Singapore Med J 2019; 60(5): 247-252 doi: https://doi.org/10.11622/smedj.2019008
Initial experience of laparoscopic right hemicolectomy with complete mesocolic excision in Singapore: a case series
Ming Li Ho1, MBBS, FRCS, Cheryl Chong2, MBBS, MRCS, Shen Ann Yeo3, MBBS, FRCS, Chee Yung Ng4, MBBS, FRCS
Author Information >Copyright and License information >
1Department of Surgery, Sengkang Health, Singapore 2Department of General Surgery, Singapore General Hospital, Singapore 3Department of Colorectal Surgery, Singapore General Hospital, Singapore 4One Surgical Clinic and Surgery, Mount Elizabeth Novena Specialist Centre, Singapore Correspondence: Dr Eugene Yeo Shen Ann, Consultant Surgeon, Department of Colorectal Surgery, Singapore General Hospital, Outram Road, Singapore 169608. eugene.yeo.s.a@singhealth.com.sg
Laparoscopic colorectal surgery is increasingly performed worldwide due to its multiple advantages over traditional open surgery. In the surgical treatment of right-sided colonic tumours, the latest technique is laparoscopic right hemicolectomy with complete mesocolic excision (lapCME), which aims to lower the rate of local recurrence and maximise survival as compared to standard laparoscopic right hemicolectomy (lapS).
METHODS
We conducted a retrospective analysis of our initial experience with lapCME in Singapore General Hospital between 2012 and 2015. All procedures were performed by a single surgeon.
RESULTS
Nine patients underwent lapCME and 16 patients underwent lapS. Indication for lapCME was cancer in the right colon. None of the patients required conversion to open surgery, and all were discharged well. The number of lymph nodes resected in the lapCME group was significantly greater than in the lapS group (29 ± 15 vs. 19 ± 6; p = 0.02) during the study period, and the mean operation time was significantly longer for lapCME (237 ± 50 minutes vs. 156 ± 46 minutes; p = 0.0005). There were no statistically significant differences in terms of demographics, tumour stage, time taken for bowel to open postoperatively, time taken for patient to resume a solid diet postoperatively and length of hospital stay. Two patients who underwent lapS were re-admitted for intra-abdominal collections – one patient required radiology-guided drainage, while the other patient was managed conservatively.
CONCLUSION
Our initial experience with lapCME confirms the feasibility and safety of the procedure.
Keywords: central vascular ligation, colon cancer, complete mesocolic excision, laparoscopic right hemicolectomy
INTRODUCTION
The use of laparoscopic surgery has been increasingly widespread, and more patients are undergoing laparoscopic surgery for the treatment of colorectal cancer. Laparoscopic colorectal surgery has been proven to be more advantageous than open surgery. The benefits include reduced length of stay (LOS) in hospital, earlier return of bowel function, as well as reduced blood loss and pain without any compromise to the quality of oncological resection and nodal yield.(1-4)
In rectal cancer surgery, the concept of total mesorectal resection (TME) that Heald RJ introduced has significantly transformed oncological outcomes.(5-7) The underlying principle is that the rectal tumour is dissected in the plane between the embryologic mesorectal and parietal fascia (also known as the ‘Holy Plane’). This enables tumour resection in a fascial and peritoneal lined envelope that also contains the draining lymphatics, lymph nodes and blood vessels through which the tumour may spread, hence minimising local recurrence rates and improving survival.
Traditionally, the operation of choice for right-sided colonic cancers is a right hemicolectomy. Surgeons who specialise in laparoscopic colorectal surgery typically perform a standard laparoscopic right hemicolectomy (lapS). Using the principles of TME in rectal surgery, this concept was extrapolated to colonic surgery, from which the technique of performing a complete mesocolic excision (CME) with central vascular ligation (CVL) in the resection of colonic tumours was derived. CME with CVL, a technique pioneered by Hohenberger et al,(8) is based on the dissection of the mesocolon along the embryological planes, resulting in resection of colon and mesocolon specimens lined by intact fascial lining containing the tumour and blood vessels, lymphatic vessels and lymph nodes. The idea behind CME is that by resecting the tumour with clear margins and in an intact mesocolic envelope, it will minimise the chance of remnant metastatic tumour being left behind. CME also ensures that lymph node harvest is maximised. Overall, the CME technique seeks to minimise local recurrence and increase survivability.
However, CME for right-sided colonic tumours is known to be particularly demanding technically, as dissection takes place along major mesenteric vessels that have variable anatomy. In this article, we review a case series, comparing patients who had undergone laparoscopic right hemicolectomy with CME (lapCME) with patients who had undergone lapS, with the aim of determining the feasibility and safety of lapCME.
METHODS
The medical records of all consecutive patients with neoplastic lesions in the right colon who underwent laparoscopic right hemicolectomy between 1 January 2012 and 30 September 2015 at the Department of Colorectal Surgery, Singapore General Hospital, were included in this study. All procedures were performed by a single surgeon (Ng CY). This study was approved by our institution’s review board.
Prior to surgery, all the patients had undergone endoscopic evaluation of the lesion, as well as staging with computed tomography of the chest, abdomen and pelvis. Right colonic tumours were defined as all colonic tumours that arose proximal to the splenic flexure. The following were the exclusion criteria: presence of distant irresectable metastasis; synchronous or double primary cancer; cancer related to hereditary syndromes such as familial adenomatous polyposis or hereditary nonpolyposis colorectal cancer; and background of inflammatory bowel disease or any operation performed in an emergency setting.
