

Abstract
INTRODUCTION
Adherence to antiepileptic drug (AED) therapy is important for controlling seizures in patients with epilepsy (PWE). It is vital to identify the factors influencing adherence to AED therapy using validated tools. This study aimed to evaluate the pattern and extent of AED adherence among PWE and to identify the factors that influence adherence.
METHODS
This was a cross-sectional study involving PWE who had a confirmed diagnosis. Treatment adherence was assessed using the four-item Morisky Medication Adherence Scale. Univariate analysis with chi-square test was used to observe the association between different variables and AED adherence. Binary logistic regression analysis was used to identify the predictors of adherence.
RESULTS
451 PWE (mean age 27.3 ± 8.1 years) were enrolled in the study; 251 (55.7%) were male and 198 (43.9%) were from the lower socioeconomic class. 326 (72.3%) patients had high adherence to AED therapy, while 125 (27.7%) had low adherence. AED adherence was significantly associated with socioeconomic status (p = 0.043) and type of epilepsy (p = 0.033). However, no significant difference was observed between adherence and age, gender, marital status, epilepsy duration, number and type of AEDs, and occurrence of adverse drug reactions. Patients with focal epilepsy and those from the middle/lower-middle socioeconomic classes were less likely to be nonadherent. The primary reason for nonadherence was forgetfulness.
CONCLUSION
This study found that a majority of PWE have optimal rates of AED adherence and that forgetfulness is the primary reason for nonadherence among PWE.
INTRODUCTION
Epilepsy affects 70 million people worldwide.(1) Long-term antiepileptic drug (AED) administration remains the mainstay of epilepsy treatment. In up to 67% of patients with epilepsy (PWE), AEDs effectively eliminate or reduce the frequency of seizures.(2) Medication adherence refers to the extent to which a patient’s behaviour corresponds with the recommendations of a health professional. Medication adherence is usually better when there is greater patient involvement in the treatment choice, as well as cooperation and mutual agreement between the health provider and the patient.(2) Nonadherence rates among PWE are reported to be 30%–50%.(3) It is well established that patients with suboptimal adherence levels are more likely to have seizures that are associated with increased number of hospital admissions and healthcare costs.(4) Factors influencing adherence to AEDs have been described; these include patient-, treatment- and health system-related factors.(5) The promotion of medication adherence is considered to be an important component of pharmaceutical care practice. Several methods have been used to measure therapeutic adherence, including self-report, pill count, appointment attendance, medication refill history, blood or urine drug levels and drug diary.(6) Indirect methods, such as self-reports and patient interviews, are the simplest and most common methods used for measuring medication adherence.(7,8)
To date, most of the studies conducted to evaluate AED adherence among PWE did not account for the influence of a wide range of variables (e.g. demographic, disease and treatment patterns). There are not many studies in the Indian literature that examine the factors that influence AED adherence. Identifying the factors associated with AED adherence would allow the development of strategies to improve adherence. Thus, the present study aimed to evaluate the pattern and extent of AED adherence among PWE and to identify the factors that influence adherence.
METHODS
This cross-sectional study was conducted by the Division of Clinical Pharmacology at the outpatient and inpatient clinics of the Department of Neurology, St John’s Medical College and Hospital, Bangalore, India, over a period of 1.5 years (January 2012 to July 2013). Ethical approval was obtained from the institution’s Ethical Review Board. Patients aged ≥ 18 years who were receiving AED treatment were eligible for inclusion in the study. Only those who gave their consent for participation were enrolled. Pregnant or lactating women and patients with comorbidities were excluded from the study.
Data was collected using a specially designed case record form that included items on demographic/family history, seizure history, duration of epilepsy, AEDs prescribed and occurrence of adverse drug reactions (ADRs). The participants were classified according to their age, gender, marital status and socioeconomic class. To determine the socioeconomic class of the participants, Kuppuswamy’s socioeconomic status scale was used; the scale takes into consideration the education, occupation and family income of the participants.(9) Epilepsy was diagnosed based on detailed medical history, neurological evaluation by a qualified neurologist, and electroencephalography and neuroimaging techniques (i.e. computed tomography and magnetic resonance imaging). Details on the patients’ AED treatment, including the generic name of the AED, dose and observed ADRs, were also collected.
