Singapore Med J 2022; 63(5): 263-267 doi: 10.11622/smedj.2020165
Endovascular repair of mycotic aortic aneurysms confers good medium-term outcomes and aneurysmal sac resolution
Yi Ting Lim1, MBBS, Wee Ming Tay1, MBBS, FRCS, Zhiwen Joseph Lo1, MBBS, FRCSEd, Uei Pua2, MBBS, FRCR, Lawrence Han Hwee Quek2, BMBS, FRCR, Bien Ping Tan2, MBBS, FRCR, Sadhana Chandrasekar1, MBBS, FRCS, Glenn Wei Leong Tan1, MBChB, FRCSEd
Author Information >Copyright and License information >
1Vascular Surgery Service, Department of General Surgery, Tan Tock Seng Hospital, Singapore 2Vascular and Interventional Radiology, Department of Diagnostic Radiology, Tan Tock Seng Hospital, Singapore Correspondence: Dr Zhiwen Joseph Lo, Consultant, Vascular Surgery Service, Department of General Surgery, Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, Singapore 308433. zhiwen@gmail.com
Mycotic aortic aneurysm (MAA) is a life-threatening condition. Endovascular repair (EVAR) of aortic aneurysms has been found to be a safe and effective alternative to open repair. We aimed to present the short- to medium-term outcomes for EVAR of MAA in our cohort.
METHODS
We conducted a retrospective study of 23 consecutive patients with MAA who underwent EVAR in our hospital from January 2008 to July 2017.
RESULTS
The mean age of our study population was 62 years. The mean aneurysmal size was 3.2 cm. Abdominal MAAs (n = 16, 70%) were the most common, followed by thoracic MAAs (n = 4, 17%). There was no 30-day mortality in our cohort. Endoleak (Types 1, 3, 4) was detected in 3 (13%) cases. At the one-month surveillance computed tomography aortogram, all patients had a reduction in aneurysmal size and 5 (22%) had complete aneurysmal sac resolution. 7 (30%) patients had sac resolution at six months and 8 (35%) patients, at 12 months. The overall survival was 91%, 80% and 61% at one, 12 and 60 months, respectively.
CONCLUSION
EVAR is a feasible and durable method for the repair of MAA, with a five-year overall survival of 61%. All patients in our study had a reduction in aneurysmal size at one month, with 65% having complete aneurysmal sac resolution by 12 months.
Mycotic aortic aneurysm (MAA) is a life-threatening condition that represents 0.5%–2.6% of all aortic pathologies.(1) Patients who develop these aneurysms commonly have multiple risk factors for an immunocompromised state. In addition, they tend to present with concomitant sepsis, which puts them at high surgical risk.(2) Classically, the standard approach consists of aggressive intravenous (IV) antibiotic therapy with open surgical debridement of the aneurysm and surrounding infected tissue, as well as extra-anatomic or in situ bypass.(3,4) However, outcomes are poor, especially in the elderly, with mortality and morbidity rates of up to 43%.(5)
Endovascular repair (EVAR) of aortic aneurysms provides a safe and effective alternative to a largely invasive approach,(6,7) with multiple benefits, including reduction of massive blood loss, lower incidence of early mortality/morbidity and avoidance of aortic cross-clamping, which predisposes a patient to prolonged distal ischaemia.(8,9) This is especially so in high-risk surgical patients. However, EVAR has various limitations – the infected material and debris are left inside the patient, which increases the risk of the prosthesis being infected, as well as persistent or recurrent sepsis. Other challenges include rupture of the aorta above or below the graft owing to continued infection,(5) and other conventional EVAR risks such as endoleak, contrast-induced nephropathy and embolic or thrombotic events. In this study, we aimed to present the short- to medium-term outcomes for EVAR of MAA, especially in terms of sac resolution, as well as a review of the current available literature.
METHODS
We conducted a single-institution retrospective review of 23 patients who underwent EVAR of MAA in our hospital from January 2008 to July 2017. The diagnosis of MAA was based on a combination of the following criteria: (a) clinical presentation (fever, pain, sepsis); (b) biochemical results (leucocytosis, elevated inflammatory markers like C-reactive protein); and (c) radiological findings (large aneurysms that were ruptured/contained, periaortic gas).
A common study protocol was applied, with the collected data consisting of patient demographics, comorbidities, biochemistry upon presentation, aneurysm characteristics (size and morphology), duration of antibiotic therapy, operative data, postoperative complications and radiological surveillance results. Devices used to repair the aneurysms consisted of stent grafts from Medtronic (Minneapolis, MN, USA), Cook Medical (Bloomington, IN, USA) and Endologix (Irvine, CA, USA).
