

Abstract
In Singapore, the newborn screening programme was started in 1965 in order to reduce the high neonatal mortality and neurological morbidity owing to severe hyperbilirubinaemia caused by erythrocyte glucose-6-phosphate dehydrogenase deficiency. About 25 years later, the national newborn screening for congenital hypothyroidism was established. Subsequently, universal newborn hearing screening and screening for multiple inborn errors of metabolism using tandem mass spectrometry were introduced as national programmes in 2003 and 2006, respectively. All these programmes are widely accepted as standards of care, and practically every newborn is screened despite the absence of any legislation. Two other evidence-based bedside screening tests, namely pulse oximetry screening for critical congenital heart disorders and physical examination of the hips for developmental dysplasia of the hips with selected ultrasonographic screening have been widely performed in hospitals, and they are soon expected to be in the national screening programmes.
INTRODUCTION
In 1963, mass newborn screening to detect phenylketonuria was conducted in America by Dr Robert Guthrie, the father of newborn screening.(1) The method of collecting heel-stick blood samples on filter paper was simple and showed good sensitivity, establishing the feasibility of conducting mass newborn screening. Almost all the affected children were managed with dietary treatment to prevent developmental retardation. Newborn screening in Singapore was started in 1965, wherein the umbilical cord blood was screened to detect erythrocytic glucose-6-phosphate dehydrogenase (G6PD) deficiency to prevent mortality as well as neurodevelopmental morbidity due to severe hyperbilirubinaemia.(2)
The huge success of these programmes fuelled enthusiasm to extend screening for other disorders. In 1975, Dussault et al(3) reported a method of screening for congenital hypothyroidism (CH). Within 15 years, in 1990, screening for CH was established in Singapore. Nationwide screening for hearing impairment (HI) and screening for inborn errors of metabolism (IEM) using tandem mass spectrometry (TMS) were introduced in 2002 and 2006, respectively.(4) Current neonatal screening includes screening for disorders detectable by not only invasive blood collection for analysis of the samples but also bedside clinical testing. These include pulse oximetry screening for critical congenital heart disorders and screening for developmental dysplasia of the hips (DDH).
Neonatal screening for G6PD deficiency, CH, HI and IEM form one prong of a multipronged National Health Policy for the prevention of neurodevelopmental delay and mental retardation. All these programmes are widely accepted as standards of care, and practically every newborn is screened despite the absence of any legislation or national funding. The screenings are hospital based, and an advisory committee is periodically convened by the Ministry of Health (MOH) to consider developments in neonatal screening from a national perspective. In this article, the lessons learned from experience with the various neonatal screening programmes, the issues that have arisen and the future possibilities of further expansion of screening are described.
SCREENING FOR G6PD DEFICIENCY
In Singapore, severe hyperbilirubinaemia resulting in kernicterus used to be the leading cause of neonatal mortality and neurodevelopmental disability in the 1950s and 1960s. A clinical study revealed that the aetiology of severe hyperbilirubinaemia was secondary to haemolytic crisis due to red cell G6PD deficiency in 43% of the cases and liver immaturity in 25% of the cases.(2,5,6) In 1964, the Kernicterus Surveillance Programme was introduced, and in the subsequent year, a mass newborn screening programme for G6PD deficiency was started. This initiative was highly successful in Singapore, and thereafter, deaths from kernicterus decreased substantially from 150 in 1950s to just five in the late 1980s. The G6PD screening programme has been well established, with very high social acceptance. Since the 1990s, kernicterus has virtually been eradicated from Singapore. (5-7)
G6PD is an X-linked enzyme, and its deficiency is one of the most frequent hereditary abnormalities. Screening for G6PD is performed by quantitative measurement of red cell G6PD activity in umbilical cord blood. The tests are performed at the hospital at birth and the results are usually available within 12 hours. Initially, infants with G6PD deficiency are kept in the hospital for 21 days after birth for close observation and treated with phototherapy in the presence of significant jaundice. Parents are educated regarding the consequences of the abnormality and the triggers that precipitate haemolysis. The G6PD status is recorded in the health book of the infant, and written information in the form of a booklet containing the details about G6PD deficiency is provided to the parents. Screening has revealed an overall incidence of 1.6%–2.5%, with a 3.15% incidence in males and 0.11% in females. A distinct ethnic variation in the incidence has also been reported among male infants (Chinese 3.94%, Malays 2.95% and Indians 0.66%), and intermediate deficiency (1.83%) has been identified in Chinese female infants.(4,8) Three common molecular variants have been identified among the Chinese in Singapore, and six different variants have been identified among Malays.(9)
The practice of prolonged stay in the hospital, which emerged during the Kernicterus Surveillance Programme, continued for about three decades. Hospital stay was subsequently reduced to two weeks of inpatient stay, after the establishment of several primary care outpatient centres (polyclinics) in the country.(4,10,11) Experience and clinical studies conducted in the local population revealed that two clinical syndromes occur during the neonatal period in babies with G6PD deficiency: haemolytic jaundice with severe hyperbilirubinaemia occurring mainly during the first week of life and non-haemolytic hyperbilirubinaemia with lower levels of serum bilirubin but prolonged jaundice occurring in the absence of haematological evidence of haemolysis. The latter is probably due to co-existence of Gilbert’s syndrome.(12) Studies have also shown that significant hyperbilirubinaemia usually occurs only during the first week of life, and infants who do not develop haemolytic jaundice during the first week are unlikely to develop it during the second week of life in the absence of trigger exposure.(4) Moreover, as high as 43%–55% of infants with G6PD deficiency never develop hyperbilirubinaemia. Parents are also less keen for their babies to stay in the hospital for more than a few days in the absence of significant jaundice requiring phototherapy. By early 2000, scientific evidence encouraged paediatricians and neonatologists to cautiously reduce the duration of hospitalisation to seven days. Since the last decade or so, babies without risk factors and those without significant jaundice in the first three days are discharged on Day 4 of life. (10,11,13) After discharge, these infants are closely monitored for jaundice and anaemia on an outpatient basis, either in the polyclinic or hospital, for two to three weeks.
