

Abstract
We described two patients who were successfully resuscitated from out-of-hospital cardiac arrest. Their ECGs showed ST elevations in V1 and aVR, as well as diffuse ST depression. Their ST elevation in V1 was noted to be greater than in aVR. While one patient was found to have an occlusion of the right ventricular (RV) branch of the right coronary artery, the other was found to have an occlusion of a proximal non-dominant right coronary artery supplying the RV branch. Successful primary percutaneous coronary intervention was performed for each patient with angioplasty and implantation of a drug-eluting stent. Both patients made good physical and neurological recovery.
CASE 1
CLINICAL PRESENTATION
A 42-year-old man with no significant past medical history or known cardiovascular risk factors had an out-of-hospital cardiac arrest while jogging. He received bystander cardiopulmonary resuscitation (CPR) immediately. Within five minutes of his collapse, paramedics arrived and used an automatic external defibrillator (AED) on him. Spontaneous circulation was re-established after the second cycle of CPR, with spontaneous breathing effort. He was taken to the local hospital emergency department and intubated, as he did not regain consciousness. What does the electrocardiogram (ECG) in
Fig. 1
Case 1: Patient’s ECG on presentation.
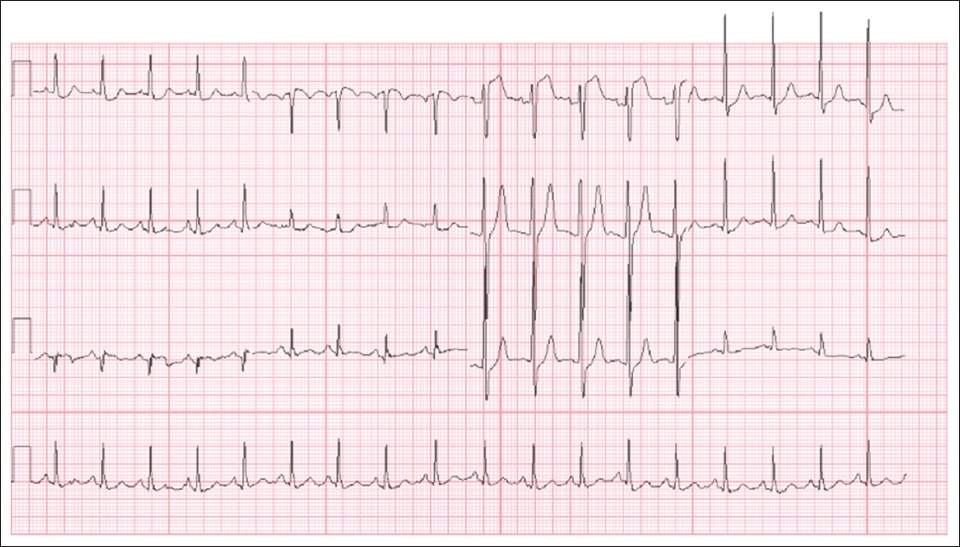
ECG INTERPRETATION
The initial ECG showed sinus rhythm (
CLINICAL COURSE
Emergency coronary angiography revealed a proximal thrombotic occlusion in a large right ventricular (RV) branch of the right coronary artery (
Fig. 2
Case 1: (a) Initial coronary angiogram shows the proximal occlusion of the right ventricular (RV) branch of the right coronary artery (arrow). (b) Coronary angiogram shows good flow into the RV branch of the right coronary artery post angioplasty (arrow).
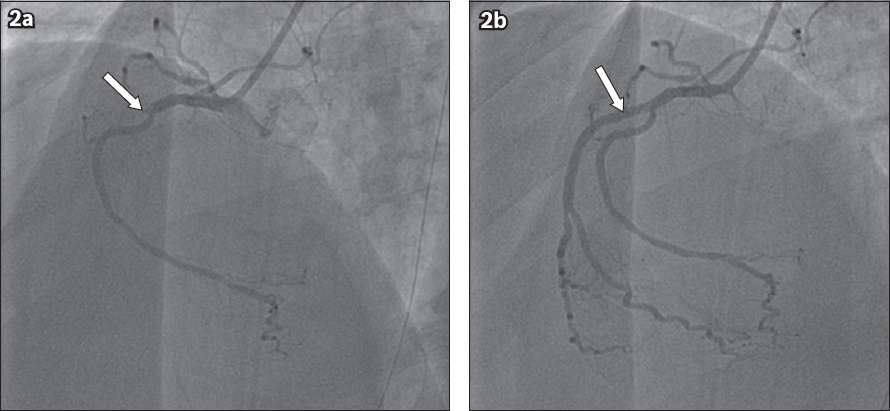
Fig. 3
Case 1: Right-sided chest leads of the patient show subtle ST elevation in V4R, V5R and V6R.