All patients received broad-spectrum empirical IV antibiotics 1–90 days preoperatively in consultation with the infectious diseases (ID) physician. Patients with positive blood cultures were switched to organism-specific antibiotics once the results were out, while the remaining patients continued with broad-spectrum antibiotics. 11 patients were considered stable and underwent early stenting after control of systemic sepsis with antibiotics, while the other 12 underwent emergency repairs. Postoperatively, the patients completed six weeks of targeted IV antibiotics followed by targeted lifelong suppressive antibiotics upon consultation with the ID physician. They also received regular reviews: clinical examination, biochemical testing and follow-up computed tomography (CT) at one, six and 12 months. All patients with negative blood cultures were prescribed Bactrim (trimethoprim and sulfamethoxazole).
Investigated factors were analysed using descriptive statistics. Percentages were used for categorical data and means with standard deviations for continuous data. Kaplan-Meier survival analysis was performed to ascertain the survival rates at pre-determined intervals. All data analysis was performed using IBM SPSS Statistics version 21.0 for Windows (IBM Corp, Armonk, NY, USA).
RESULTS
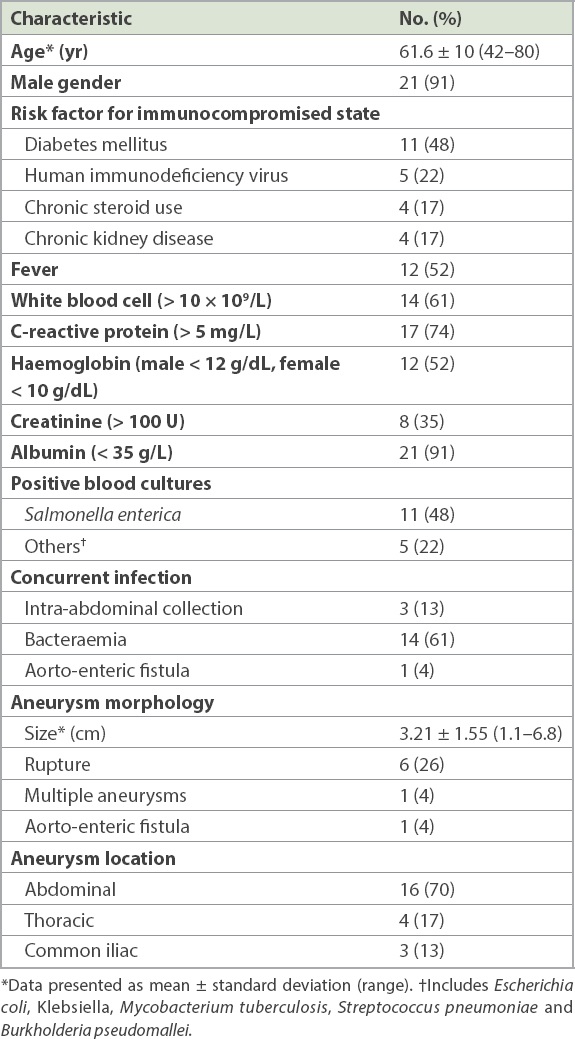
During the nine-year study period, 23 patients (21 male and 2 female) with MAA were identified (Table I). The mean age of the study population was 62 (range 42–80) years. The median clinical follow-up duration was 19 (range 2–143) months. 17 (74%) patients had at least one risk factor for an immunocompromised state, the most common being diabetes mellitus (48%), followed by human immunodeficiency virus (22%), chronic steroid use (17%) and chronic kidney disease (17%). 16 (70%) patients had positive blood cultures, with Salmonella enterica being the most common organism identified (n = 11, 48%).
Table I
Patient characteristics (n = 23).
Upon presentation, 12 (52.2%) patients had fever, 14 (60.9%) had leukocytosis (> 10 × 109/L), 12 (52.2%) had anaemia (male < 12 g/dL, female < 10 g/dL), 17 (73.9%) had elevated C-reactive protein (> 5 mg/L) and 21 (91.3%) had hypoalbuminaemia (< 35 g/L). The mean preoperative antibiotic duration at the time of operative repair was 15 (range 1–90) days. Postoperatively, all patients received lifelong antibiotics.
