

Abstract
INTRODUCTION
In view of the important role of the environment in improving population health, implementation of health promotion programmes is recommended in living and working environments. Assessing the prevalence of such community health-promoting practices is important to identify gaps and make continuous and tangible improvements to health-promoting environments. We aimed to evaluate the inter-rater reliability of a composite scorecard used to assess the prevalence of community health-promoting practices in Singapore.
METHODS
Inter-rater reliability for the use of the composite health promotion scorecards was evaluated in eight residential zones in the western region of Singapore. The assessment involved three raters, and each zone was evaluated by two raters. Health-promoting practices in residential zones were assessed based on 44 measurable elements under five domains – community support and resources, healthy behaviours, chronic conditions, mental health and common medical emergencies – in the composite scorecard using weighted kappa. The strength of agreement was determined based on Landis and Koch’s classification method.
RESULTS
A high degree of agreement (almost perfect-to-perfect) was observed between both raters for the measurable elements from most domains and subdomains. An exception was observed for the community support and resources domain, where there was a lower degree of agreement between the raters for a few elements.
CONCLUSION
The composite scorecard demonstrated a high degree of reliability and yielded similar scores for the same residential zone, even when used by different raters.
INTRODUCTION
A health-promoting environment is made up of health-promoting programmes, policies, practices and aspects of the built-up environment.(1,2) Its role in preventing chronic diseases and improving the health of the population has been supported by substantial evidence in the existing literature.(3-5) For example, health promotion programmes implemented in workplaces are associated with positive outcomes, such as reduced absenteeism and increased work ability in workers.(6,7) In addition, it has demonstrated positive financial outcomes, such as low medical and absenteeism costs, and substantial cost savings.(8,9) In view of these benefits, implementation of health promotion programmes ought to be recommended in living and working environments.
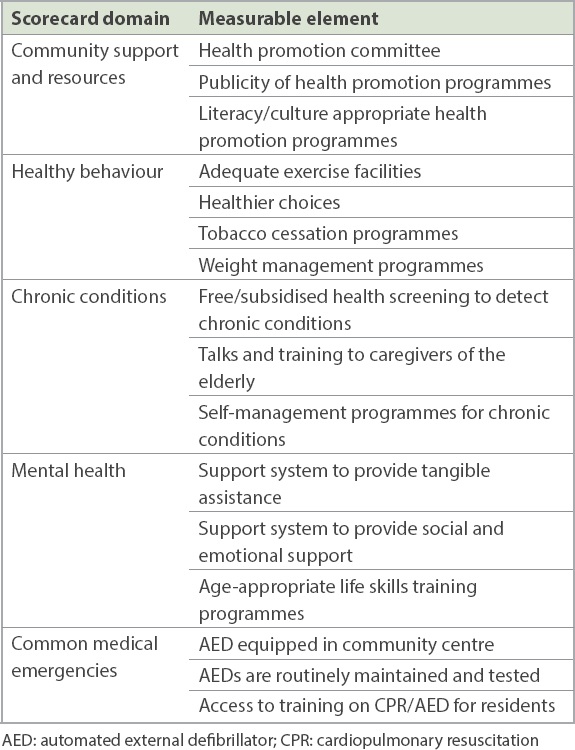
Composite scores could be used as a standardised method to evaluate health promotion programmes and ensure that they are comprehensive and evidence based. The CDC (Centers for Disease Control and Prevention) Worksite Health ScoreCard (HSC) is used to assess employers’ health promotion practices in workplaces in the United States.(10) In Singapore, we developed a similar composite health promotion scorecard after consulting experts from the Saw Swee Hock School of Public Health, National University of Singapore, and the Health Promotion Board to assess the prevalence of health-promoting practices in residential zones. The scorecard consisted of 44 measurable elements that were associated with positive lifestyle and health behaviour changes identified from a comprehensive review of the existing literature. These measurable elements were grouped under five domains: community support and resources; healthy behaviour; chronic conditions; mental health; and common medical emergencies. Each element was assigned a weightage based on the strength of evidence and its impact. Some examples of the measurable elements under each of the five domains of the composite scorecard are listed individually in
Table I
Examples of measurable elements grouped under five domains of the composite health promotion scorecard.