We retrospectively reviewed patients’ medical records, including demographic data such as age, gender and comorbidities, and surgical factors. The primary endpoints included oncological outcomes, tumour stage, clear margins and lymph node yield. We also investigated clinical outcomes, including duration of operation, time taken for bowels to open postoperatively, time taken to resume a solid diet postoperatively, LOS and postoperative complications. Complications were graded according to the Clavien-Dindo classification system.(9) Pathology results were reported according to the sixth edition of the AJCC (American Joint Committee on Cancer) Cancer Staging Manual.
All statistical analyses were performed using SPSS version 14.0 (SPSS Inc, Chicago, IL, USA). Categorical data, such as gender and tumour stage, was analysed using chi-square test, while numerical data was assessed using the t-test. All statistical tests were assessed at the conventional 0.05 level of significance.
The following is a description of the surgical technique. In lapS, the camera port is placed through a subumbilical midline incision. A total of four 5-mm ports are inserted at the right/left hypochondrium and right/left iliac fossa. An assistant applies traction on the bloodless fold of Treves, which enables the ileocolic vessels to be tented laterally. Next, the ileocolic pedicle is dissected free and ligated either with a laparoscopic linear stapler or an energy device. However, the origin of the ileocolic pedicle from the superior mesenteric artery/superior mesenteric vein (SMA/SMV) is not exposed; ligation of the pedicle is performed intracorporeally at a proximal location determined by the surgeon. After ligation of the ileocolic pedicle, the mesentery is dissected to the second part of the duodenum. From this point, mobilisation proceeds in a medial to lateral direction, and the head of the pancreas is not exposed. If the right colic pedicle is present, it is ligated at the level of the second part of the duodenum. Lateral mobilisation of the bowel is performed from the ileum to the proximal transverse colon to release the remnant attachments of the bowel from the retroperitoneum. The tumour is then exteriorised via a mini-laparotomy wound. After exteriorising the tumour, the right branch of the middle colic pedicle is ligated along with the exteriorised colonic mesentery; its origin to the middle colic pedicle is not dissected free. The tumour is then resected and anastomosis is performed extracorporeally in an antiperistaltic side-to-side fashion using linear staplers.
LapCME is routinely performed by the surgeon in the following manner. A 10-mm camera port is placed through a subumbilical midline incision. This incision is later extended for specimen extraction. Pneumoperitoneum is created and the abdominal cavity is explored with a 30-degree laparoscope. The surgeon operates on the patient’s left side, and 5-mm working ports are inserted as per lapS. The patient is placed in a steep Trendelenburg position and right-side up. Initial dissection is performed inferiorly at the base of the ileal mesentery, with dissection performed between the ileal mesentery and retroperitoneum. The assistant grasps the bloodless fold of Treves at the ileocecal junction to stretch up the mesentery towards the right lower quadrant. An advanced energy device can be used to facilitate dissection.
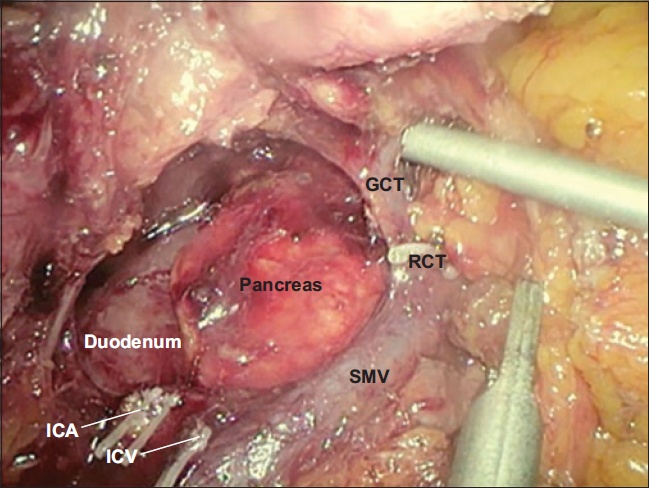
Following that, mesocolic plane dissection proceeds in the cephalad plane until the C loop of the duodenum and pancreatic head is exposed. Fig. 1 shows the visualised structures following an adequate mobilisation of the right colon. Next, a CVL is carried out, beginning with dissection of the ileocolic vessels at their origin; the ileocolic vessels are ligated with 5-mm clips and transected. The CVL proceeds in a cephalad direction to further dissect and ligate the right colic artery (if present) and middle colic pedicles (always present). Traction is then applied inferiorly on the colon and the lesser sac is entered. The right gastroepiploic vein is traced to its confluence with the right colic vein (RCV) and, at this juncture, the surgeon is able to identify the location of the gastrocolic trunk (GCT) of Henle. Just before it joins the right gastroepiploic vein, the RCV is ligated.
Fig. 1
Intraoperative photograph shows the dissected out superior mesenteric vein (SMV) with the ligated ileocolic vein (ICV) and ileocolic artery (ICA). The gastrocolic trunk (GCT) and ligated right colic vein (RCV) are also identified.
Subsequently, the proximal transverse colon is retracted inferomedially. A lateral to medial colonic mobilisation is performed to release the remaining colonic attachments from the retroperitoneum. The right hemicolon and tumour are exteriorised through a midline mini-laparotomy wound; the tumour is then resected and a functional end-to-end ileocolic anastomosis is performed in the usual fashion.