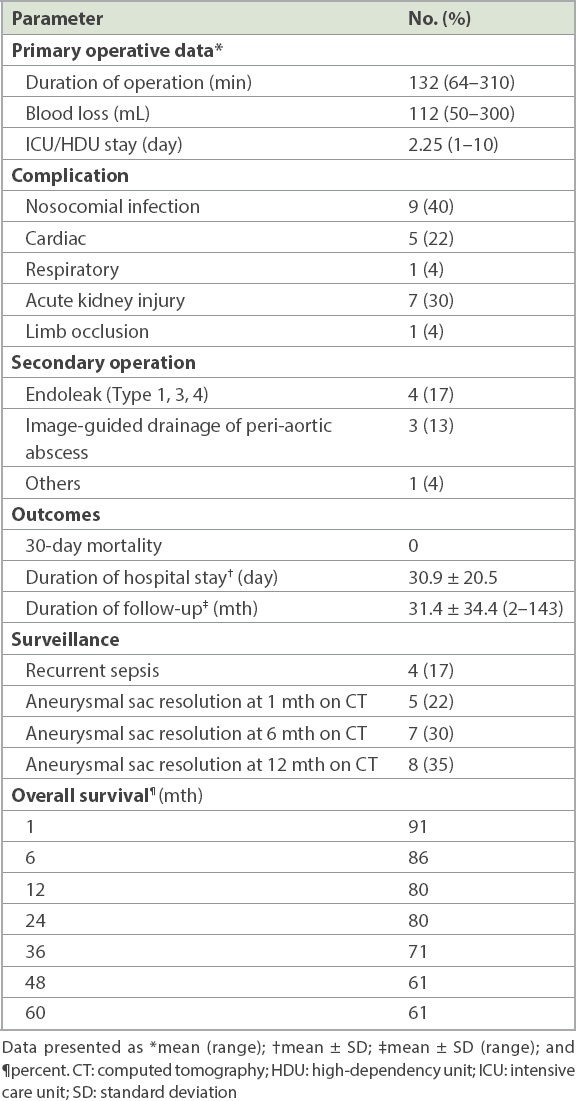
Abdominal MAAs (n = 16, 70%) were the most common, followed by thoracic MAAs (n = 4, 17%) and common iliac aneurysms (n = 3, 13%). 6 (26%) patients presented with a ruptured aneurysm and 1 (4%) patient had an aorto-enteric fistula. The mean aneurysmal size was 3.2 (range 1.1–6.8) cm. The mean operation time was 132 (range 64–310) minutes. The mean amount of blood loss was 112 (range 50–300) mL and the average duration of stay in the intensive care unit or high-dependency unit was 2.25 (range 1–10) days. There was no 30-day mortality, and the mean length of hospital stay was 31 (range 5–84) days (Table II). After repair, 9 (39.1%) patients contracted nosocomial infections, 8 (34.8%) required a second operation, 7 (30.4%) had acute kidney injury and 5 (21.7%) had cardiac complications. One patient had thrombosis of the left common iliac artery.
Table II
Operative data and outcomes (n = 23).
Endoleak (Types 1, 3, 4) was detected in 4 (17%) patients, for which they underwent stent re-lining after detection on surveillance imaging. 3 (13%) patients required image-guided drainage of peri-aortic abscesses and 1 (4%) patient required a laparotomy and excision of an aorto-oesophageal fistula with duodenal-jejunal anastomosis. 2 (9%) patients suffered from recurrent aneurysm-related sepsis, and there was one aneurysm-related mortality (secondary to aorto-oesophageal fistula). Other causes of mortality included pneumonia secondary to systemic lupus erythematosus, metastatic lung cancer, malignant pleural effusion secondary to oesophageal carcinoma, enterococcaemia secondary to psoas abscess and ischaemic heart disease. Of the other five cases of mortality, only one patient underwent an emergency repair.
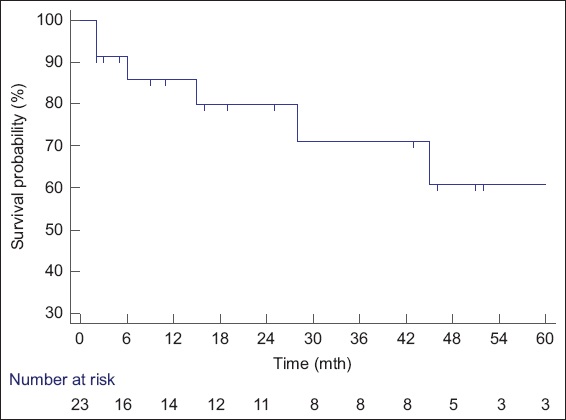
At one-month surveillance CT aortogram, all patients showed a reduction in the size of the aneurysm; of these, 5 (22%) patients had complete aneurysmal sac resolution, 7 (30%) had sac resolution at six months and 8 (35%) had sac resolution at 12 months. The overall survival was 91%, 86%, 80% and 61% at one, six, 12 and 60 months, respectively (Table II, Fig. 1). There was no difference in survival between those who underwent elective and emergency repair, as the causes of mortality in this series were largely unrelated to the aneurysm, with the exception of the one case of aorto-oesophageal fistula.
Fig. 1
Kaplan-Meier survival curve shows overall survival of 91%, 80% and 61% at 1, 12 and 60 months, respectively.