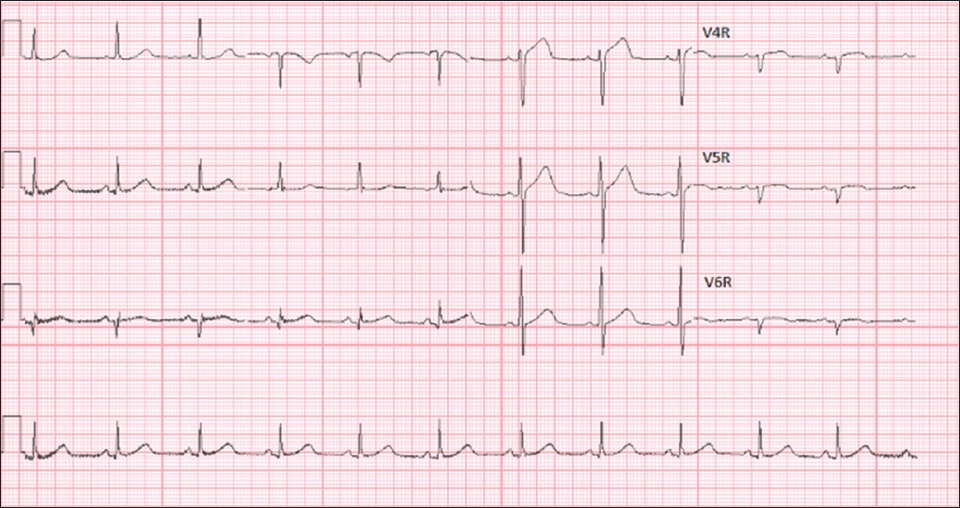
Fig. 4
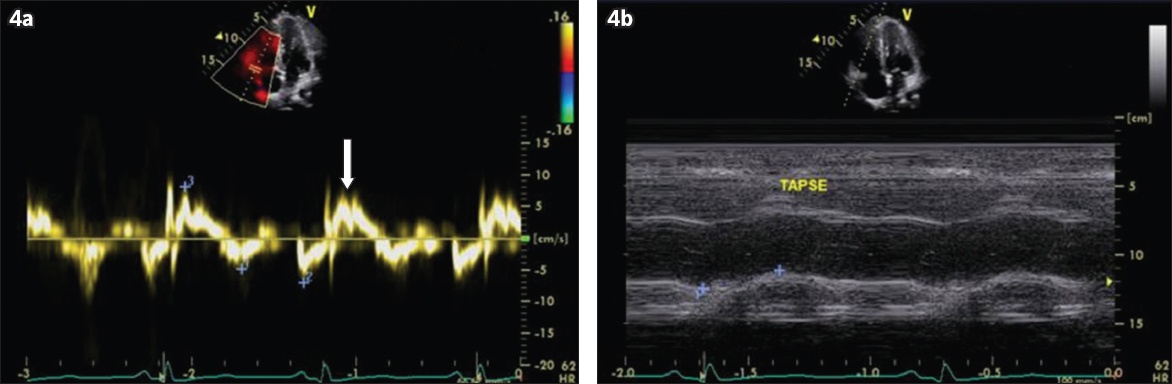
Case 1: Echocardiograms show (a) right ventricular (RV) systolic excursion velocity of 8 cm/second (arrow), suggesting moderate RV systolic dysfunction; and (b) tricuspid annular plane systolic excursion of 13 mm, indicating mild to moderate reduction in RV systolic function.
On the day of admission, the patient was hypotensive with systolic blood pressure in the range of 70–80 mmHg. He required administration of multiple fluid boluses that amounted to 5 L in total in order to improve his preload and, hence, his blood pressure. Three days later, the patient was successfully weaned off therapeutic hypothermia and extubated. His hospital stay was uncomplicated and without any further arrhythmias. He made a complete neurological recovery and was discharged ten days after admission.
CASE 2
CLINICAL PRESENTATION
A 39-year-old man, who was a hepatitis B carrier without other past medical history, had an out-of-hospital cardiac arrest while working in a food centre. He was started on bystander CPR immediately until paramedics arrived. His initial rhythm was ventricular fibrillation. The resuscitation attempt continued while he was being transported to the hospital. Three shocks were given before the patient had a return of spontaneous circulation on arrival at the hospital. He was alert and conversant when he was assessed in the emergency department.