Adherence to AED treatment was assessed using the four-item Morisky Medication Adherence Scale (MMAS-4),(10) a standardised, validated questionnaire for measuring self-reported medication adherence. The four items of the MMAS-4 assess whether: (a) the patient has ever forgotten to take medication; (b) the patient has ever had problems remembering to take medication; (c) the patient has stopped medication due to worsening symptoms; and (d) the patient has stopped medication due to alleviating symptoms.(11) Each item is scored as either 0 (Yes) or 1 (No). The score of each item is then summed to give a range of scores from 0 to 4. A score of 3–4 suggests that the patient is adherent, while a score of ≤ 2 suggests that the patient is nonadherent.
Data was expressed as frequency (percentage). Descriptive statistical analysis was used to analyse the data, and univariate analysis with chi-square test was used to observe the association between the variables and adherence. Binary logistic regression analysis was used to identify the predicting factors of adherence to treatment. A p-value < 0.05 was considered statistically significant.
RESULTS
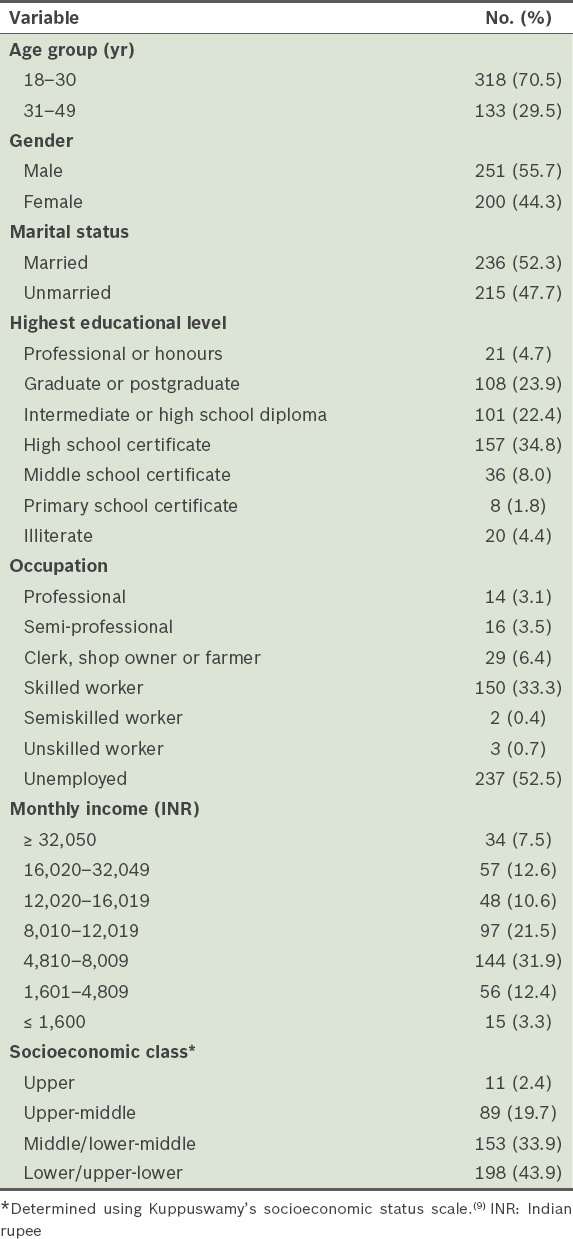
A total of 451 PWE were enrolled in the study. 251 (55.7%) patients were male and the majority (n = 318, 70.5%) were aged 18–30 years (
Table I
Demographic characteristics of the patients with epilepsy (n = 451).
Focal epilepsy was more common in our study cohort (n = 298, 66.1%) than generalised epilepsy (n = 153, 33.9%) (
Table II
Clinical characteristics of the patients with epilepsy (n = 451).