Being an aggregate measure of multiple performance indicators using a predetermined weighting methodology,(12) composite scores are subject to measurement errors. Similar to new instruments of health measurement scales, newly developed composite scores ought to be validated before their formal use. The HSC is a validated tool – its face validity and inter-rater reliability were investigated(13) before it was used to evaluate health promotion programmes in workplaces. Similarly, the composite health promotion scorecard developed in Singapore should be validated before its usage in residential communities. As its face validity had been determined by experts during the development phase,(11) we explored the reliability issue due to the involvement of different assessors when using the composite scorecard. We aimed to evaluate the inter-rater reliability of this composite scorecard for assessing the health-promoting environment in residential communities.
METHODS
The composite health promotion scorecard was developed through a number of processes, such as a review of health promotion literature to identify elements, including interventions, pertinent to changing individual lifestyle and health behaviour. This list was further reviewed to select elements that were relevant to a residential community. Additionally, national health promotion guidelines were incorporated to suit the local context.(11)
The inter-rater reliability of the composite scorecard was assessed in eight residential zones in the western region of Singapore. These zones were community subdivisions of two different electoral constituencies. Guidelines were developed to assist in and bring consistency to its scoring. Each measurable element was scored as ‘fully met’, ‘partially met’ or ‘not met’ based on whether the zone met the criteria specified in the guidelines. The score for each element under a domain was then added to obtain the domain score for the residential zone. The overall score for the residential zone was a total of the various domain scores.(11)
A total of three raters were involved in the assessment. For each zone, two raters took turns to conduct site visits and interview grassroots leaders and committee members of the zone. Discussions with grassroots leaders and observations made during site visits were documented separately by these raters. The raters then used the composite scorecard and scoring guidelines to appraise the health-promoting environments and score the residential zones independently.
The scoring of each residential zone was done by two raters. These raters were medical graduates with a Master’s degree in public health and a minimum of two years’ working experience in hospital epidemiology.(11) Raters were trained by an experienced senior public health consultant who developed the scoring methodology based on international hospital quality accreditation standards.
The training session spanned a total of three hours and included the following: (a) general overview and discussion on the scoring methodology/guidelines for the scoring system; (b) item-by-item review of the measurable elements of the composite health promotion scoring system to train staff in the intent, assessment process and scoring of individual elements; (c) completion of a practice assessment on a hypothetical scenario; and (d) group discussion of the practice assessments to resolve any areas of confusion. Any queries regarding the measurable elements and scoring guidelines were clarified by the trainer.
Inter-rater reliability was assessed for every measurable element scored by both raters in the composite scorecard using weighted kappa, with a range of 0 (no agreement) to 1 (perfect agreement). Weighted kappa was used instead of Cohen’s kappa (unweighted kappa), as the former takes the ordered nature of the weightage values into account. In contrast, Cohen’s kappa assumes the degree of disagreement between two raters to be the same for all pairs of weightage values. For example, using Cohen’s kappa, [1,2] and [1,3] weighted score pairs would be viewed to have the same degree of disagreement. However, weighted kappa would take into account that the degree of disagreement would be larger for the [1,3] weighted score pair than the [1,2] weighted score pair. Hence, weighted kappa is able to perceive a difference in the degree of disagreement between the raters.
The strength of agreement between Raters 1 and 2 was determined using Landis and Koch’s classification method: slight (≤ 0.20); fair (range 0.21–0.40); moderate (range 0.41–0.60); substantial (range 0.61–0.80); and almost perfect (range 0.81–1.00).(14)
RESULTS
The classification of these elements is summarised by chapter and subchapter in
Table II
Strength of agreement by domain based on Landis and Koch’s classification method.