ECG INTERPRETATION
The initial ECG (
Fig. 5
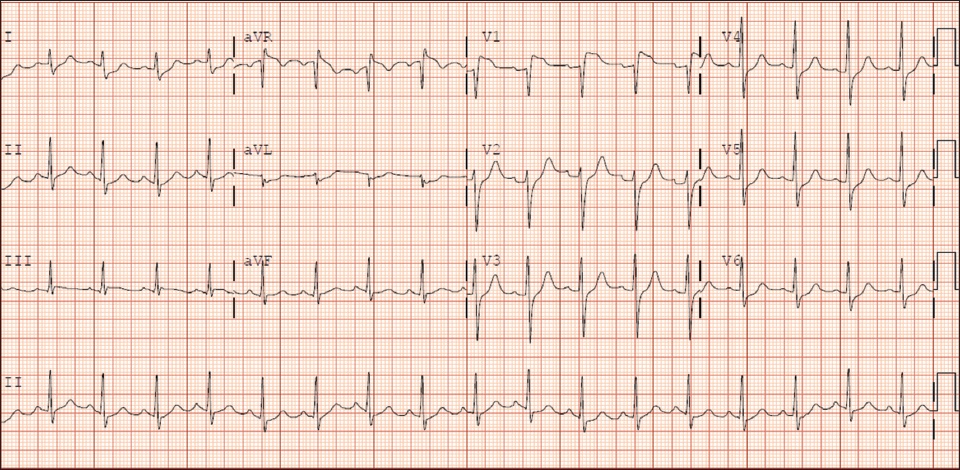
Case 2: Initial ECG of the patient shows ST elevation in V1 that is higher than the ST elevation in aVR.
CLINICAL COURSE
Emergency coronary angiography showed an occlusion in the non-dominant right coronary artery just proximal to the origin of the RV branch (
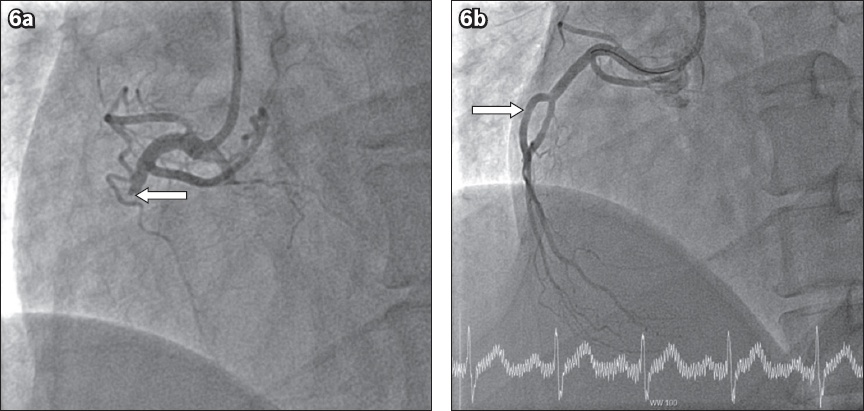
Fig. 6
Case 2: (a) Initial coronary angiogram shows occlusion of the proximal non-dominant right coronary artery (RCA; arrow). (b) Post-intervention coronary angiogram shows good flow in the proximal non-dominant RCA (arrow).
DISCUSSION
In both patients, the presenting ECG, coronary angiogram and echocardiography findings were consistent with an isolated RV infarction. As isolated RV infarction is rare, it is not uncommon to misinterpret it to be an infarction of the anterior left ventricular wall, or even a left main stem occlusion, because of ST changes in the anterior leads V1–V3.(1-3) However, in these cases, ST elevation in V1 was more marked than ST elevation in aVR, which differentiates acute RV infarction from anterior wall infarction or left main coronary artery infarction.(1,3) This might be because anatomically, lead V1 is located directly over the right ventricle, thus, V1 ST elevation is also greater than ST elevation in V2 and V3 in both cases.