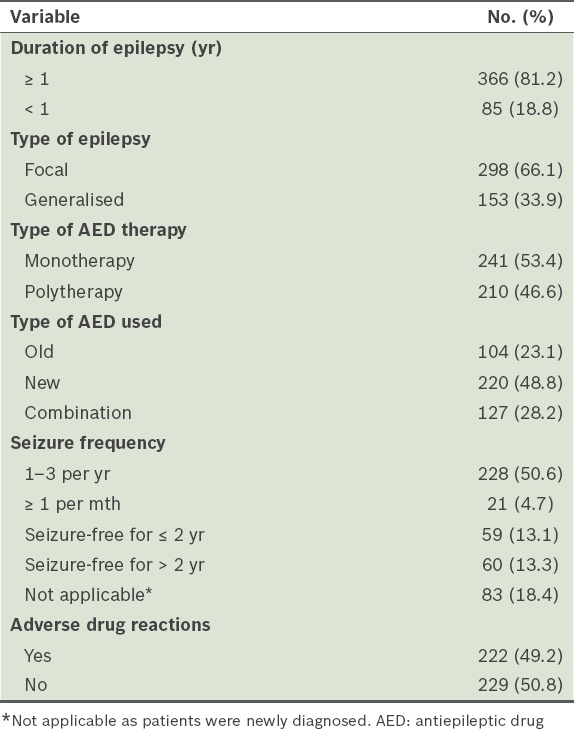
Among the 241 PWE who were prescribed AED monotherapy, the most frequently prescribed old AED was phenytoin (n = 34, 14.1%), followed by valproic acid (n = 30, 12.4%). The new AEDs used in AED monotherapy included oxcarbazepine (n = 66, 27.4%), levetiracetam (n = 53, 22.0%) and topiramate (n = 6, 2.5%). The most common AED dual therapy was oxcarbazepine with clobazam (n = 31, 19.4%), and the most frequently used add-on AED was clobazam (58.2%). Patients with focal epilepsy received phenytoin, carbamazepine, oxcarbazepine and/or levetiracetam, while those with generalised epilepsy received valproic acid, levetiracetam and/or lamotrigine.
Among the 451 PWE, 222 (49.2%) reported having ADRs; of these, 175 (78.8%) had ADRs involving the central nervous system (e.g. impaired memory, tiredness, drowsiness, headache and depression), 15 (6.8%) had aphthous ulcers, 10 (4.5%) experienced weight gain, 7 (3.2%) had gastritis, 6 (2.7%) had bone pain, 5 (2.3%) had rashes and 4 (1.8%) had pimples.
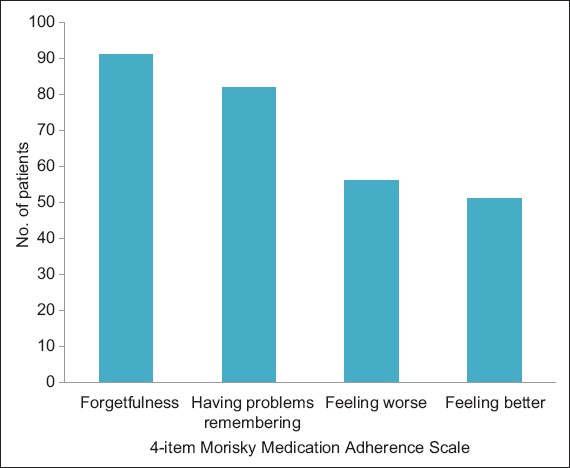
A small proportion of the PWE (27.7%) answered “Yes” (i.e. indicated nonadherence to AED therapy) to at least one of the four items in the MMAS-4 questionnaire. Forgetfulness was the most common reason for nonadherence (n = 91, 32.5%) followed by having problems remembering (n = 82, 29.3%) and stopping medication when feeling worse (n = 56, 20.0%) or when feeling better (n = 51, 18.2%) (
Fig. 1
