic product 2016. Available at: https://www.singstat.gov.sg/find-data/search-by-theme/economy/national-accounts/latest-data#1. Accessed October 3 2016. Chong SA, Abdin E, Vaingankar JA, et al. A population-based survey of mental disorders in Singapore.Ann Acad Med Singapore. 2012;41:49-66. Ho RC, Mak KK, Chua AN, Ho CS, Mak A.The effect of severity of depressive disorder on economic burden in a university hospital in Singapore.Expert Rev Pharmacoecon Outcomes Res. 2013;13:549-59. Chisholm D, Sweeny K, Sheehan P, et al. Scaling-up treatment of depression and anxiety:a global return on investment analysis.Lancet Psychiatry. 2016;3:415-24. Chong HY, Teoh SL, Wu DB, et al. Global economic burden of schizophrenia:a systematic review.Neuropsychiatr Dis Treat. 2016;12:357-73. Chua H, Chan L, Chee K, et al. Ministry of Health clinical practice guidelines:Depression. Available at: https://www.moh.gov.sg/hpp/doctors/guidelines/GuidelineDetails/cpgmed_depression. Accessed October 3 2016. Ministry of Health, SingaporeHospital Services. Available at: https://www.moh.gov.sg/content/moh_web/home/our_healthcare_system/Healthcare_Services/Hospitals.html. Accessed October 3 2016. Ng BY. Till the Break of Day:a History of Mental Health Services in Singapore 1841-1993. 2001;Singapore NUS Press. Xiang YT, Ungvari GS, Correll CU, et al. Use of electroconvulsive therapy for Asian patients with schizophrenia (2001-2009):trends and correlates.Psychiatry Clin Neurosci. 2015;69:489-96. Little JD.ECT in the Asia Pacific region:what do we know?.J ECT. 2003;19:93-7. Chee KT.Medico-legal implications of electro-convulsive therapy--a Singapore viewpoint.Singapore Med J. 1992;33:271-2. Ministry of Health SingaporeCompleted Healthcare Facilities. Available at: https://www.moh.gov.sg/news-highlights/details/completed-healthcare-facilities. Accessed October 3 2016. Department of Statistics Singapore. Population and Population Structure 2015. Available at: https://www.singstat.gov.sg/find-data/search-by-theme/population/population-and-population-structure/latest-data. Accessed October 3 2016. Del Tufo MV.Malaya, comprising the Federation of Malaya and the Colony of Singapore:A report on the 1947 census of population.Crown Agents for the Colonies. 1949;. Shorter E, Healy D.Shock Therapy: a History of Electroconvulsive Treatment in Mental Illness.Rutgers University Press. 2007;. Payne NA, Prudic J.Electroconvulsive therapy:part II:a biopsychosocial perspective.J Psychiatr Pract. 2009;15:369-90. Parker G, Chen H, Kua J, Loh J, Jorm AF.A comparative mental health literacy survey of psychiatrists and other mental health professionals in Singapore.Aust N Z J Psychiatry. 2000;34:627-36. Jaffe R, Dubin W, Shoyer B, et al. Outpatient electroconvulsive therapy:efficacy and safety.Convuls Ther. 1990;6:231-8. Reti IM, Walker M, Pulia K, et al. Safety considerations for outpatient electroconvulsive therapy.J Psychiatr Pract. 2012;18:130-6. Petrides G, Braga RJ, Fink M.CORE (Consortium for Research in ECT) GroupSeizure threshold in a large sample:implications for stimulus dosing strategies in bilateral ECT:a report from CORE.J ECT. 2009;25:232-7. Tiller JW, Ingram N.Seizure threshold determination for electroconvulsive therapy:stimulus dose titration versus age-based estimations.Aust N Z J Psychiatry. 2006;40:188-92. Prudic J.Strategies to minimize cognitive side effects with ECT:aspects of ECT technique.J ECT. 2008;24:46-51. Abrams R.Stimulus titration and ECT dosing.J ECT. 2002;18:3-9. discussion 14-5. Petrides G, Fink M.The “half-age” stimulation strategy for ECT dosing.J ECT. 1996;12:138-46. Martínez-Amorós E, Cardoner N, Soria V, et al. Long-term treatment strategies in major depression:a 2-year prospective naturalistic follow-up after successful electroconvulsive therapy.J ECT. 2012;28:92-7. Slade EP, Jahn DR, Regenold WT, Case BG.Association of electroconvulsive therapy with psychiatric readmissions in US hospitals.JAMA Psychiatry. 2017;74:798-804. Chong S.Mental health in Singapore:a quiet revolution?.Ann Acad Med Singapore. 