This early discharge strategy for high-risk infants has been observed to be safe and has also reduced the social, emotional and financial burden of G6PD deficiency in Singapore. Moreover, in accordance with baby-friendly initiatives, breastfeeding and maternal-infant bonding have been facilitated, without any reported case of bilirubin-induced encephalopathy resulting in kernicterus. However, babies with G6PD deficiency should not be considered as low-risk infants; monitoring for jaundice, watchfulness and education of the parents must be continued by the younger generation of specialists and doctors.
SCREENING FOR CONGENITAL HYPOTHYROIDISM
Screening for CH in Singapore began in 1981 as an 18-month pilot research study in Kandang Kerbau Hospital, the then largest maternity hospital, where about 50% of the national births occurred.(14) The success of the programme and the experience gained led to its establishment in 1985 as a standard service at the National University Hospital (NUH). In 1990, it became a national programme.(15)
Cord blood was used for the screening, because this was already being collected for screening of G6PD deficiency. Another reason was that the majority of newborns were discharged from hospital within 48 hours of birth. Initially, the pilot programme used an isotope-based T4 supplemental thyroid-stimulating hormone (TSH) strategy. With the advent of enzyme immunoassays, the strategy changed to a primary TSH strategy, which has continued till today. The TSH cut-off for recall has been set at the 99th centile. This corresponded with a TSH value of 23 mIU/L. Babies who screen positive have a T4 measurement on the original cord serum specimen and are recalled for evaluation between Days 3 and 5. Those with extreme values are evaluated earlier. CH was diagnosed if serum TSH values remained > 20 mIU/L in the first week of life and the T4 values were below the age-specific mean. Prior to initiating treatment, radiography of the knee to assess bone age and radioisotope thyroid scan were performed whenever feasible. We found that in the majority of our patients, a starting dose of 25 mcg of thyroxine (8 mcg/kg/day) was sufficient to bring both the TSH and the fT4 values into the normal range within about two weeks of instituting therapy. With this strategy and threshold, permanent CH was being diagnosed at a rate of about one in 3,000 births.(16,17)
However, screening for CH has faced some challenges over the years. The first is attributable to the use of at least three different TSH analysers across the different hospitals in Singapore. Each analyser has a reference range that is slightly different from that of another. In a recent comparison, the range between the analysers was about 4 mIU/L at the 99th centile. This difference makes it necessary for cut-offs to be analyser specific and, by itself, is not technically difficult. However, it creates difficulties when parents compare the TSH values of their babies or when healthcare professionals have to evaluate a TSH value without knowing the analyser that was used. In order to unify the differences in the TSH analysers, the cut-off for the cord serum TSH value was revised to ≥ 25 mIU/L in the year 2000. In an audit conducted between August and December 1996 on a sample population of 145,843 newborn infants from the three restructured hospitals, 62 cases of CH were detected by the primary cord blood screening programme. This yielded an incidence of one in 2,350 births, with a female preponderance (sex ratio 2:1). Technetium isotope study of the thyroid revealed ectopia in 52% of the cases, eutopia in 33% of the cases and agenesis in 10% of the cases. Osseous maturation was delayed in 75% of the cases, signifying fetal onset of hypothyroidism. Follow-up study showed that about 20% of the infants who were initially diagnosed as having CH and treated had only transient hypothyroidism, and thyroxine could be weaned off between 2.5 and 3 years of age.