Bar graph shows the reasons for nonadherence to antiepileptic drug therapy among patients with epilepsy.
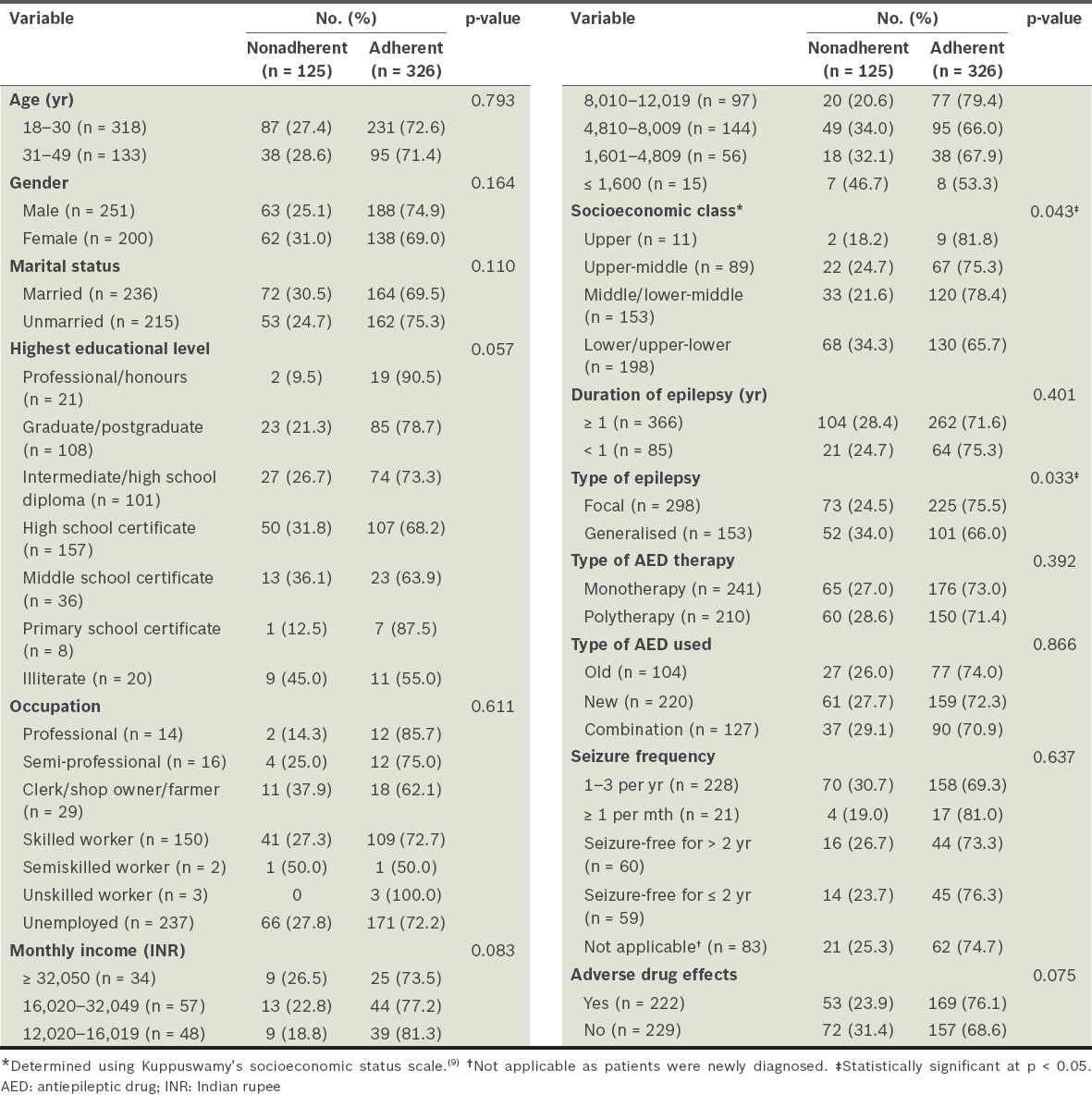
Based on the results of MMAS-4, 326 (72.3%) of the PWE were adherent and 125 (27.7%) were nonadherent to AED therapy. Socioeconomic status and type of epilepsy were found to be significantly associated with adherence (p = 0.043 and p = 0.033, respectively), while age, gender, marital status, duration of epilepsy, type of AED therapy, type of AED used and the occurrence of ADRs were not found to be significantly associated with adherence (
Table III
Results of univariate analysis comparing patients with epilepsy who were adherent and nonadherent to medication (n = 451).
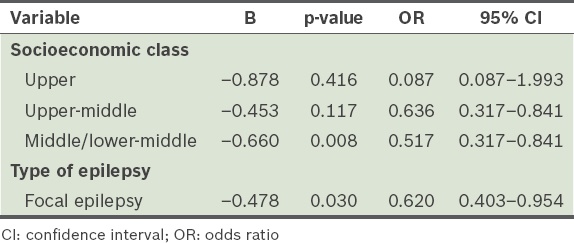
Factors that were found to be significantly associated with medication adherence in the univariate analysis (i.e. socioeconomic class [p = 0.043] and type of epilepsy [p = 0.033]) were included in the multiple regression analysis. The results of the multiple logistic regression analysis are summarised in
Table IV
Results of the logistic regression analysis evaluating the factors associated with nonadherence.
DISCUSSION
Adherence to AED is a challenge in the management of epilepsy. Although poor adherence is considered to be one of the major causes of non-responsiveness to AED therapy, this has not been studied extensively in India. Hence, we assessed the extent of AED adherence, as well as the factors influencing AED adherence among PWE.