DISCUSSION
Despite advances in perioperative optimisation and antimicrobial regimes, an optimal treatment strategy for MAA has yet to be agreed upon. Although EVAR is now widely used and generally acceptable, the decision to rely solely on EVAR as the therapeutic gold standard is uncertain. Kim et al reported good short- and medium-term outcomes in their series with open repair of MAA despite their patients being at high risk for open surgery.(10) Hybrid therapy (combination of EVAR and open surgery) remains an option, especially for those with recurrent sepsis. However, for some physicians, placing a prosthetic material in an infected field is counter-intuitive, even controversial.
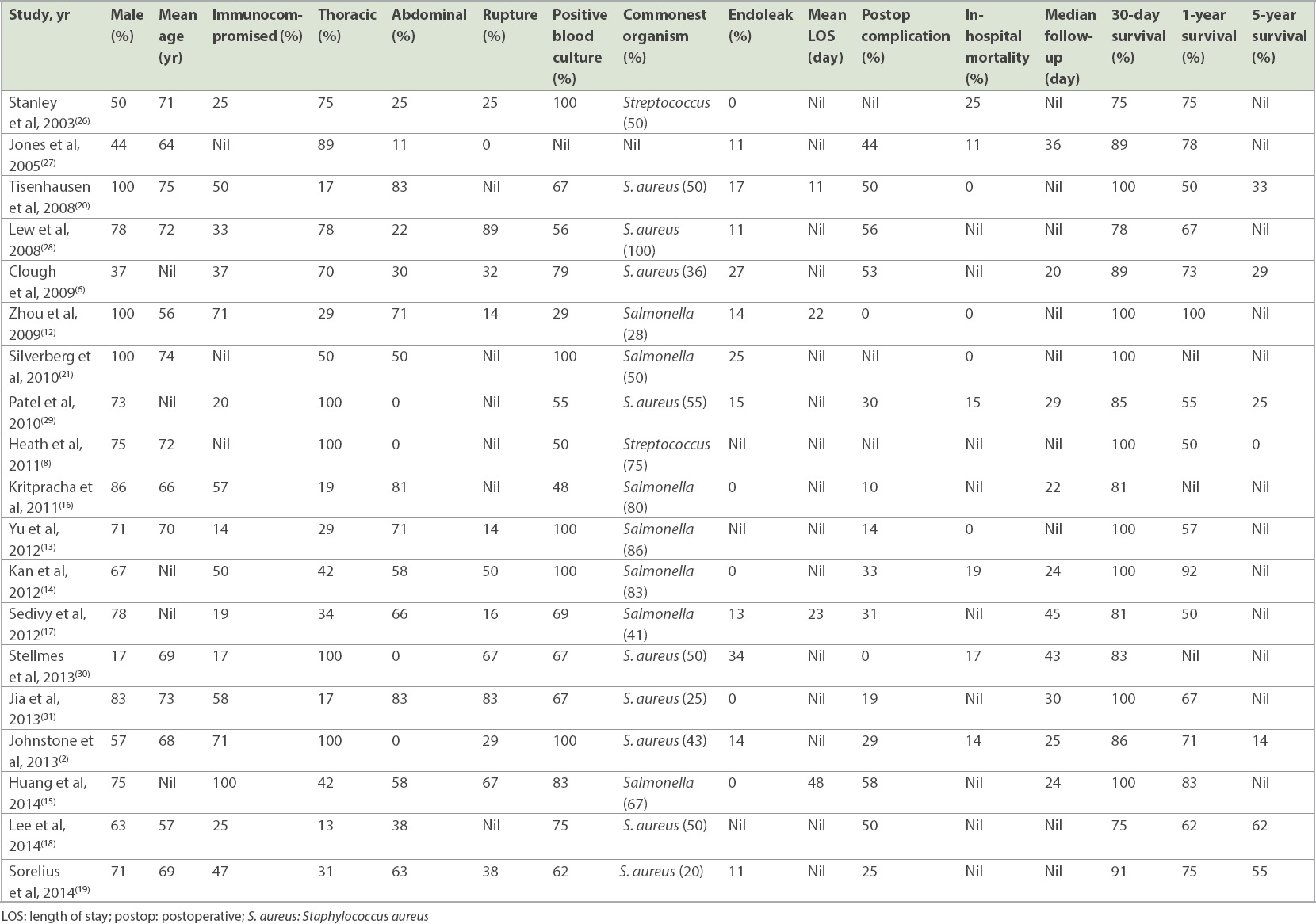
Studies have shown that Salmonella infections are more common in the Asian population compared to their Western counterparts.(11) A review of the existing literature (Table III) found that out of seven studies conducted in the East, six reported Salmonella as the most common organism identified in blood cultures.(12-17) This corresponds to our finding – 70% of our patients who had positive blood cultures were positive for Salmonella. Salmonella-related aneurysms are also known to have rapid disease progression and a risk of early rupture. This is because Salmonella tends to adhere to vascular endothelium, especially if it is diseased by atherosclerosis.(12)
Table III
Endovascular repair of mycotic aortic aneurysms in the literature.