RESULTS
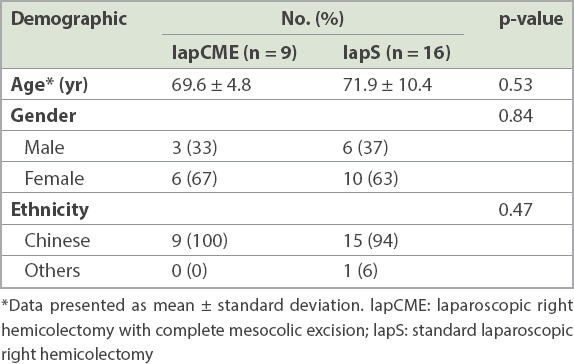
A total of 25 patients formed the basis of this study. Nine patients (three male, six female) underwent lapCME and 16 patients (six male, ten female) underwent lapS. The mean age of patients in the lapCME group and lapS group was 69.6 years and 71.9 years, respectively. Table I shows the demographics of the patient cohort. All the patients had neoplastic lesions involving the right colon. Four patients had previously undergone abdominal surgery – lapCME group: open appendicectomy (n = 1) and open hysterectomy (n = 1); lapS group: laparoscopic cholecystectomy (n = 1) and open right ovarian cystectomy (n = 1).
Table I
Patient demographic in the patient groups (n = 25).
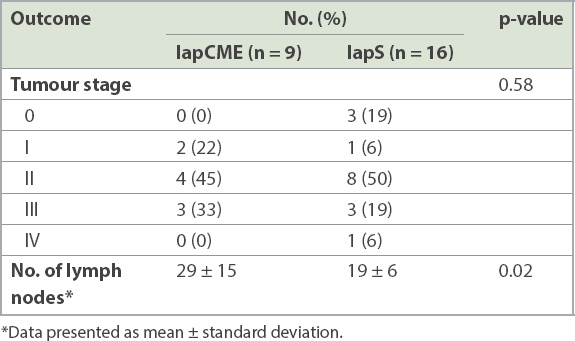
Pathological assessment of the resected specimens of patients who underwent lapCME revealed two patients with Stage I, four with Stage II and three with Stage III disease. One of these patients had Stage II medullary carcinoma, while the rest had adenocarcinoma. In the lapS group, the number of patients with Stage I, II, III and IV disease on histology was one, eight, three and one, respectively. The patient with Stage IV disease was classified as such based on the presence of a solitary liver metastasis; following lapS, this patient underwent adjuvant chemotherapy and subsequent curative liver resection. In the lapS group, there were 3 (19%) patients whose final histology showed non-malignant disease; two patients had tubular adenoma with low-grade dysplasia and one patient had tubulovillous adenoma with high-grade dysplasia). The number of lymph nodes harvested in the lapCME group was significantly higher than in the lapS group (29 ± 15 vs. 19 ± 6; p = 0.02; Table II).
Table II
Histological outcomes of resected specimens.
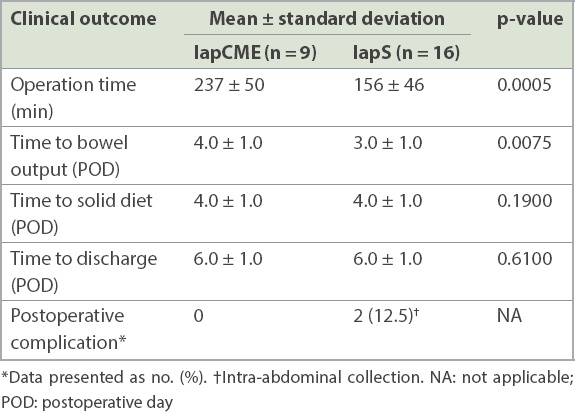
Table III shows the various clinical outcomes of the cohort. Operation time in the lapCME group was significantly longer than in the lapS group (mean 237 ± 50 minutes vs. 156 ± 46 minutes; p = 0.0005). None of the cases required conversion to open surgery. Postoperatively, the mean time for bowels to open was four days for lapCME patients versus three days for lapS patients (p = 0.0075). Both LapCME and lapS patients required an average of four days to resume a solid diet postoperatively and six days of hospital stay before discharge. No major intraoperative complications were encountered in either arm. There were also no mortalities, anastomotic leaks or re-operations. In the lapS group, two patients developed intra-abdominal collections.
Table III
Clinical outcomes of the patients (n = 25).
The first patient was a 69-year-old who presented with anaemia and was subsequently noted to have an ascending colonic mass on colonoscopy. Histology showed foci of high-grade dysplasia. The patient underwent an uneventful lapS and was discharged home on postoperative day (POD) 4. On POD 34, the patient was re-admitted from the clinic after complaining of right-sided abdominal pain. Physical examination showed tenderness in the upper right abdomen. Inflammatory markers were elevated. Computed tomography of the abdomen and pelvis (CTAP) showed a 4.7-cm fluid collection in the subhepatic space with no free intraperitoneal air present. The patient underwent radiological percutaneous drainage of the intra-abdominal collection where 30 mL of pus was drained, and received intravenous antibiotics for seven days. The patient recovered uneventfully and was subsequently discharged well.
The second patient was a 63-year-old who was diagnosed with adenocarcinoma of the ascending colon, for which an lapS was performed. The operation was uneventful. The patient was discharged well on POD 4, but was re-admitted on POD 30 for right flank pain. Subsequent CTAP showed a 2.0-cm fluid collection adjacent to the ileocolic anastomosis with no free air present on imaging. The patient was managed conservatively with antibiotics, and the pain resolved. The patient was subsequently discharged well.