The second challenge arose from the global observation that not every newborn with CH can be identified using any single strategy or cut-off value. The current understanding is that 10%–15% of CH cases may not be identified. In a recent local unpublished analysis, it was found that, in a screened population of about 12,000 newborns, nine babies with CH were identified using a TSH cut-off of 25 mIU/L. Two additional cases were identified when the physician in charge decided to investigate babies with a TSH value that was slightly lower than the 99th centile (24.6 mIU/L and 24.9 mIU/L). This meant an almost 20% difference in incidence, which was significant.
It should be noted that central CH and delayed-onset primary CH many not manifest as biochemical abnormalities during the first few days of life and may, therefore, be missed by our screening methodology. Moreover, none of the existing newborn screening strategies can identify all cases of CH, and hence, if any infant presents with clinical signs suggestive of hypothyroidism (such as prolonged jaundice, constipation, hypothermia, hypotonia, poor feeding, macroglossia, large anterior fontanelle or open posterior fontanelle), thyroid function tests (TSH and fT4) need to be performed urgently, even if cord blood screening yields normal results.
The third challenge arises from the recognition that the primary TSH measurement does not screen for central CH, a much rarer condition with highly variable fT4 and TSH values in the newborn period. This issue was previously explored when the national programme was being developed. It showed that the strategy of measurement of T4 and TSH markedly increased the number of babies that were recalled but did not yield a case of central CH.(15) Use of fourth-generation analysers along with thyroxine-binding globulin assays in the Netherlands has generated practical and feasible outcomes.(18)
The fourth challenge is the need to establish age-specific and local reference ranges in the first two weeks of life for the new generation of TSH and fT4 analysers. The Perinatal Society of Singapore, in collaboration with the College of Paediatrics and Child Health, has set up a professional group to study the above issues and propose national-level solutions. These are expected by the end of the year.
Early and adequate treatment of CH in infants have shown excellent prognosis for growth, puberty and neurodevelopmental outcomes, and disappearance of intellectual disabilities with intelligence quotient (IQ) < 70. Grosse et al(19) reported that the mean global IQ of patients identified early was 10–30 points higher than that of patients in the pre-screening stage. Cognitive outcome has been correlated with the age of onset of therapy, thyroxine dose, compliance with medication and the parents’ socio-educational status.(20,21) However, despite early diagnosis by neonatal screening and treatment, subtle defects in sensorimotor function, memory deficits and reduced hippocampal volumes have been reported in children and adolescents, which have been correlated with the severity of CH at birth.(22) By contrast, the cognitive and behavioural defects in infants with delayed diagnosis and treatment depend on the severity of CH and the time taken to achieve biochemical euthyroidism.
SCREENING FOR HEARING IMPAIRMENT
Hearing is closely linked to speech and language development. Even mild to moderate levels of hearing loss (HL) can lead to changes in the brain.(23) Evidence-based research supports that early identification and subsequent intervention within the first six months of life are critical to realise the benefits of early experience with language and sound.
In the past, students with severe HI used to receive their primary education in the School for the Deaf or the Canossian School for the Deaf. These students required eight years to complete their primary education instead of the usual six, and they also scored lower than their normal-hearing peers did in the Primary School Leaving Examination.(24) The median age at diagnosis of HI was 20.8 (range 0–86) months. Hearing aids were fitted at a median age of 42.2 (range 1–120) months. A greater delay in intervention was associated with poorer academic outcomes. Late diagnosis of congenital HI can result in significant delays in speech, language, and intellectual, social and emotional development.
Congenital HI is one of the most common disorders worldwide. In Singapore, the incidence of HI of any severity is 3–4 per 1,000 infants. HI is not a visible condition at birth; most children with congenital HL are born to normal-hearing parents and have no health issues or risk factors for HL.
The pilot screening for HL in newborns began in a restructured hospital in 1995.(25) In 2000, a study on the early detection and intervention of HI among children in Singapore recommended that a national Universal Newborn Hearing Screening (UNHS) programme was highly feasible and required a software programme for tracking.(26) The UNHS programme was started in 2002 in KKH as a Health Service Development Programme (HSDP) funded by the MOH, and became a fully paid service in KKH and a national programme in 2003.
The UNHS programme aimed to screen 95% of all infants by one month of life and to diagnose and provide intervention for HI by six months of life, in keeping with the recommendations by the Joint Committee of Infant Hearing of the American Academy of Pediatrics.(27) Guidelines on the establishment of the UNHS programme were reported by Lim and Daniel in 2008.(28) The UNHS is now implemented in all Singapore hospitals with obstetric service; hence, most infants born locally would have been screened, unless an infant was very unwell or the parents declined the screening. Congenital HI is detected by two methods, namely the automated auditory brainstem response (AABR) and otoacoustic emission (OAE) tests; both these methods are noninvasive. AABR detects neurosensory defects and has a lower repeat rate than OAE does; however, the former is more expensive and may require a longer time to complete.