Obtaining right-sided ECG V4R, V5R and V6R leads may aid in the diagnosis, since ST elevation and Q waves in V4R may be diagnostic for isolated RV infarction.(3,4) On the other hand, although a posterior ECG (leads V7–V9) has utility to detect infarction in the posterior circulation of the left ventricle, it would not be useful in diagnosing an RV infarction. It should also be noted that the anterior chest leads are perpendicular to the limb leads and should not cause reciprocal inferior ST depression in the limb leads, unless there is widespread left ventricular ischaemia causing ST depression. The inferior limb leads in II, III and aVF are, in fact, reciprocal to limb leads I and aVL.(4)
The patient’s coronary angiogram in Case 1 showed occlusion in the RV branch, which was consistent with the ECG finding of acute isolated RV infarction. More commonly, classic inferior ST elevation myocardial infarction presenting with RV failure would have an occlusion in the proximal right coronary artery proximal to the RV branch. However, in Case 1, the main right coronary artery branch was spared, while the occlusion was confined to the RV branch, causing an isolated RV infarction. The patient in Case 2 had a proximal occlusion of a non-dominant right coronary artery. As the non-dominant right coronary artery predominantly supplies the right ventricle, his presentation mimicked that of an isolated RV infarction.
The involvement of the myocardium during occlusion of the right coronary artery is typically greater in a right-dominant coronary system when the posterior descending artery and the posterolateral artery originate from the right coronary artery. In a minority of patients with a left-dominant circulation, where the posterior descending artery and the posterolateral artery branch off from the left circumflex artery, the right coronary artery is non-dominant. A non-dominant right coronary artery may have limited contribution to the left ventricle, as observed with the patient in Case 2.
An important complication to recognise with RV infarction is RV failure. As such, adequate preload is vital to maintain satisfactory cardiac output. The patient in Case 1 had myocardial infarction while he was jogging and was thus likely to have lost a substantial amount of fluid through perspiration. He was dehydrated and intravascularly depleted at presentation. This fluid deficit had to be taken into account during the initial resuscitation in order to maintain his preload and cardiac output. In patients who are hypotensive with RV failure, the first-line treatment is augmentation of RV preload with boluses of intravenous fluids.(5) Thus, nitrates are not haemodynamically favourable in these patients, as they would cause venodilatation, which may reduce the RV preload.(3) As these patients are usually responsive to an increase in preload from intravenous fluids, inotropes and mechanical support with devices such as an intra-aortic balloon pump are not considered as first-line therapy.(5) Maintaining adequate RV preload was less important for the patient in Case 2, as he had not been engaged in intense physical activity that led to substantial fluid loss. Left ventricular systolic function is usually not an issue in isolated RV infarction, as seen in both patients.
An isolated RV infarction may be proarrhythmic, and patients may present with out-of-hospital cardiac arrest, as seen in both our patients. It was previously postulated that RV infarction causes sympathetic and vagal denervation at the right ventricular outflow tract (RVOT) and lateral and septal sides of the viable peri-infarct area. Autonomic denervation in the RVOT may contribute to the development of ventricular tachyarrhythmias during the acute phase of RV infarction.(6)
Although isolated RV infarction has been described to have a good prognosis,(1-3,7) the prognosis following cardiac arrest in these cases was also dependent on early CPR. Both patients had a short no-flow time, which is defined as time without chest compression during the first period of cardiac arrest, as they received almost immediate bystander CPR. While the patient in Case 2 was alert and talking on arrival at the emergency department, the patient in Case 1 remained unconscious on arrival at the hospital. Thus, the patient in Case 1 was also given therapeutic hypothermia, which could have contributed to a favourable neurological recovery.(8,9) Although the rate of bystander CPR in Singapore remained at a low of about 20% until 2011, the implementation of dispatcher-assisted CPR by the Singapore Civil Defence Force has led to a rise in bystander CPR rates, to 49% in 2015.(10-12) Thus, dispatcher-assisted CPR may improve outcomes in patients with out-of-hospital cardiac arrest in Singapore.(13)
One possible reason that laypersons may be averse to performing bystander CPR is that mouth-to-mouth ventilation is still included in the standard Basic Cardiac Life Support (BCLS) protocol, although evidence suggests that it does little to improve outcomes.(14,15) Making mouth-to-mouth ventilation optional in the standard BCLS protocol taught to members of the public may encourage more bystander CPRs. Furthermore, using a simpler protocol may boost confidence. This would translate to improved outcomes for patients suffering from out-of-hospital cardiac arrest in Singapore.(11-14,16)
While 82.6% and 57.2% of Singaporeans feel that all adults should be trained in CPR and AED, respectively, the actual proportion of Singaporeans who are trained in these is only 34.3% and 31.4%, respectively.(17) In order to enhance training in CPR and AED, the National Resuscitation Council has set up a system for monitoring and maintaining standards of life support training, leading to a large increase in the number of training centres for BCLS.(18) Bystander CPR has also been promoted through community-based training programmes. These initiatives would likely lead to improved outcomes in future for individuals with out-of-hospital cardiac arrests.(18)
SMJ-60-129.pdf