DISCUSSION
The basic tenet in the curative surgical treatment of colorectal cancer is resection of the primary tumour along with its accompanying blood supply, lymphatics and lymph nodes with an adequate bowel resection margin. Over the last 20 years, the focus of advancement in colorectal cancer surgery was mainly the management of rectal carcinoma with standardisation of surgical approaches and techniques. As a result, local recurrence and overall survival in rectal cancer have improved greatly. Studies have shown that standardisation in surgical techniques reduces rates of local recurrence and improves surgical outcomes.(10-14) However, it has also been observed that the survival rates for colon cancer have only improved modestly in the last two decades. In fact, some studies have reported that disease-free survival rates for rectal cancer have surpassed those for colon cancer.(15,16)
The central idea behind TME is that with meticulous dissection, rectal resection can be performed with a preserved mesorectal fascia. CME follows a similar concept. During CME, sharp dissection is performed in the potential space (also known as Toldt’s space) between the mesenteric plane and parietal plane of the retroperitoneum. This results in the removal of the mesentery within a complete envelope of mesenteric fascia and visceral peritoneum, which contains all lymph nodes draining the tumour. Next, a CVL is performed to completely remove all lymph nodes along the draining vessels and, finally, resection of an adequate length of bowel is performed to remove the involved pericolic lymph nodes. In CME of right-sided colonic tumours, mobilisation of the mesocolon is more radical than in a standard resection. By exposing the head of the pancreas and the anterior surfaces of the SMV/SMA, the origins of the ileocolic and middle colic pedicles are dissected out, thus allowing ligation of the tumour’s feeding vessels to be performed at the origin. During a ‘standard’ right hemicolectomy, the pedicle is usually ligated at a proximal location that is convenient to the surgeon.
CME holds several benefits over standard surgery. Hohenberger et al,(8) who pioneered CME in the West, showed that the technique yields excellent disease-specific survival and low local recurrence rates. Their series compared 1,329 patients who underwent colonic resections for cancer over three time periods. In the third and latest time period, surgery was carried out in their unit using a standardised CME technique; the recurrence rate was found to have dropped from 6.5% to 3.6%, while the five-year cancer-related survival rate improved from 82.1% to 89.1%. The study further demonstrated that a lymph node count > 28 was significantly associated with improved survival in patients with node-negative disease. An Australian study conducted by Bokey et al(17) had used a similar study design that compared patients over two time periods, with the latter period corresponding to the time where the institution started performing CME and CVL; marked improvements were seen in the five-year overall survival from 48% to 63% and disease-specific survival from 66% to 76%.
In Asia, particularly Korea and Japan, many colorectal units that have performed colonic surgery by adopting the concept of D3 lymphadenectomy, which has very similar principles to CME and CVL, have reported remarkable results.(18-20) Advocates of CME argue that it results in a higher nodal yield compared to standard surgery, thus leading to improved accuracy of staging and greater survival benefits.(21-24) In a large case series specific to right hemicolectomies, West et al reported a greater average nodal yield of 31.3 nodes for CME, as compared to that of 20 nodes for conventional right hemicolectomy.(24) Similarly in our case series, we demonstrated a significantly greater number of lymph nodes harvested using lapCME compared to lapS. Additionally, as skip metastases to apical nodes occur in 0.8%–2.0% of cases,(22,25) it has been proposed that adherence to CME/CVL techniques ensures that apical skip lesions are removed in the event that they occur.(26-28)
CME can be successfully performed via laparoscopic surgery with comparable oncological outcomes.(29-31) In a randomised trial comparing laparoscopic and open CME, Yamamoto et al(32) reported improved short-term outcomes, including lower complication rates and shorter LOS in the laparoscopic group.
Recent studies comparing standard laparoscopic versus open right hemicolectomy have reported an LOS of 6–13 days.(33-37) In our study, the average LOS for both the lapCME and lapS groups was six days, which is on the lower end of the spectrum reported in the current literature. This suggests that lapCME patients can still benefit from a short LOS despite having undergone a more extensive surgical procedure.
It is well recognised that CME is a technically challenging procedure with much of the dissection occurring in close proximity to major vessels such as the SMV and middle colic artery. The difficulty of the procedure is further increased when done laparoscopically. Recent studies comparing standard laparoscopic versus open right hemicolectomy showed that the average duration of operation for the former was 107–207 minutes.(33-37) Likewise, this was reflected in our study; while the time of lapS was in keeping with those reported in the current literature, the average time taken to perform lapCME was significantly longer at 237 minutes. Our data also showed that lapCME patients took a significantly longer time (four vs. three days) to have their first bowel movement after surgery. This is possibly due to the increased duration of operation for lapCME, and more dissection around the duodenum and pancreas. However, we found no difference in the time taken for patients to resume a solid diet postoperatively.