All hospitals in Singapore follow a two-step protocol, and any infant that does not pass the second screen would be referred to the otolaryngology department for further evaluation. KKH and Singapore General Hospital (SGH) use the AABR screen for all newborns; at-risk infants also undergo OAE screening. NUH uses the OAE screen for all their newborns, and their at-risk infants also undergo AABR screening. Most private hospitals also follow the two-step protocol using AABR or OAE. A hearing screening can be done as early as six hours of age, which allows for re-screening of some infants later during their hospital stay. This inpatient re-screening of an infant with a ‘refer’ result has been shown to reduce the chance of false positive results.(29) The outpatient re-screen is done 3–6 weeks after discharge, and any child with poor emissions is referred to the otolaryngology department for further evaluation of any HI.
Although the UNHS programme recommends that all newborns should be screened for HI after birth, some infants are more susceptible to HI. These at-risk categories are listed in
Box 1
Risk factors during infancy for hearing impairment or progressive hearing loss in childhood;
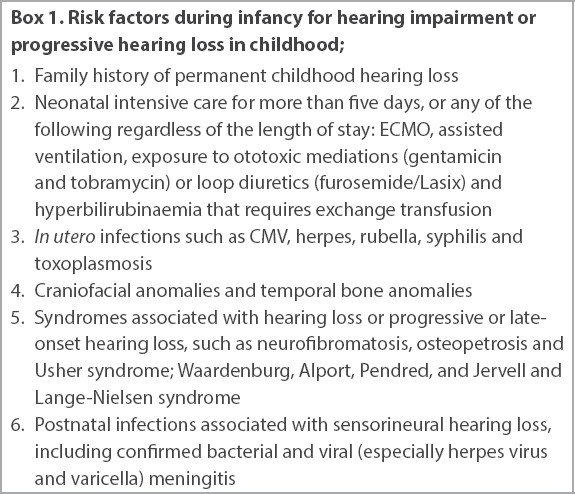
Data from KKH from January 2010 to December 2019 showed that 116,495 infants (99.9% of all eligible infants) underwent the UNHS. Of these, 1,162 (1%) were referred to the otolaryngology department for further evaluation and, to date, we have detected 376 (42.6%) infants with HL, yielding an incidence of HI of any severity of 3.2 per 1,000 infants. Severe profound HI was observed in 1.6 per 1,000 infants. 60.4% of the infants with HI had sensorineural HL and 3.5% of the infants had mixed HL. 55% of these infants had bilateral HI. Hearing aids were fitted for 150 infants. 25 infants with bilateral severe profound HI who did not adequately benefit from hearing aids and auditory-verbal therapy went on to have cochlear implants. 56 infants were medically treated for conductive HI, whereas 38 infants were surgically treated as well. A post-UNHS implementation study showed that the median age at diagnosis of HI was 4.8 (range 1–24) months. Hearing aids were fitted at a median age of 7.6 (range 2–45) months.(32) The hearing screening programme in Singapore has not only allowed for the diagnosis and early intervention of congenital HI in a considerable number of infants, thus providing them an opportunity for development of normal speech and language, but has also shown the value of repeat screening in high-risk infants.
The latest guidance on childhood developmental screening announced by the MOH on July 2020(33) has acknowledged the UNHS programme. It advises all clinicians to ensure that the UNHS result is checked in the health booklet upon the infant’s first visit, in order to ensure that the child has passed the hearing screen or to decide whether the child should be referred for further evaluation.
The best indication of the success of the UNHS programme in Singapore was the closure of the Singapore School for the Deaf in 2017 owing to its ‘dwindling enrolment’. This is attributable to the medical advances in screening, early diagnosis and provision of assistive devices, which has enabled most children with HI to hear well enough to attend mainstream schools.