Kritpracha et al reported that EVAR had a poor outcome in patients with fistula complication.(16) This is also noted in our study, as the only aneurysm-related death was secondary to an aorto-oesophageal fistula, likely because these patients tend to present with overwhelming sepsis and shock, and are unable to recover owing to their advanced age and comorbidities. Our centre had overall higher rates of nosocomial infections as well as cardiac and kidney complications compared to those reported in the current literature. This could be due to the advanced age of our patient population and their various comorbidities, which precluded them to a difficult postoperative recovery. Our centre’s endoleak rate of 17% is comparable to that of other studies (range 0%–34%).(2,12,17) Of note, the Type 3 and 4 endoleaks that occurred in this series were from the older-generation stent grafts, and such leaks are exceedingly rare with the advent of modern devices.
Our five-year survival rate of 61% was similar to that of other studies,(18,19) while our in-hospital mortality rate was also comparable to that reported in other studies,(12,13,20,21) with a mean rate of 10% (range 0%–25%). Compared with open surgery, which showed in-hospital mortality rates of 12%–27%,(3,9,11) our in-hospital mortality rate for EVAR was much lower, at 0%. Thus, EVAR as the first-line treatment in patients with MAA is a reasonable approach owing to its low in-hospital mortality rate. Notably, most of the identified studies did not report the five-year survival rates owing to the lack of follow-up.
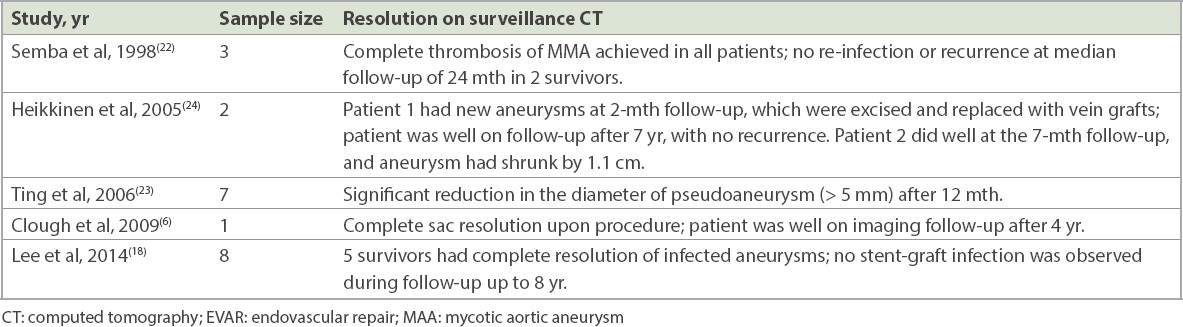
In our study, the reported sac resolution rates of 22%, 30% and 35% at one, six and 12 months, respectively, are one of the first few reported and should be a documented follow-up marker for future studies. We noted that five studies in the current literature had published their CT surveillance results (Table IV). Of these, three studies reported complete resolution of the aneurysmal sac in their surviving patient population(6,18,22) and two studies reported a significant reduction in aneurysmal size after seven and 12 months, respectively.(23,24) However, as these papers had only a small sample population of 1–8 patients, it is difficult to draw any statistically meaningful conclusions from them.
Table IV
Studies documenting MAA sac resolution after EVAR.
Compliance to antibiotic therapy is of utmost importance. As recurrent infection cannot be excluded, lifelong antibiotic therapy and radiological surveillance are mandatory. This is especially so in our patient population, most of whom were frail and immunosuppressed and hence, might not have been able to mount an early response to recurrent infection. However, there is no universal agreement on the mandatory use of lifelong antibiotic therapy; in some centres, antibiotic therapy may be discontinued if there is no clinical or radiological evidence of ongoing sepsis.(1,9,25)
The main limitation of the current study is its small sample size owing to the rarity of the disease, making it impossible to reach statistically meaningful conclusions. Other limitations include the retrospective nature of the study and the existence of patient selection bias. Furthermore, the median follow-up duration of 19 months is not long enough to identify all cases of late aneurysm-related mortality, especially in patients who underwent EVAR. Therefore, an extended, multi-institutional study that compares the outcomes of open repair and EVAR would be recommended.
In conclusion, EVAR was a feasible and durable method for repairing MAA in our patients who were on lifelong antibiotics. Although the aortic interventions performed were successful, immunocompromised patients had difficult postoperative recoveries. All our patients saw a reduction in aneurysmal size at one month, with 65% having complete aneurysmal sac resolution by 12 months. The recurrence rate for aneurysm-related sepsis was low at 9%, and the five-year overall survival rate was acceptable at 61%.