Questions have been raised about the significant risk of postoperative complications following CME. Recent studies have shown that CME carries a postoperative morbidity rate of 5.7%–19.7%.(38,39) Some studies have also reported that CME is associated with more intraoperative organ injuries and severe complications compared to standard surgery.(40,41) Of note, there is a significant risk of injury to the SMV during CME right hemicolectomy, especially when dissecting around the pancreas, due to the anatomic complexity and vascular variations.(42)
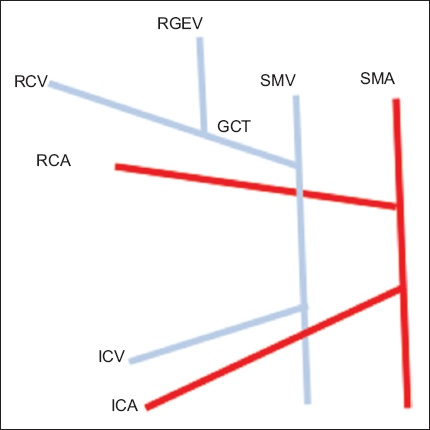
The ileocolic vein is a vessel that is always present and drains into the SMV. However, there are numerous vascular anatomical variations involving the RCV, accessory RCV (if present), middle colic vein and GCT. One common variant is when the GCT is a single trunk with the right gastroepiploic vein and RCV both draining into the GCT. In terms of arterial anatomy, the ileocolic artery passes anteriorly to the SMV 50% of the time and posteriorly to the SMV. Likewise, the right colic artery (if present), passes anteriorly to the SMV 50% of the time after branching out from the SMA. Due to these variations, lapCME is made much more challenging, as each branch needs to be identified with certainty prior to ligation. Fig. 2 shows an illustration of one of the more common variants of the vascular anatomy. Inadvertent injury to major mesenteric vessels could lead to significant postoperative morbidity and mortality. Fortunately, most of our patients recovered uneventfully after lapCME, and our surgical team did not encounter any major intraoperative complications. Furthermore, none of our patients developed anastomotic leak or required re-operation.
Fig. 2
Illustration shows a common variant in vascular anatomy. GCT: gastrocolic trunk; ICA: ileocolic artery; ICV: ileocolic vein; RCA: right colic artery; RCV: right colic vein; RGEV: right gastroepiploic vein; SMA: superior mesenteric artery; SMV: superior mesenteric vein
Opponents of CME also argue that there are too many confounders in the current literature to make any definite conclusions regarding the oncological benefits of CME – the most prominent confounder being the effect conferred by standardised adjuvant chemotherapy regimes, which plays a significant role in the satisfactory results achieved by many CME surgeons. We recognise that, apart from the small sample size, the retrospective design of this study made it prone to bias. However, the single-surgeon design of our study served to overcome the surgical-related confounders.
In summary, the present study is one of the first in the region to examine the use of laparoscopic CME in right hemicolectomy. We have shown that lapCME can be safely performed with satisfactory results, and minimal complications and postoperative sequalae. Due to its low morbidity, we opine that extended lymphadenectomy is only beneficial for patients undergoing oncological surgery. We hope that this initial data will serve as a foundation for more research on this topic in the future.
References Fleshman J, Sargent DJ, Green E, et al. Clinical Outcomes of Surgical Therapy Study GroupLaparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial.Ann Surg. 2007;246:655-64. Jayne DG, Guillou PJ, Thorpe H, et al. UK MRC CLASICC Trial GroupRandomized trial of laparoscopic-assisted resection of colorectal carcinoma:3-year results of the UK MRC CLASICC Trial Group.J Clin Oncol. 2007;25:3061-8. Guillou PJ, Quirke P, Thorpe H, et al. UK MRC CLASICC Trial GroupShort-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial):multicentre, randomised controlled trial.Lancet. 2005;365:1718-26. Lacy AM, García-Valdecasas JC, Delgado S, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer:a randomised trial.Lancet. 2002;359:2224-9. Heald RJ, Husband EM, Ryall RD.The mesorectum in rectal cancer surgery--the clue to pelvic recurrence?.Br J Surg. 1982;69:613-6. Heald RJ, Ryall RD.Recurrence and survival after total mesorectal excision for rectal cancer.Lancet. 1986;1:1479-82. MacFarlane JK, Ryall RD, Heald RJ.Mesorectal excision for rectal cancer.Lancet. 1993;341:457-60. Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S.Standardized surgery for colonic cancer:complete mesocolic excision and central ligation--technical notes and outcome.Colorectal Dis. 2009;11:354-65. Dindo D, Demartines N, Clavien PA.Classification of surgical complications:a new proposal with evaluation in a cohort of 6,336 patients and results of a survey.Ann Surg. 2004;240:205-13. Pramateftakis MG.Optimizing colonic cancer surgery:high ligation and complete mesocolic excision dang right hemicolectomy.Tech Coloproctol. 2010;14:Suppl 1S49-51. Kobayashi H, Enomoto M, Higuchi T, et al. Clinical significance of lymph node ratio and location of nodal involvement in patients with right colon cancer.Dig Surg. 2011;28:190-7. Martling AL, Holm T, Rutqvist LE, et al. Effect of a surgical training programme on outcome of rectal cancer in the County of Stockholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project.Lancet. 2000;356:93-6. Kapiteijn E, Putter H, van de Velde CJ.Cooperative investigators of the Dutch ColoRectal Cancer GroupImpact of the introduction and training of total mesorectal excision on recurrence and survival in rectal cancer in The Netherlands.Br J Surg. 2002;89:1142-9. Wibe A, Møller B, Norstein J, et al. Norwegian Rectal Cancer GroupA national strategic change in treatment policy for rectal cancer--implementation of total mesorectal excision as routine treatment in Norway. A national audit.Dis Colon Rectum. 