SCREENING FOR INBORN ERRORS OF METABOLISM
Expansion of newborn screening by tandem mass spectrometry
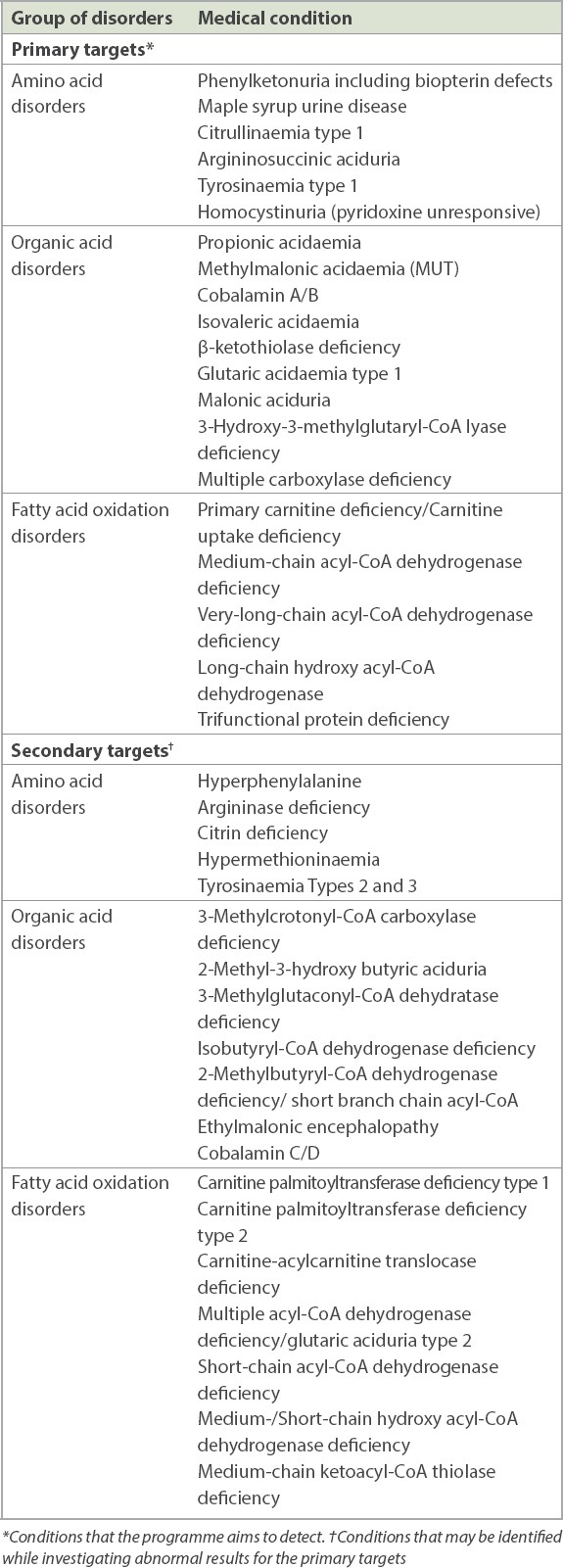
In Singapore, prior to 2005, newborn screening was available for G6PD deficiency, hypothyroidism and HL. The development of electrospray ionisation tandem mass spectrometry (MS/MS) in the 1990s was critical in the expansion of newborn screening. A single dried blood spot test is applied for the simultaneous screening of a number of disorders, including amino acidopathies, fatty acid oxidation disorders and organic acidaemias. The primary and secondary disorders that the screening programme aims to detect are shown in
Table I
List of primary and secondary targets of the expanded newborn screening programme by tandem mass spectrometry.
After much deliberation, in 2004, the National Newborn Advisory Committee approved the proposal to expand newborn screening to include IEM using TMS. In 2005, a Health Service Development Programme (HSDP 04/X03) Award was given to evaluate and implement newborn screening for IEM by MS/MS. This was done through a collaborative partnership among KKH, NUH and SGH.
A successful screening programme requires careful planning and integration of a comprehensive infrastructure involving education, screening, follow-up of abnormal results, diagnosis, treatment/management and evaluation of the system. Prior to the commencement of the pilot programme at KKH, a team comprising a senior neonatologist, paediatric metabolic specialist, scientific officer and medical technologist was sent to Adelaide, South Australia to be trained at the South Australian Neonatal Screening Centre for about a month.
Education
The initial challenge for the pilot programme in attracting private hospitals was a lack of knowledge of IEM and scepticism regarding the prevalence of these disorders in the local population. Correspondingly, there was a lack of interest among the general public and health professionals. In response, the team developed and printed information brochures in three languages; released educational videos; and conducted seminars for the health professionals, public and media.
Moreover, we also introduced and taught proper collection of dried blood spots to healthcare professionals. Our guidelines called for all infants, regardless of gestational age and feeding status, to have their samples taken for screening at more than 24 hours of age. Further, we had a premature newborn (< 36 weeks) protocol, which was adapted from the Clinical and Laboratory Standards Institute’s guidelines.(34) It required the collection of three specimens — the first sample at 24–72 hours, second sample at two weeks of life and third sample at four weeks of life.
The pilot programme: a preview of the population disease distribution and frequency
The expanded newborn screening programme based at KKH started in the public hospitals in July 2006 and progressed in phases to include the private sector. To encourage participation in the public hospitals, a subsidised cost scheme for participation in the pilot programme was instituted. During the pilot phase, between July 2006 and July 2010, 61,313 newborns were screened. A total of 20 newborns were diagnosed with a variety of IEM (three medium-chain acyl-CoA dehydrogenase deficiency, one carnitine uptake defect [CUD], one very long-chain acyl-CoA dehydrogenase deficiency, one short-chain acyl-CoA dehydrogenase deficiency, three 3-methylcrotnyl carboxylase deficiency [3-MCC], two glutaric acidaemia type I, one citrin deficiency, one methylmalonic acidaemia, one cobalamin C metabolism defect, one ornithine transcarbamylase deficiency, one 6-pyruvoyl-tetrahydropterin synthase deficiency, and four maternal conditions – one 3-MCC, one vitamin B12 deficiency, two CUD), yielding a detection rate of one in 3,000.(35)
Since its implementation until December 2020, the IEM screening programme has screened 404,227 newborns across Singapore. A total of 131 true positive cases were detected, of which 47 were organic acidaemias; 44 were fatty acid oxidation disorders; 23 were amino acidopathies; and 17 were assorted cases of maternal deficiencies of vitamin B12, 3-MCC and primary carnitine. The detection rate of IEM in Singapore is one in 3,158 live births, which is similar to the detection rates reported in other countries. Of note, this test is not efficient in screening for citrin deficiency, an amino acid disorder prevalent in the local and Asian population. The overall sensitivity and specificity of this test are 85% and 99.9%, respectively. The cumulative positive predictive value and recall rate for retests are acceptable (26% and 0.1%, respectively). The current participation rate of all birthing hospitals (private and public) is 92% of the annual live births.