References Chan FY, Crawford ES, Coselli JS, Safi HJ, Williams TW, Jr last In situ prosthetic graft replacement for mycotic aneurysm of the aorta.Ann Thorac Surg. 1989;47:193-203. Johnstone JK, Slaiby JM, Marcaccio EJ, Chong TT, Garcia-Toca M. Endovascular repair of mycotic aneurysm of the descending thoracic aorta.Ann Vasc Surg. 2013;27:23-8. Dubois M, Daenens K, Houthoofd S, Peetermans WE, Fourneau I. Treatment of mycotic aneurysms with involvement of the abdominal aorta:single-centre experience in 44 consecutive cases.Eur J Vasc Endovasc Surg. 2010;40:450-6. Gross C, Harringer W, Mair R, et al. Mycotic aneurysms of the thoracic aorta.Eur J Cardiothorac Surg. 1994;8:135-8. Smith JJ, Taylor PR. Endovascular treatment of mycotic aneurysms of the thoracic and abdominal aorta:the need for level I evidence.Eur J Vasc Endovasc Surg. 2004;27:569-70. Clough RE, Black SA, Lyons OT, et al. Is endovascular repair of mycotic aortic aneurysms a durable treatment option?.Eur J Vasc Endovasc Surg. 2009;37:407-12. Walsh SR, Tang TY, Sadat U, et al. Endovascular stenting versus open surgery for thoracic aortic disease:systematic review and meta-analysis of perioperative results.J Vasc Surg. 2008;47:1094-8. Heath AJ, Day CP, Buckenham TM. Outcomes of infective aneurysm repairs in the New Zealand thoracic stent database.ANZ J Surg. 2011;81:713-6. Kyriakides C, Kan Y, Kerle M, et al. 11-year experience with anatomical and extra-anatomical repair of mycotic aortic aneurysms.Eur J Vasc Endovasc Surg. 2004;27:585-9. Kim HH, Kim DJ, Joo HC. Outcomes of open repair of mycotic aortic aneurysms with in situ replacement.Korean J Thorac Cardiovasc Surg. 2017;50:430-5. Hsu RB, Lin FY. Infected aneurysm of the thoracic aorta.J Vasc Surg. 2008;47:270-6. Zhou T, Guo D, Chen B, et al. Endovascular stent-graft repair of mycotic aneurysms of the aorta:a case series with a 22-month follow-up.World J Surg. 2009;33:1772-8. Yu SY, Lee CH, Hsieh HC, Chou AH, Ko PJ. Treatment of primary infected aortic aneurysm without aortic resection.J Vasc Surg. 2012;56:943-50. Kan CD, Yen HT, Kan CB, Yang YJ. The feasibility of endovascular aortic repair strategy in treating infected aortic aneurysms.J Vasc Surg. 2012;55:55-60. Huang YK, Ko PJ, Chen CL, et al. Therapeutic opinion on endovascular repair for mycotic aortic aneurysm.Ann Vasc Surg. 2014;28:579-89. Kritpracha B, Premprabha D, Sungsiri J, et al. Endovascular therapy for infected aortic aneurysms.J Vasc Surg. 2011;54:1259-65. Sedivy P, Spacek M, El Samman K, et al. Endovascular treatment of infected aortic aneurysms.Eur J Vasc Endovasc Surg. 2012;44:385-94. Lee CH, Hsieh HC, Ko PJ, Chou AH, Yu SY. Treatment of infected abdominal aortic aneurysm caused by Salmonella.Ann Vasc Surg. 2014;28:217-26. Sörelius K, Mani K, Björck M, et al. European MAA collaboratorsEndovascular treatment of mycotic aortic aneurysms:a European multicenter study.Circulation. 2014;130:2136-42. Tiesenhausen K, Hessinger M, Tomka M, et al. Endovascular treatment of mycotic aortic pseudoaneurysms with stent-grafts.Cardiovasc Intervent Radiol. 2008;31:509-13. Silverberg D, Halak M, Yakubovitch D, et al. Endovascular management of mycotic aortic aneurysms.Vasc Endovascular Surg. 2010;44:693-6. Semba CP, Sakai T, Slonim SM, et al. Mycotic aneurysms of the thoracic aorta:repair with use of endovascular stent-grafts.J Vasc Interv Radiol. 