2002;45:857-66. Birgisson H, Talbäck M, Gunnarsson U, Påhlman L, Glimelius B.Improved survival in cancer of the colon and rectum in Sweden.Eur J Surg Oncol. 2005;31:845-53. Iversen LH, Nørgaard M, Jepsen P, et al. Northern Danish Cancer Quality Assessment GroupTrends in colorectal cancer survival in northern Denmark 1985-2004.Colorectal Dis. 2007;9:210-7. Bokey EL, Chapuis PH, Dent OF, et al. Surgical technique and survival in patients having a curative resection for colon cancer.Dis Colon Rectum. 2003;46:860-6. Watanabe T, Itabashi M, Shimada Y, et al. Japanese Society for Cancer of the Colon and RectumJapanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2010 for the treatment of colorectal cancer.Int J Clin Oncol. 2012;17:1-29. West NP, Kobayashi H, Takahashi K, et al. Understanding optimal colonic cancer surgery:comparison of Japanese D3 resection and European complete mesocolic excision with central vascular ligation.J Clin Oncol. 2012;30:1763-9. Shin JW, Amar AH, Kim SH, et al. Complete mesocolic excision with D3 lymph node dissection in laparoscopic colectomy for stages II and III colon cancer:long-term oncologic outcomes in 168 patients.Tech Coloproctol. 2014;18:795-803. Chang GJ, Rodriguez-Bigas MA, Skibber JM, Moyer VA.Lymph node evaluation and survival after curative resection of colon cancer:systematic review.J Natl Cancer Inst. 2007;99:433-41. Chen SL, Bilchik AJ.More extensive nodal dissection improves survival for stages I to III of colon cancer:a population-based study.Ann Surg. 2006;244:602-10. Kessler H, Hohenberger W.Extended lymphadenectomy in colon cancer is crucial.World J Surg. 2013;37:1789-98. West NP, Hohenberger W, Weber K, et al. Complete mesocolic excision with central vascular ligation produces an oncologically superior specimen compared with standard surgery for carcinoma of the colon.J Clin Oncol. 2010;28:272-8. Merrie AE, Phillips LV, Yun K, McCall JL.Skip metastases in colon cancer:assessment by lymph node mapping using molecular detection.Surgery. 2001;129:684-91. Tan KY, Kawamura YJ, Mizokami K, et al. Distribution of the first metastatic lymph node in colon cancer and its clinical significance.Colorectal Dis. 2010;12:44-7. Liang JT, Huang KC, Lai HS, Lee PH, Sun CT.Oncologic results of laparoscopic D3 lymphadenectomy for male sigmoid and upper rectal cancer with clinically positive lymph nodes.Ann Surg Oncol. 2007;14:1980-90. Liang JT, Lai HS, Huang J, Sun CT.Long-term oncologic results of laparoscopic D3 lymphadenectomy with complete mesocolic excision for right-sided colon cancer with clinically positive lymph nodes.Surg Endosc. 2015;29:2394-401. Toyota S, Ohta H, Anazawa S.Rationale for extent of lymph node dissection for right colon cancer.Dis Colon Rectum. 1995;38:705-11. Storli KE, Søndenaa K, Furnes B, Eide GE.Outcome after introduction of complete mesocolic excision for colon cancer is similar for open and laparoscopic surgical treatments.Dig Surg. 2013;30:317-27. Han DP, Lu AG, Feng H, et al. Long-term outcome of laparoscopic-assisted right-hemicolectomy with D3 lymphadenectomy versus open surgery for colon carcinoma.Surg Today. 2014;44:868-74. Yamamoto S, Inomata M, Katayama H, et al. Japanese Clinical Oncology Group Colorectal Cancer Study GroupShort-term surgical outcomes from a randomized controlled trial to evaluate laparoscopic and open D3 dissection for stage II/III colon cancer. Japan Clinical Oncology Group Study JCOG0404.Ann Surg. 2014;260:23-30. Baker RP, Titu LV, Hartley JE, Lee PW, Monson JR.A case-control study of laparoscopic right hemicolectomy vs. open right hemicolectomy.Dis Colon Rectum. 2004;47:1675-9. Ng SS, Lee JF, Yiu RY, et al. Emergency laparoscopic-assisted versus open right hemicolectomy for obstructing right-sided colonic carcinoma:a comparative study of short-term clinical outcomes.World J Surg. 2008;32:454-8. Zheng MH, Feng B, Lu AG, et al. Laparoscopic versus open right hemicolectomy with curative intent for colon carcinoma.World J Gastroenterol. 2005;11:323-6. Tong DK, Law WL.Laparoscopic versus open right hemicolectomy for carcinoma of the colon.JSLS. 2007;11:76-80. Braga M, Frasson M, Vignali A, Zuliani W, Di Carlo V.Open right colectomy is still effective compared to laparoscopy:results of a randomized trial.Ann Surg. 2007;246:1010-5. Cho MS, Baek SJ, Hur H, et al. Modified complete mesocolic excision with central vascular ligation for the treatment of right-sided colon cancer:long-term outcomes and prognostic factors.Ann Surg. 2015;261:708-15. Adamina M, Manwaring ML, Park KJ, Delaney CP.Laparoscopic complete mesocolic excision for right colon cancer.Surg Endosc. 2012;26:2976-80. Feng B, Sun J, Ling TL, et al. Laparoscopic complete mesocolic excision (CME) with medial access for right-hemi colon cancer:feasibility and technical strategies.Surg Endosc. 2012;26:3669-75. Bertelsen CA, Neuenschwander AU, Jansen JE, et al. Copenhagen Complete Mesocolic Excision Study (COMES);Danish Colorectal Cancer Group (DCCG)Short-term outcomes after complete mesocolic excision compared with 'conventional'colonic cancer surgery.Br J Surg. 2016;103:581-9. Lee SJ, Park SC, Kim MJ, Sohn DK, Oh JH.Vascular anatomy in laparoscopic colectomy for right colon cancer.Dis Colon Rectum. 2016;59:718-24.