2007;36:795-6. Tor PC, Ying J, Ho NF, et al. Effectiveness of electroconvulsive therapy and associated cognitive change in schizophrenia:a naturalistic, comparative study of treating schizophrenia with electroconvulsive therapy.J ECT. 2017;33:272-7. Roy-Byrne P, Gerner RH.Legal restrictions on the use of ECT in California:clinical impact on the incompetent patient.J Clin Psychiatry. 1981;42:300-3. Singapore Statutes OnlineMental Health (Care and Treatment) Act 2008. Available at: https://sso.agc.gov.sg/Acts-Supp/21-2008/Published/20081030?DocDate=20081030. Accessed October 3 2016. SingaporeMental Capacity Act. 2008;c 177A:11. Chiu NM, Lee Y, Lee WK.Electroconvulsive therapy without consent from patients:one-year follow-up study.Asia Pac Psychiatry. 2014;6:83-90. Andrade C, Kanji S.Continuation and maintenance ECT:a review of recent research.J ECT. 2002;18:149-58. Russell JC, Rasmussen KG, O'Connor MK, et al. Long-term maintenance ECT:a retrospective review of efficacy and cognitive outcome.J ECT. 2003;19:4-9. Navarro V, Gastó C, Torres X, et al. Continuation/maintenance treatment with nortriptyline versus combined nortriptyline and ECT in late-life psychotic depression:a two-year randomized study.Am J Geriatr Psychiatry. 2008;16:498-505. Socialstyrelsen[ECT-treatment, a pilot study 2010]. Available at: https://www.socialstyrelsen.se/en/. Accessed October 3 2016Swedish. Selis MA, Kauye F, Leentjens AF.The practice of electroconvulsive therapy in Malawi.J ECT. 2008;24:137-40. American Psychiatric Association The Practice of Electroconvulsive Therapy:Recommendations for Treatment, Training, and Privileginga Task Force Report of the American Psychiatric Association. 2008;Arlington, VA American Psychiatric Publishing. Mental Health and Drug and Alcohol Office, NSW Government, Australia Electroconvulsive TherapyECT Minimum Standard of Practice in NSW. Available at: http://www0.health.nsw.gov.au/policies/pd/2011/PD2011_003.html.. Accessed October 3 2016. National Institute for Clinical ExcellenceGuidance on the use of electroconvulsive therapy. Available at: https://www.nice.org.uk/guidance/ta59. Accessed October 3 2016. Ho RC, Ho EC, Tai BC, Ng WY, Chia BH.Elderly suicide with and without a history of suicidal behavior:implications for suicide prevention and management.Arch Suicide Res. 2014;18:363-75. Kellner CH, Husain MM, Knapp RG.CORE/PRIDE Work GroupRight unilateral ultrabrief pulse ECT in geriatric depression:phase 1 of the PRIDE study.Am J Psychiatry. 2016;173:1101-9. Gálvez V, Li A, Oxley C, et al. Health related quality of life after ECT for depression:a study exploring the role of different electrode-placements and pulse-widths.J Affect Disord. 2016;206:268-72.
REFERENCES:
1. UK ECT Review Group. Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis. Lancet 2003; 361:799-808. https://doi.org/10.1016/S0140-6736(03)12705-5
2. Mukherjee S, Sackeim HA, Schnur DB. Electroconvulsive therapy of acute manic episodes: a review of 50 years' experience. Am J Psychiatry 1994; 151:169-76. https://doi.org/10.1176/ajp.151.2.169
PMid:8296883
5. Watts BV, Groft A, Bagian JP, Mills PD. An examination of mortality and other adverse events related to electroconvulsive therapy using a national adverse event report system. J ECT 2011; 27:105-8. https://doi.org/10.1097/YCT.0b013e3181f6d17f
PMid:20966769
6. Dennis NM, Dennis PA, Shafer A, Weiner RD, Husain MM. Electroconvulsive therapy and all-cause mortality in Texas, 1998-2013. J ECT 2017; 33:22-5. https://doi.org/10.1097/YCT.0000000000000340
PMid:27428480
7. Leiknes KA, Jarosh-von Schweder L, Høie B. Contemporary use and practice of electroconvulsive therapy worldwide. Brain Behav 2012; 2:283-344. https://doi.org/10.1002/brb3.37
PMid:22741102 PMCid:PMC3381633
10. Schweder LJ, Lydersen S, Wahlund B, Bergsholm P, Linaker OM. Electroconvulsive therapy in Norway: rates of use, clinical characteristics, diagnoses, and attitude. J ECT 2011; 27:292-5. https://doi.org/10.1097/YCT.0b013e318208e24b