1998;9:1 Pt 133-40. Ting AC, Cheng SW, Ho P, Poon JT. Endovascular stent graft repair for infected thoracic aortic pseudoaneurysms--a durable option?.J Vasc Surg. 2006;44:701-5. Heikkinen MA, Dake MD, Alsac JM, Zarins CK. Multiple HIV-related aneurysms:open and endovascular treatment.J Endovasc Ther. 2005;12:405-10. Wang JH, Liu YC, Yen MY, et al. Mycotic aneurysm due to non-typhi salmonella:report of 16 cases.Clin Infect Dis. 1996;23:743-7. Stanley BM, Semmens JB, Lawrence-Brown MMD, et al. Endoluminal repair of mycotic thoracic aneurysms.J Endovasc Ther. 2003;10:511-5. Jones KG, Bell RE, Sabharwal T, et al. Treatment of mycotic aortic aneurysms with endoluminal grafts.Eur J Vasc Endovasc Surg. 2005;29:139-44. Lew WK, Rowe VL, Cunningham MJ, et al. Endovascular management of mycotic aortic aneurysms and associated aortoaerodigestive fistulas.Ann Vasc Surg. 2009;23:81-9. Patel HJ, Williams DM, Upchurch GR, et al. Thoracic aortic endovascular repair for mycotic aneurysms and fistulas.J Vasc Surg. 2010;52:4 Suppl37S-40S. Stellmes A, Von Allmen R, Derungs U, et al. Thoracic endovascular aortic repair as emergency therapy despite suspected aortic infection.Interact Cardiovasc Thorac Surg. 2013;16:459-64. Jia X, Dong YF, Liu XP, et al. Open and endovascular repair of primary mycotic aortic aneurysms:a 10-year single-center experience.J Endovasc Ther. 2013;20:305-10.
REFERENCES
1. Chan FY, Crawford ES, Coselli JS, Safi HJ, Williams TW Jr. In situ prosthetic graft replacement for mycotic aneurysm of the aorta. Ann Thorac Surg 1989; 47:193-203. https://doi.org/10.1016/0003-4975(89)90268-3
2. Johnstone JK, Slaiby JM, Marcaccio EJ, Chong TT, Garcia-Toca M. Endovascular repair of mycotic aneurysm of the descending thoracic aorta. Ann Vasc Surg 2013; 27:23-8. https://doi.org/10.1016/j.avsg.2012.06.004
PMid:23084733
3. Dubois M, Daenens K, Houthoofd S, Peetermans WE, Fourneau I. Treatment of mycotic aneurysms with involvement of the abdominal aorta: single-centre experience in 44 consecutive cases. Eur J Vasc Endovasc Surg 2010; 40:450-6. https://doi.org/10.1016/j.ejvs.2010.07.017
PMid:20719550
4. Gross C, Harringer W, Mair R, et al. Mycotic aneurysms of the thoracic aorta. Eur J Cardiothorac Surg 1994; 8:135-8. https://doi.org/10.1016/1010-7940(94)90169-4
5. Smith JJ, Taylor PR. Endovascular treatment of mycotic aneurysms of the thoracic and abdominal aorta: the need for level I evidence. Eur J Vasc Endovasc Surg 2004; 27:569-70. https://doi.org/10.1016/j.ejvs.2004.01.022
PMid:15121104
6. Clough RE, Black SA, Lyons OT, et al. Is endovascular repair of mycotic aortic aneurysms a durable treatment option? Eur J Vasc Endovasc Surg 2009; 37:407-12. https://doi.org/10.1016/j.ejvs.2008.11.025
PMid:19211280
7. Walsh SR, Tang TY, Sadat U, et al. Endovascular stenting versus open surgery for thoracic aortic disease: systematic review and meta-analysis of perioperative results. J Vasc Surg 2008; 47:1094-8. https://doi.org/10.1016/j.jvs.2007.09.062
PMid:18242941
8. Heath AJ, Day CP, Buckenham TM. Outcomes of infective aneurysm repairs in the New Zealand thoracic stent database. ANZ J Surg 2011; 81:713-6. https://doi.org/10.1111/j.1445-2197.2010.05600.x
PMid:22295312
9. Kyriakides C, Kan Y, Kerle M, et al. 11-year experience with anatomical and extra-anatomical repair of mycotic aortic aneurysms. Eur J Vasc Endovasc Surg 2004; 27:585-9. https://doi.org/10.1016/j.ejvs.2004.02.024
PMid:15121107
10. Kim HH, Kim DJ, Joo HC. Outcomes of open repair of mycotic aortic aneurysms with in situ replacement. Korean J Thorac Cardiovasc Surg 2017; 50:430-5. https://doi.org/10.5090/kjtcs.2017.50.6.430
PMid:29234609 PMCid:PMC5716645
12. Zhou T, Guo D, Chen B, et al. Endovascular stent-graft repair of mycotic aneurysms of the aorta: a case series with a 22-month follow-up. World J Surg 2009; 33:1772-8. https://doi.org/10.1007/s00268-009-0075-6