REFERENCES:
1. Fleshman J, Sargent DJ, Green E, et al; Clinical Outcomes of Surgical Therapy Study Group. Laparoscopic colectomy for cancer is not inferior to open surgery based on 5-year data from the COST Study Group trial. Ann Surg 2007; 246:655‑64. https://doi.org/10.1097/SLA.0b013e318155a762
PMid:17893502
2. Jayne DG, Guillou PJ, Thorpe H, et al; UK MRC CLASICC Trial Group. Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J Clin Oncol 2007; 25:3061‑8. https://doi.org/10.1200/JCO.2006.09.7758
PMid:17634484
3. Guillou PJ, Quirke P, Thorpe H, et al; UK MRC CLASICC Trial Group. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet 2005; 365:1718-26. https://doi.org/10.1016/S0140-6736(05)66545-2
4. Lacy AM, García-Valdecasas JC, Delgado S, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 2002; 359:2224-9. https://doi.org/10.1016/S0140-6736(02)09290-5
5. Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery--the clue to pelvic recurrence? Br J Surg 1982; 69:613-6. https://doi.org/10.1002/bjs.1800691019
PMid:6751457
8. Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S. Standardized surgery for colonic cancer: complete mesocolic excision and central ligation--technical notes and outcome. Colorectal Dis 2009; 11:354-65. https://doi.org/10.1111/j.1463-1318.2008.01735.x
PMid:19016817
9. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6,336 patients and results of a survey. Ann Surg 2004; 240:205-13. https://doi.org/10.1097/01.sla.0000133083.54934.ae
PMid:15273542 PMCid:PMC1360123
10. Pramateftakis MG. Optimizing colonic cancer surgery: high ligation and complete mesocolic excision during right hemicolectomy. Tech Coloproctol 2010; 14 Suppl 1:S49-51. https://doi.org/10.1007/s10151-010-0609-9
PMid:20697925
11. Kobayashi H, Enomoto M, Higuchi T, et al. Clinical significance of lymph node ratio and location of nodal involvement in patients with right colon cancer. Dig Surg 2011; 28:190-7. https://doi.org/10.1159/000323966
PMid:21555889
12. Martling AL, Holm T, Rutqvist LE, et al. Effect of a surgical training programme on outcome of rectal cancer in the County of Stockholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project. Lancet 2000; 356:93-6. https://doi.org/10.1016/S0140-6736(00)02469-7
13. Kapiteijn E, Putter H, van de Velde CJ; Cooperative investigators of the Dutch ColoRectal Cancer Group. Impact of the introduction and training of total mesorectal excision on recurrence and survival in rectal cancer in The Netherlands. Br J Surg 2002; 89:1142-9. https://doi.org/10.1046/j.1365-2168.2002.02196.x
PMid:12190680
14. Wibe A, Møller B, Norstein J, et al; Norwegian Rectal Cancer Group. A national strategic change in treatment policy for rectal cancer--implementation of total mesorectal excision as routine treatment in Norway. A national audit. Dis Colon Rectum 2002; 45:857-66. https://doi.org/10.1007/s10350-004-6317-7
PMid:12130870
15. Birgisson H, Talbäck M, Gunnarsson U, Påhlman L, Glimelius B. Improved survival in cancer of the colon and rectum in Sweden. Eur J Surg Oncol 2005; 31:845-53. https://doi.org/10.1016/j.ejso.2005.05.002
PMid:15979269
16. Iversen LH, Nørgaard M, Jepsen P, et al; Northern Danish Cancer Quality Assessment Group. Trends in colorectal cancer survival in northern Denmark: 1985-2004. Colorectal Dis 2007; 9:210-7. https://doi.org/10.1111/j.1463-1318.2006.01130.x
PMid:17298618
17. Bokey EL, Chapuis PH, Dent OF, et al. Surgical technique and survival in patients having a curative resection for colon cancer. Dis Colon Rectum 2003; 46:860-6. https://doi.org/10.1007/s10350-004-6673-3
PMid:12847357
18. Watanabe T, Itabashi M, Shimada Y, et al; Japanese Society for Cancer of the Colon and Rectum. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2010 for the treatment of colorectal cancer. Int J Clin Oncol 2012; 17:1-29. https://doi.org/10.1007/s10147-011-0315-2
PMid:22002491
19. West NP, Kobayashi H, Takahashi K, et al. Understanding optimal colonic cancer surgery: comparison of Japanese D3 resection and European complete mesocolic excision with central vascular ligation. J Clin Oncol 2012; 30:1763-9. https://doi.org/10.1200/JCO.2011.38.3992
PMid:22473170
20. Shin JW, Amar AH, Kim SH, et al. Complete mesocolic excision with D3 lymph node dissection in laparoscopic colectomy for stages II and III colon cancer: long-term oncologic outcomes in 168 patients. Tech Coloproctol 2014; 18:795‑803. https://doi.org/10.1007/s10151-014-1134-z
PMid:24633427
21. Chang GJ, Rodriguez-Bigas MA, Skibber JM, Moyer VA. Lymph node evaluation and survival after curative resection of colon cancer: systematic review. J Natl Cancer Inst 2007; 99:433-41. https://doi.org/10.1093/jnci/djk092
PMid:17374833
22. Chen SL, Bilchik AJ. More extensive nodal dissection improves survival for stages I to III of colon cancer: a population-based study. Ann Surg 2006; 244:602-10.