Few studies have used self-reporting measures of adherence to assess adherence among PWE.(12,13) MMAS-4 was used in the present study and it showed that the majority (72.3%) of PWE in our study cohort adhered to the prescribed regimen. Another study that used a self-reporting measure of adherence reported a 51.9% adherence rate.(13) These results suggest that the PWE in our study were more adherent to their prescribed medication than patients in other studies that assessed adherence using self-reporting measures. Differences in the rate of adherence may be due to the unique characteristics of the study populations (e.g. differences in the patient attitude toward adherence due to cultural or educational influences, or clinicians’ approach) and differences in the criteria used to measure adherence.(14)
In the present study, we did not find any significant differences in the rate of nonadherence among the age groups and between the genders. This finding is similar to that of Liu et al’s study,(13) which did not find any demographic differences (i.e. gender and age) between AED-adherent and AED-nonadherent patients. A study by Johnbull et al(15) reported a similar observation, in that gender did not affect the adherence rate in their study.
We found a significant association between AED adherence and lower/upper-lower socioeconomic class. This is in contrast to the findings of Asadi-Pooya,(12) who found no significant association between AED adherence and socioeconomic status (measured based on parental smoking, place of residence and educational level). In a study conducted by Das et al in India,(16) the following socioeconomic factors were found to be related to discontinuation of AED treatment: unemployment; loss of job; marital disharmony; spiritual illusions about epilepsy; and lack of availability of medications in local areas. The findings of the present study suggest that PWE who are of a lower socioeconomic class (based on Kuppuswamy’s socioeconomic status scale, which takes into account education, occupation and income)(9) may be at a higher risk of nonadherence.
In the present study, the duration of epilepsy did not have a significant association with adherence among the PWE. This finding is similar to the results reported by Gabr and Shams,(17) but differs from the results of Kyngäs’ study, which showed that a duration of epilepsy > 3 years was significantly related to adherence to medications.(18) However, a significant association between generalised epilepsy and nonadherence to AED was found in the present study, as well as in the study by Samsonsen et al;(19) the reason for this observation is elusive. One possible explanation that may account for the higher rate of adherence is that episodes of focal epilepsy are more frequent than generalised epilepsy. However, Liu et al(13) did not find any relationship between the type of epilepsy and adherence. In terms of frequency, we did not find any significant association between frequency of seizure and adherence in our study, unlike Gabr and Shams,(17) who found that seizure frequency was higher among PWE who were nonadherent.
Our findings regarding the influence of AED therapy type on the extent of adherence are in agreement with those of Sweileh et al.(20) Both studies showed no significant difference in medication adherence between patients on monotherapy and those on polytherapy. In contrast, the studies by Gabr and Shams,(17) Bautista and Rundle-Gonzalez(21) and Harimanana et al(22) found that patients on monotherapy were significantly more adherent to medication than those who were on polytherapy. This has been attributed to the complexity of a treatment regimen(7) involving a larger number of pills that need to be taken at different time intervals, which increases the likelihood of missed doses.(23) In the present study, we did not find any significant relationship between the occurrence of ADRs and adherence, even though ADRs that are related to the central nervous system may increase the likelihood of nonadherence. Our finding differs from that of Martins et al’s study,(6) which found a statistically significant association between the occurrence of ADRs and AED adherence among their cohort, which consisted mainly of patients suffering from juvenile myoclonic epilepsy.
Multiple logistic regression analysis of the patient demographics and clinical factors revealed that socioeconomic status and type of epilepsy were the variables that best explained nonadherence in our cohort. Other than that, the most common reason for nonadherence was forgetfulness of PWE. This finding is in accordance with those of studies conducted by Liu et al(13) and Paschal et al,(24) who reported that the primary reason for nonadherence in their study cohort was forgetfulness (69.6% and 32.5%, respectively). Johnbull et al(15) observed that forgetfulness was the reason for nonadherence in only 40.7% of their study cohort.
MMAS-4, which is a validated and reliable tool with a significant linear relationship with adherence, was used to measure adherence in our study. However, this tool has the disadvantage of recall bias, and hence, has the tendency to overestimate adherence level. In order to reduce the bias related to the assessment of adherence using the four-item scale, it has been suggested that the responses given by PWE should be cross-verified with data on prescription refills and/or the number of AEDs remaining with the patients, wherever possible.
To conclude, the present study found that socioeconomic class and type of epilepsy have a significant influence on the adherence of PWE to AED therapy, and that forgetfulness is the primary reason for AED nonadherence among PWE. The only limitation of the present study was that it was carried out in a tertiary healthcare setting, which made it difficult for us to extrapolate our findings to the general population. We suggest that further studies be conducted using multiple validated tools to measure adherence in a more varied population in order to better address the issue of AED adherence among PWE.