PMid:21983754
11. van Waarde JA, Verwey B, van den Broek WW, van der Mast RC. Electroconvulsive therapy in the Netherlands: a questionnaire survey on contemporary practice. J ECT 2009; 25:190-4. https://doi.org/10.1097/YCT.0b013e31819190b5
PMid:19190510
13. Tang YL, Jiang W, Ren YP, et al. Electroconvulsive therapy in China: clinical practice and research on efficacy. J ECT 2012; 28:206-12. https://doi.org/10.1097/YCT.0b013e31825957b1
PMid:22801297
14. Chung KF, Ng YK, Yiu GC, Cheung HK. Electroconvulsive therapy in Hong Kong. Psychiatr Bull 2003; 27:102-4. https://doi.org/10.1192/pb.27.3.102
16. Wang ZM, Zhu H, Pan YL, et al. Electroconvulsive therapy and its association with demographic and clinical characteristics in Chinese psychiatric patients. J ECT 2015; 31:114-8. https://doi.org/10.1097/YCT.0000000000000181
PMid:25203288
17. Chanpattana W. One hundred twenty years of mental health care in Thailand and the development of electroconvulsive therapy. J ECT 2010; 26:11-3. https://doi.org/10.1097/YCT.0b013e3181c185f9
PMid:19935095
18. Chanpattana W, Kramer BA, Kunigiri G, et al. A survey of the practice of electroconvulsive therapy in Asia. J ECT 2010; 26:5-10. https://doi.org/10.1097/YCT.0b013e3181a74368
PMid:19444137
19. Chanpattana W, Kunigiri G, Kramer BA, Gangadhar B. Survey of the practice of electroconvulsive therapy in teaching hospitals in India. J ECT 2005; 21:100-4. https://doi.org/10.1097/01.yct.0000166634.73555.e6
PMid:15905751
20. Motohashi N, Awata S, Higuchi T. A questionnaire survey of ECT practice in university hospitals and national hospitals in Japan. J ECT 2004; 20:21-3. https://doi.org/10.1097/00124509-200403000-00005
PMid:15087992
21. O'Dea JF, Mitchell PB, Hickie IB. Unilateral or bilateral electroconvulsive therapy for depression? A survey of practice and attitudes in Australia and New Zealand. Med J Aust 1991; 155:9-11. https://doi.org/10.5694/j.1326-5377.1991.tb116367.x
PMid:2067461
23. Chong SA, Abdin E, Vaingankar JA, et al. A population-based survey of mental disorders in Singapore. Ann Acad Med Singapore 2012; 41:49-66.
24. Ho RC, Mak KK, Chua AN, Ho CS, Mak A. The effect of severity of depressive disorder on economic burden in a university hospital in Singapore. Expert Rev Pharmacoecon Outcomes Res 2013; 13:549-59. https://doi.org/10.1586/14737167.2013.815409
PMid:23977979
25. Chisholm D, Sweeny K, Sheehan P, et al. Scaling-up treatment of depression and anxiety: a global return on investment analysis. Lancet Psychiatry 2016; 3:415-24. https://doi.org/10.1016/S2215-0366(16)30024-4
26. Chong HY, Teoh SL, Wu DB, et al. Global economic burden of schizophrenia: a systematic review. Neuropsychiatr Dis Treat 2016; 12:357-73. https://doi.org/10.2147/NDT.S96649
PMid:26937191 PMCid:PMC4762470
29. Ng BY. Till the Break of Day: a History of Mental Health Services in Singapore, 1841-1993. Singapore: NUS Press, 2001.
30. Xiang YT, Ungvari GS, Correll CU, et al. Use of electroconvulsive therapy for Asian patients with schizophrenia (2001-2009): trends and correlates. Psychiatry Clin Neurosci 2015; 69:489-96. https://doi.org/10.1111/pcn.12283
PMid:25708964
35. Del Tufo MV. Malaya, comprising the Federation of Malaya and the Colony of Singapore: A report on the 1947 census of population. Crown Agents for the Colonies, 1949.
36. Shorter E, Healy D. Shock Therapy: a History of Electroconvulsive Treatment in Mental Illness. Rutgers University Press, 2007.
37. Payne NA, Prudic J. Electroconvulsive therapy: part II: a biopsychosocial perspective. J Psychiatr Pract 2009; 15:369-90. https://doi.org/10.1097/01.pra.0000361278.73092.85
PMid:19820554 PMCid:PMC3069072
38. Parker G, Chen H, Kua J, Loh J, Jorm AF. A comparative mental health literacy survey of psychiatrists and other mental health professionals in Singapore. Aust N Z J Psychiatry 2000; 34:627-36. https://doi.org/10.1080/j.1440-1614.2000.00739.x
PMid:10954394
39. Jaffe R, Dubin W, Shoyer B, et al. Outpatient electroconvulsive therapy: efficacy and safety. Convuls Ther 1990; 6:231-8.