Laboratory support and clinical follow-up team
The NBS MS/MS programme is supported by a rapid-response centralised confirmatory/diagnostic testing laboratory and a rapid-response team of metabolic specialists. The close collaboration between the screening laboratory and the two metabolic services located at KKH and NUH ensured that patients are seen within 24–48 hours of referral and that the same methodologies are used in evaluating the patients. In our experience of over 100 cases, more than 97% of presumptive positive patients were evaluated by a metabolic specialist within seven days of birth. Of these, 92% were clinically asymptomatic and another 4% had mild symptoms. After the clinical evaluation, samples were collected for confirmatory testing. Treatment was initiated if appropriate and necessary, and genetic counselling was also offered.
Evaluation of the system in the centralised laboratory
From the outset, we formulated a protocol for patient referral and follow-up, and established a laboratory quality system for both the MS/MS screening and diagnostic testing platforms. This ensured a robust and quick turnaround time in patient care. Our participation in the Collaborative Laboratory Integrated Reports programme helps us to evaluate our performance metrics (positive predictive value, false positivity rate, sensitivity, specificity) against those of other international programmes in Asia, Asia Pacific, Europe and America. Critical indicators are monitored and evaluated via external laboratory proficiency testing and assessment schemes such as CDC (Center for Disease Control and Prevention) and ERNDIM (European Research Network for evaluation and improvement of screening, Diagnosis and treatment of Inherited disorders of Metabolism).
Expanding the scope of testing in the newborn screening panel
In October 2019, we expanded the scope of testing to include five more disorders in the newborn screening panel, namely congenital adrenal hyperplasia, biotinidase deficiency, severe combined immunodeficiency syndrome, galactosaemia and cystic fibrosis.
This was accomplished in a partnership with PerkinElmer to establish KKH as a Centre of Excellence for Newborn Screening. Through this partnership, new laboratory equipment and instrumentation (Genetic Screening Processor, Victor EnLite) were introduced and validated in a pilot programme to screen for the disorders. In preparation for the launch, we expanded and recruited additional specialists (in the departments of endocrinology, respiratory and immunology) in the follow-up teams at both metabolic services at KKH and NUH. Recent one-year data (n = 35,888) since the launch of the newly revised panel showed positive screens in detecting congenital adrenal hyperplasia (one case), biotinidase deficiency (one case) and several cases of T-cell lymphopenia (three syndromic, two unresolved, four resolved) that were not related to severe combined immunodeficiency syndrome. The recall rate for the five tests was 0.04%–0.34%, with cystic fibrosis having the highest recall rate. The laboratory is currently fine-tuning the parameters and algorithms to further reduce this recall rate.
PULSE OXIMETRY SCREENING
Critical congenital heart defects (CCHD) are the most serious form of congenital heart defects; these require invasive intervention or they could result in death within the first year of life. The incidence of CCHD is 2–3 per 1,000 live births. (36) Pre-symptomatic diagnosis of CCHD has been shown to improve mortality and morbidity. The initial feature of mild hypoxaemia that is present in most cases of CCHD may not be clinically discernible. Screening using pulse oximetry has been found to be beneficial, cost-effective, safe and simple to perform. Many centres worldwide have included pulse oximetry in their newborn screening programmes.
The primary targets for pulse oximetry screening are hypoplastic left heart syndrome, pulmonary atresia, tetralogy of Fallot, total anomalous pulmonary venous return, transposition of great arteries, tricuspid atresia and truncus arteriosus.(37) Other cardiac defects that less consistently cause hypoxia in newborns may also be detected.