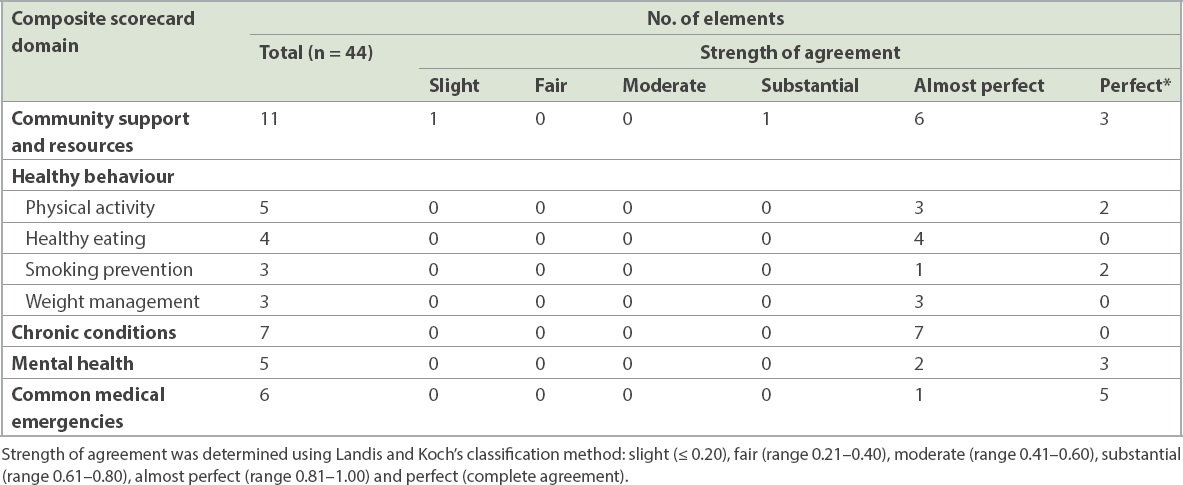
The weighted kappa values for the measurable elements were concentrated in the ‘almost perfect’ and ‘perfect’ categories for most chapters and subchapters, implying a high degree of agreement between Raters 1 and 2 in our study. A dissimilar trend was observed for the domain of community support and resources where, despite most of the measurable elements being clustered in the almost perfect and perfect categories, a couple of elements were classified into the slight and substantial categories. Therefore, Raters 1 and 2 had a varying degree of agreement for some elements of this domain.
DISCUSSION
It is important to ensure minimal measurement errors when multiple assessors are associated with the use of composite health promotion scorecards, and accordingly, this study aimed to examine its inter-rater reliability. We found a high degree of agreement for most measurable elements from the domains and subdomains based on Landis and Koch’s classification method. However, a lower degree of agreement was found for a couple of elements from the community support and resources domain. The disagreement could probably be attributed to some differences in the interpretation of interview statements provided by the residential zones.
The use of weighted kappa, as an appropriate inter-rater reliability measure, was advantageous for our study. Weighted kappa was preferred over unweighted kappa, as it would take the ordinal nature of the three-level rating system and the relative differences between levels into consideration,(15) thereby improving the accuracy of the study’s inter-rater reliability. Furthermore, the kappa statistic is a more superior measure than the conventional percent agreement owing to its ability to account for chance agreement.(16) Both raters used the scoring guidelines of the composite scorecard, thereby minimising potential variability associated with subjective scoring preferences.
The main limitation was the small number of raters and residential zones being assessed in the study, thereby affecting the accuracy of the inter-rater reliability measured. As this was a pilot study, it was conducted only among a limited number of constituency zones. It could also be argued that the high degree of agreement was on account of the background of the raters, who were epidemiologists with formal training in public health. However, scoring guidelines were created in a manner that would be simple for non-professionals to use. Furthermore, the feasibility of the score and the face validity of the scoring guidelines were evaluated by grassroots leaders in the community. Nonetheless, it is still pertinent that the current raters were not the eventual intended users of the composite scorecard, and this has been identified as an area for improvement in future studies.
Owing to the nature of implementation on the ground, there was a lack of complete independence in the assessment of the residential zones by the two raters. For example, part of the assessment for the scoring involved meeting with a group of committee members, including chairpersons of the zone, to obtain information about the zone’s programmes and practices. However, this could not be conducted separately for the raters, as it was not practically feasible to organise multiple sessions. Nevertheless, as the raters referenced the scoring guidelines and scored independently of each other, this is unlikely to have overtly influenced the end scores given to the zones.
In conclusion, the composite health promotion scorecard yielded similar scores for the same residential zone, even when used repeatedly by different users. Further exploration could involve non-professional raters in assessments of residential zones.
ACKNOWLEDGEMENTS
We would like to thank Mr Johnny Wong for his help with the statistical analysis.