23. Kessler H, Hohenberger W. Extended lymphadenectomy in colon cancer is crucial. World J Surg 2013; 37:1789-98. https://doi.org/10.1007/s00268-013-2130-6
PMid:23754141
24. West NP, Hohenberger W, Weber K, et al. Complete mesocolic excision with central vascular ligation produces an oncologically superior specimen compared with standard surgery for carcinoma of the colon. J Clin Oncol 2010; 28:272-8. https://doi.org/10.1200/JCO.2009.24.1448
PMid:19949013
25. Merrie AE, Phillips LV, Yun K, McCall JL. Skip metastases in colon cancer: assessment by lymph node mapping using molecular detection. Surgery 2001; 129:684-91. https://doi.org/10.1067/msy.2001.113887
PMid:11391366
26. Tan KY, Kawamura YJ, Mizokami K, et al. Distribution of the first metastatic lymph node in colon cancer and its clinical significance. Colorectal Dis 2010; 12:44-7. https://doi.org/10.1111/j.1463-1318.2009.01924.x
PMid:19438890
27. Liang JT, Huang KC, Lai HS, Lee PH, Sun CT. Oncologic results of laparoscopic D3 lymphadenectomy for male sigmoid and upper rectal cancer with clinically positive lymph nodes. Ann Surg Oncol 2007; 14:1980-90. https://doi.org/10.1245/s10434-007-9368-x
PMid:17458586
28. Liang JT, Lai HS, Huang J, Sun CT. Long-term oncologic results of laparoscopic D3 lymphadenectomy with complete mesocolic excision for right-sided colon cancer with clinically positive lymph nodes. Surg Endosc 2015; 29:2394-401. https://doi.org/10.1007/s00464-014-3940-9
PMid:25384361
29. Toyota S, Ohta H, Anazawa S. Rationale for extent of lymph node dissection for right colon cancer. Dis Colon Rectum 1995; 38:705-11. https://doi.org/10.1007/BF02048026
PMid:7607029
30. Storli KE, Søndenaa K, Furnes B, Eide GE. Outcome after introduction of complete mesocolic excision for colon cancer is similar for open and laparoscopic surgical treatments. Dig Surg 2013; 30:317-27. https://doi.org/10.1159/000354580
PMid:24022524
31. Han DP, Lu AG, Feng H, et al. Long-term outcome of laparoscopic-assisted right-hemicolectomy with D3 lymphadenectomy versus open surgery for colon carcinoma. Surg Today 2014; 44:868-74. https://doi.org/10.1007/s00595-013-0697-z
PMid:23989942
32. Yamamoto S, Inomata M, Katayama H, et al; Japanese Clinical Oncology Group Colorectal Cancer Study Group. Short-term surgical outcomes from a randomized controlled trial to evaluate laparoscopic and open D3 dissection for stage II/III colon cancer: Japan Clinical Oncology Group Study JCOG 0404. Ann Surg 2014; 260:23-30. https://doi.org/10.1097/SLA.0000000000000499
PMid:24509190
33. Baker RP, Titu LV, Hartley JE, Lee PW, Monson JR. A case-control study of laparoscopic right hemicolectomy vs. open right hemicolectomy. Dis Colon Rectum 2004; 47:1675-9. https://doi.org/10.1007/s10350-004-0655-3
PMid:15540298
34. Ng SS, Lee JF, Yiu RY, et al. Emergency laparoscopic-assisted versus open right hemicolectomy for obstructing right-sided colonic carcinoma: a comparative study of short-term clinical outcomes. World J Surg 2008; 32:454-8. https://doi.org/10.1007/s00268-007-9400-0
PMid:18196317
35. Zheng MH, Feng B, Lu AG, et al. Laparoscopic versus open right hemicolectomy with curative intent for colon carcinoma. World J Gastroenterol 2005; 11:323-6. https://doi.org/10.3748/wjg.v11.i3.323
PMid:15637736 PMCid:PMC4205329
36. Tong DK, Law WL. Laparoscopic versus open right hemicolectomy for carcinoma of the colon. JSLS 2007; 11:76-80.
37. Braga M, Frasson M, Vignali A, Zuliani W, Di Carlo V. Open right colectomy is still effective compared to laparoscopy: results of a randomized trial. Ann Surg 2007; 246:1010-5. https://doi.org/10.1097/SLA.0b013e31815c4065
PMid:18043103
38. Cho MS, Baek SJ, Hur H, et al. Modified complete mesocolic excision with central vascular ligation for the treatment of right-sided colon cancer: long-term outcomes and prognostic factors. Ann Surg 2015; 261:708-15. https://doi.org/10.1097/SLA.0000000000000831
PMid:25072438
39. Adamina M, Manwaring ML, Park KJ, Delaney CP. Laparoscopic complete mesocolic excision for right colon cancer. Surg Endosc 2012; 26:2976-80. https://doi.org/10.1007/s00464-012-2294-4
PMid:22549374
40. Feng B, Sun J, Ling TL, et al. Laparoscopic complete mesocolic excision (CME) with medial access for right-hemi colon cancer: feasibility and technical strategies. Surg Endosc 2012; 26:3669-75. https://doi.org/10.1007/s00464-012-2435-9
PMid:22733200
41. Bertelsen CA, Neuenschwander AU, Jansen JE, et al; Copenhagen Complete Mesocolic Excision Study (COMES); Danish Colorectal Cancer Group (DCCG). Short-term outcomes after complete mesocolic excision compared with 'conventional' colonic cancer surgery. Br J Surg 2016; 103:581-9. https://doi.org/10.1002/bjs.10083
PMid:26780563
42. Lee SJ, Park SC, Kim MJ, Sohn DK, Oh JH. Vascular anatomy in laparoscopic colectomy for right colon cancer. Dis Colon Rectum 2016; 59:718-24 https://doi.org/10.1097/DCR.0000000000000636
PMid:27384089