PMid:19452208
13. Yu SY, Lee CH, Hsieh HC, Chou AH, Ko PJ. Treatment of primary infected aortic aneurysm without aortic resection. J Vasc Surg 2012; 56:943-50. https://doi.org/10.1016/j.jvs.2012.03.018
PMid:22608792
14. Kan CD, Yen HT, Kan CB, Yang YJ. The feasibility of endovascular aortic repair strategy in treating infected aortic aneurysms. J Vasc Surg 2012; 55:55-60. https://doi.org/10.1016/j.jvs.2011.07.077
PMid:22051868
15. Huang YK, Ko PJ, Chen CL, et al. Therapeutic opinion on endovascular repair for mycotic aortic aneurysm. Ann Vasc Surg 2014; 28:579-89. https://doi.org/10.1016/j.avsg.2013.07.009
PMid:24405771
17. Sedivy P, Spacek M, El Samman K, et al. Endovascular treatment of infected aortic aneurysms. Eur J Vasc Endovasc Surg 2012; 44:385-94. https://doi.org/10.1016/j.ejvs.2012.07.011
PMid:22917674
18. Lee CH, Hsieh HC, Ko PJ, Chou AH, Yu SY. Treatment of infected abdominal aortic aneurysm caused by Salmonella. Ann Vasc Surg 2014; 28:217-26. https://doi.org/10.1016/j.avsg.2013.02.021
PMid:24084275
19. Sörelius K, Mani K, Björck M, et al; European MAA collaborators. Endovascular treatment of mycotic aortic aneurysms: a European multicenter study. Circulation 2014; 130:2136-42. https://doi.org/10.1161/CIRCULATIONAHA.114.009481
PMid:25378548
20. Tiesenhausen K, Hessinger M, Tomka M, et al. Endovascular treatment of mycotic aortic pseudoaneurysms with stent-grafts. Cardiovasc Intervent Radiol 2008; 31:509-13. https://doi.org/10.1007/s00270-007-9287-z
PMid:18236107
21. Silverberg D, Halak M, Yakubovitch D, et al. Endovascular management of mycotic aortic aneurysms. Vasc Endovascular Surg 2010; 44:693-6. https://doi.org/10.1177/1538574410377667
PMid:20675323
22. Semba CP, Sakai T, Slonim SM, et al. Mycotic aneurysms of the thoracic aorta: repair with use of endovascular stent-grafts. J Vasc Interv Radiol 1998; 9(1 Pt 1):33-40. https://doi.org/10.1016/S1051-0443(98)70479-8
23. Ting AC, Cheng SW, Ho P, Poon JT. Endovascular stent graft repair for infected thoracic aortic pseudoaneurysms--a durable option? J Vasc Surg 2006; 44:701-5. https://doi.org/10.1016/j.jvs.2006.05.055
PMid:16930927
25. Wang JH, Liu YC, Yen MY, et al. Mycotic aneurysm due to non-typhi salmonella: report of 16 cases. Clin Infect Dis 1996; 23:743-7. https://doi.org/10.1093/clinids/23.4.743
PMid:8909837
26. Stanley BM, Semmens JB, Lawrence-Brown MMD, et al. Endoluminal repair of mycotic thoracic aneurysms. J Endovasc Ther 2003; 10:511-5. https://doi.org/10.1177/152660280301000316
PMid:12932162
27. Jones KG, Bell RE, Sabharwal T, et al. Treatment of mycotic aortic aneurysms with endoluminal grafts. Eur J Vasc Endovasc Surg 2005; 29:139-44. https://doi.org/10.1016/j.ejvs.2004.11.008
PMid:15649719
28. Lew WK, Rowe VL, Cunningham MJ, et al. Endovascular management of mycotic aortic aneurysms and associated aortoaerodigestive fistulas. Ann Vasc Surg 2009; 23:81-9. https://doi.org/10.1016/j.avsg.2008.08.008
PMid:18973981
29. Patel HJ, Williams DM, Upchurch GR, et al. Thoracic aortic endovascular repair for mycotic aneurysms and fistulas. J Vasc Surg 2010; 52(4 Suppl):37S-40S. https://doi.org/10.1016/j.jvs.2010.06.139
PMid:20800423
30. Stellmes A, Von Allmen R, Derungs U, et al. Thoracic endovascular aortic repair as emergency therapy despite suspected aortic infection. Interact Cardiovasc Thorac Surg 2013; 16:459-64. https://doi.org/10.1093/icvts/ivs539
PMid:23287587 PMCid:PMC3598039
31. Jia X, Dong YF, Liu XP, et al. Open and endovascular repair of primary mycotic aortic aneurysms: a 10-year single-center experience. J Endovasc Ther 2013; 20:305-10. https://doi.org/10.1583/13-4222MR.1
PMid:23731302