A meta-analysis of 19 studies with almost 440,000 patients reported that pulse oximetry had a 76.3% sensitivity, 99.9% specificity and a false positivity rate of 0.14% for detection of CCHD.(38) In another meta-analysis, the sensitivity of postnatal physical examination alone for the detection of CCHD was 53%; however, the sensitivity improved to 92% when physical examination was combined with pulse oximetry screening.(39) It has been estimated that pulse oximetry screening, in combination with antenatal ultrasound and postnatal physical examination, can identify 92%–96% of infants with CCHD.(40) State-wide implementation of mandatory pulse oximetry screening in the US has been associated with 33.4% reduction in early infant cardiac deaths, compared with the rate in states without these policies.(41)
Between 27% and 77% of the false positives have significant non-CCHD pathologies that require immediate treatment or follow-up, such as respiratory conditions (e.g. persistent pulmonary hypertension, congenital pneumonia, transient tachypnea of newborn, pneumothorax, meconium aspiration syndrome), sepsis and non-critical cardiac defects.(36) The detection of these cases allows for early management, and therefore, they are sometimes regarded as secondary targets of pulse oximetry screening.
The false positivity rate is higher (0.42%) when screening is performed within 24 hours of birth compared with after 24 hours of birth (0.06%).(38) Although early screening with higher false positivity rates may increase the number of investigations, it helps in earlier detection of significant non-CCHD pathologies. The lower false positivity rates with later screening have to be balanced against the risk of deterioration before screening. These are important considerations in the settings of early discharge before 24 hours of life and in home births, in which pulse oximetry screening has been found to be feasible.(42)
Sensitivity and specificity did not differ significantly between screening with pre- and post-ductal measurements versus post-ductal measurements alone.(38) Although post-ductal screening alone is easier and quicker, it may miss conditions such as transposition of great arteries with reverse differential cyanosis. It is well established that left heart obstructive lesions are most commonly missed, with or without pulse oximetry screening. The addition of perfusion index measurement may improve the sensitivity of pulse oximetry screening for these lesions.(43)
Pulse oximetry screening was implemented at KKH in June 2014 (
Fig. 1
Pulse oximetry screening algorithm at KK Women’s and Children’s Hospital.

To date, no CCHD has been detected through screening of asymptomatic infants in the well-baby nurseries at KKH, but infants with non-CCHD pathologies have been detected. We postulate that effective prenatal ultrasound screening combined with good postnatal monitoring contributed to the lack of detection of CCHD through pulse oximetry screening. Pulse oximetry is now considered a screening test for general well-being in apparently healthy-looking infants.
In Singapore, pulse oximetry screening has been implemented widely and has become a national programme. Considerations prior to implementation include prenatal detection rates, access to cardiology service and expertise in performing echocardiograms within individual settings. An individualised screening algorithm that strikes a good balance between detecting a serious condition and minimising false positive results is important.
SCREENING FOR ORTHOPAEDIC DISORDERS
The orthopaedic and neonatology departments should work very closely to ensure timely screening of orthopaedic conditions at birth. This will ensure the use of effective early interventions that are relatively noninvasive. The orthopaedic conditions that are screened at birth include DDH, clubfeet and primary muscular torticollis.
Developmental dysplasia of the hips
DDH is one of the common concerns encountered in paediatric orthopaedics. The definition of DDH includes dislocated, dislocatable or dysplastic hips diagnosed by imaging modalities. The cause of DDH remains largely unknown, although an interplay of genetic and ethnic factors has been found. Most developed countries report an incidence of 1.5 to 20 per 1,000 births. The variation is attributable, in part, to differences in diagnostic methods and the timing of evaluation.(44)