40. Reti IM, Walker M, Pulia K, et al. Safety considerations for outpatient electroconvulsive therapy. J Psychiatr Pract 2012; 18:130-6. https://doi.org/10.1097/01.pra.0000413280.95843.d3
PMid:22418405
41. Petrides G, Braga RJ, Fink M, et al; CORE (Consortium for Research in ECT) Group. Seizure threshold in a large sample: implications for stimulus dosing strategies in bilateral ECT: a report from CORE. J ECT 2009; 25:232-7. https://doi.org/10.1097/YCT.0b013e31819c76ff
PMid:19972637 PMCid:PMC2792571
42. Tiller JW, Ingram N. Seizure threshold determination for electroconvulsive therapy: stimulus dose titration versus age-based estimations. Aust N Z J Psychiatry 2006; 40:188-92. https://doi.org/10.1080/j.1440-1614.2006.01773.x
PMid:16476138
43. Prudic J. Strategies to minimize cognitive side effects with ECT: aspects of ECT technique. J ECT 2008; 24:46-51. https://doi.org/10.1097/YCT.0b013e31815ef238
PMid:18379335
45. Petrides G, Fink M. The "half-age" stimulation strategy for ECT dosing. J ECT 1996; 12:138-46.
46. Martínez-Amorós E, Cardoner N, Soria V, et al. Long-term treatment strategies in major depression: a 2-year prospective naturalistic follow-up after successful electroconvulsive therapy. J ECT 2012; 28:92-7. https://doi.org/10.1097/YCT.0b013e31823e2705
PMid:22531201
47. Slade EP, Jahn DR, Regenold WT, Case BG. Association of electroconvulsive therapy with psychiatric readmissions in US hospitals. JAMA Psychiatry 2017; 74:798-804. https://doi.org/10.1001/jamapsychiatry.2017.1378
PMid:28658489 PMCid:PMC5710550
48. Chong S. Mental health in Singapore: a quiet revolution? Ann Acad Med Singapore 2007; 36:795-6.
49. Tor PC, Ying J, Ho NF, et al. Effectiveness of electroconvulsive therapy and associated cognitive change in schizophrenia: a naturalistic, comparative study of treating schizophrenia with electroconvulsive therapy. J ECT 2017; 33:272-7. https://doi.org/10.1097/YCT.0000000000000422
PMid:28640170
50. Roy-Byrne P, Gerner RH. Legal restrictions on the use of ECT in California: clinical impact on the incompetent patient. J Clin Psychiatry 1981; 42:300-3.
52. Singapore. Mental Capacity Act 2008, c 177A, s 11.
53. Chiu NM, Lee Y, Lee WK. Electroconvulsive therapy without consent from patients: one-year follow-up study. Asia Pac Psychiatry 2014; 6:83-90. https://doi.org/10.1111/j.1758-5872.2012.00203.x
PMid:23857906
55. Russell JC, Rasmussen KG, O'Connor MK, et al. Long-term maintenance ECT: a retrospective review of efficacy and cognitive outcome. J ECT 2003; 19:4-9. https://doi.org/10.1097/00124509-200303000-00002
PMid:12621270
56. Navarro V, Gastó C, Torres X, et al. Continuation/maintenance treatment with nortriptyline versus combined nortriptyline and ECT in late-life psychotic depression: a two-year randomized study. Am J Geriatr Psychiatry 2008; 16:498-505. https://doi.org/10.1097/JGP.0b013e318170a6fa
PMid:18515694
57. Socialstyrelsen. [ECT-treatment, a pilot study 2010]. Available at: https://www.socialstyrelsen.se/en/. Accessed October 3, 2016. Swedish.
59. American Psychiatric Association. The Practice of Electroconvulsive Therapy: Recommendations for Treatment, Training, and Privileging: a Task Force Report of the American Psychiatric Association. Arlington, VA: American Psychiatric Publishing, 2008.
61. National Institute for Clinical Excellence. Guidance on the use of electroconvulsive therapy. Available at: https://www.nice.org.uk/guidance/ta59. Accessed October 3, 2016.
62. Ho RC, Ho EC, Tai BC, Ng WY, Chia BH. Elderly suicide with and without a history of suicidal behavior: implications for suicide prevention and management. Arch Suicide Res 2014; 18:363-75. https://doi.org/10.1080/13811118.2013.826153
PMid:24828390
63. Kellner CH, Husain MM, Knapp RG, et al; CORE/PRIDE Work Group. Right unilateral ultrabrief pulse ECT in geriatric depression: phase 1 of the PRIDE study. Am J Psychiatry 2016; 173:1101-9. https://doi.org/10.1176/appi.ajp.2016.15081101
PMid:27418379
64. Gálvez V, Li A, Oxley C, et al. Health related quality of life after ECT for depression: a study exploring the role of different electrode-placements and pulse-widths. J Affect Disord 2016; 206:268-72. https://doi.org/10.1016/j.jad.2016.08.002
PMid:27541282