Infants with the following features have been considered to be at a higher risk for DDH: first born, female gender, breech presentation, positive family history and conditions associated with ‘packaging disorders’ of the uterus.(44) The observed natural history of DDH includes leg length discrepancy, gait abnormalities, chronic hip pain and early osteoarthritis.(44)
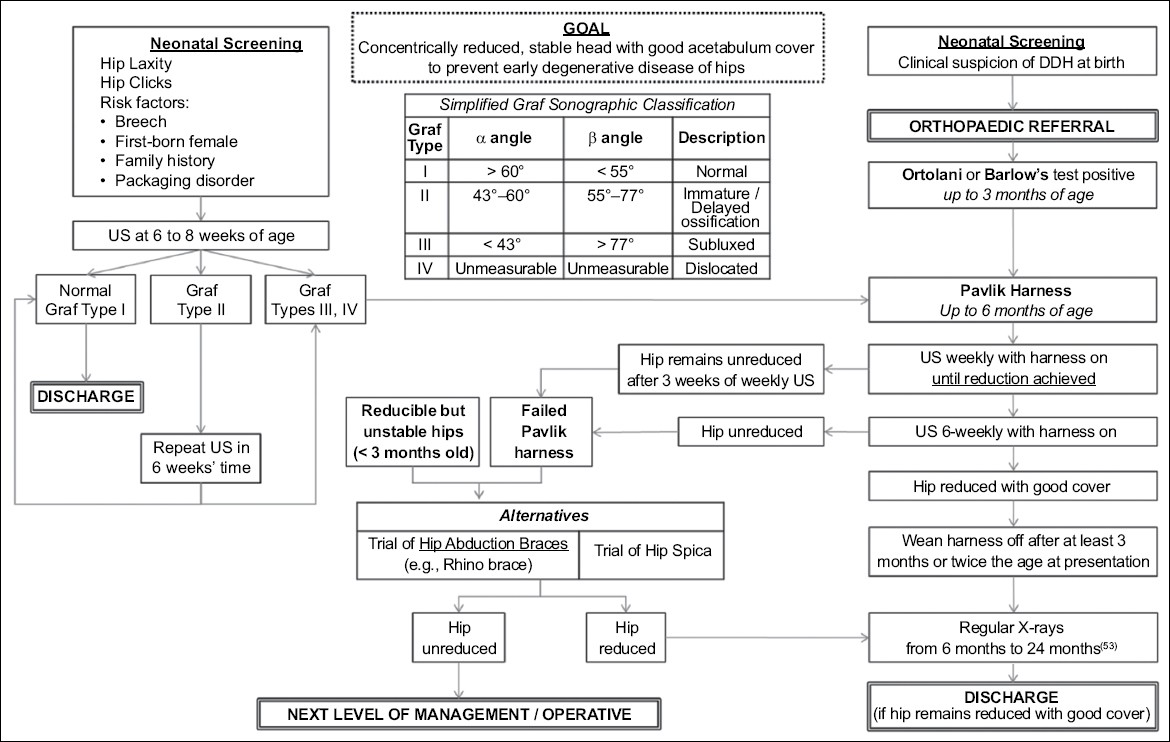
In KKH, selective screening is practiced, in that only infants with a high risk for DDH with normal clinical findings at birth undergo the DDH ultrasound protocol, as described by Graf, at six to eight weeks.(45) All other neonates undergo the routine head-to-toe screening by the neonatologist shortly after birth, and if they are found to be Ortolani- or Barlow-positive, they are referred to the paediatric orthopaedic surgeon while still in the hospital. Once the findings are confirmed, treatment is immediately started with a Pavlik harness, as detailed in the protocol in
Fig. 2
Screening and management protocol for developmental dysplasia of the hips (DDH) at KK Women’s and Children’s Hospital.
Clubfeet
The incidence of congenital talipes equinovarus, commonly known as clubfoot, is estimated at 1–2 per 1,000 live births,(47,48) with variation in its global incidence, according to a 2014 estimate by the Global Clubfoot Initiative.(49) It has a male predominance, with a male-to-female ratio of 2:1.(50) Bilateral involvement is observed in 30%–50% of the cases.(51)
Clubfoot is another common condition that is screened at birth and treated early. This is especially important owing to the very short window of opportunity it presents to ensure good results. Once a structural clubfoot has been confirmed after referral by the screening neonatologist, serial manipulation casting by the Ponseti method(52) is started as early as possible, usually on Day 2 of life. Subsequent weekly casting and manipulation follows until clinical milestones are reached, as spelled out in the protocol. While the details of the protocol are beyond the scope of this article, screening and early intervention are crucial for achieving a success rate of over 95%, i.e. for the feet being fully corrected.
Primary muscular torticollis
While it may not be obvious at birth, early detection and screening of this condition by looking at risk factors such as the ‘packaging disorders’ is important. If this condition is missed at birth, it is mostly picked up at the well-baby clinic at around three months, when the child begins to develop head and neck control.
Early intervention would involve a series of physiotherapist-supervised stretches of the affected sternomastoid muscles. This helps to avoid long-term secondary effects of facial asymmetry, which can be difficult to reverse once the child is older. It has also been shown that physiotherapy is most effective below the age of one year, rendering the screening of this condition all the more important.
FUTURE DIRECTIONS
There is a need to establish a national Newborn Screening Centre in Singapore with full-time dedicated staff to take over the organisation, audit, bench-marking, quality assurance and further development of screening. In future, screening could be made available for some of the other countries in the region, especially Indonesia, Brunei, Vietnam, Myanmar, Laos and Cambodia. Advances in molecular genetics have revealed that markers of degenerative diseases, namely obesity, diabetes mellitus, hypercholesterolaemia, systemic hypertension and ischaemic heart disease are present during the newborn period. The rapid advancement of technology has also made genomic screening on a single blood spot feasible. The potential benefits of such initiatives would be early identification and intervention, which may result in prevention or delay in the presentation of these diseases that have public health concerns in Singapore. However, more research is warranted to determine the sensitivity and specificity of these molecular and genetic markers and their predictive values. Moreover, the social, ethical, insurance and legal issues related to such screening strategies need to be addressed before embarking upon such initiatives.
ACKNOWLEDGEMENTS
We extend our sincere thanks to Ms Karen Hee, Senior Coordinator, Universal Newborn Hearing Screening, KK Women’s and Children’s Hospital for her contribution to this manuscript.