Author Information >Copyright and License information >
1Department of Obstetrics and Gynaecology, National University Hospital, Singapore 2Yong Loo Lin School of Medicine, National University of Singapore, Singapore Correspondence: Dr Arundhati Gosavi, Registrar, Department of Obstetrics and Gynaecology, National University Hospital, National University Health System, NUHS Tower Block, Level 12, 1E Kent Ridge Road Singapore 119228. arundhati_gosavi@nuhs.edu.sg
The study aimed to assess the level of awareness and knowledge of contraception among women in Singapore, and identify the factors that influence contraception choice.
METHODS
We conducted a cross-sectional survey of 259 female patients, aged 21–49 years, who attended the Obstetrics and Gynaecology Clinic at National University Hospital, Singapore. An original questionnaire on nine contraceptive methods was used. Respondents who had ≥ 2 correct answers for a method (out of four questions) were considered to have good knowledge of the method. Participants were asked to rate factors known to influence contraceptive choice as important or not important.
RESULTS
Awareness of the following methods was high: condom (100.0%), oral contraception pill (89.2%), tubal ligation (73.0%) and copper intrauterine device (IUD) (72.2%). The women were least aware of hormonal IUD (24.3%). Women who were parous, had a previous abortion, had completed their family or used contraception previously were more likely to have a higher awareness of contraception. 89.2% of the women had good knowledge of the condom; among those aware of hormonal IUD, only 46.0% had good knowledge of it. Women who had used hormonal IUD and the condom were more likely to have good knowledge of them. Many rated efficacy (90.5%) and a healthcare professional’s advice (90.1%) as important in contraceptive choice. Few considered peer influence (21.0%) and cultural practices (16.3%) to be important.
CONCLUSION
Women in Singapore have poor awareness and knowledge of contraception, especially long-acting reversible methods. More effective ways are needed to educate women about contraceptive methods.
Contraceptive use is the cornerstone of prevention for unintended pregnancy.(1) In Singapore, about one in five pregnancies are terminated,(2,3) with unintended pregnancies accounting for most of the terminations.(4,5) This indicates an unmet need for contraception. Termination of pregnancy (TOP) is associated with significant risks. Vacuum aspiration involves short-term risks (e.g. associated with general anaesthesia, uterine haemorrhage, perforation and infection) and long-term risks (e.g. increased risk of subsequent preterm birth),(6) while medical TOP comes with adverse effects (e.g. lower abdominal pain, fever and diarrhoea) and the need for surgical intervention should TOP fail.(7) Hence, prevention of unintended pregnancies is a long-term healthcare goal with significance for public health; this has been outlined in the Millennium Development Goals Report by the United Nations.(8) Prevention of unintended pregnancies can also lead to reductions in healthcare costs.(9) Good knowledge of contraception has been associated with increased contraceptive use, which in turn reduces the incidence of abortion.(10)
While a wide variety of contraceptive methods are available in Singapore, there is no robust data about the level of awareness and knowledge of contraception among women in Singapore. It is thus unclear whether current measures to educate women on contraception are effective. Women consider many factors when choosing a method of contraception.(11-14) Although there are previous studies on contraceptive knowledge and factors determining choice of contraception, most of them were conducted on North American and European populations, and may not reflect the situation in Singapore due to differences in socioeconomic and cultural factors. Hence, the primary aim of the present study was to ascertain the level of awareness and knowledge of contraception among women in Singapore. The secondary aim was to identify factors that influence the women’s choice of contraception.
METHODS
A cross-sectional survey of female patients, aged 21–49 years, who presented to the Obstetrics and Gynaecology Clinic at National University Hospital, Singapore, was conducted from 19 February 2013 to 14 January 2014. Ethics approval was obtained from the Domain Specific Review Board of the National Healthcare Group, Singapore. Written informed consent was obtained from all participants before they answered the survey. The survey was administered by a trained interviewer in a private room to maintain privacy and confidentiality. The answers given were verbally reviewed with the participant after each question. No financial compensation was given to the participants and no funding was obtained for this study.
An original questionnaire was developed for the purpose of this study. It was designed to assess awareness and knowledge of nine methods of contraception that are available in Singapore, namely the oral contraceptive pill (OCP), implant, patch, copper intrauterine device (IUD), levonorgestrel-releasing intrauterine system (LNG-IUS, also known as hormonal IUD), injectable contraceptive, condom, tubal ligation and vaginal ring. For each of these nine methods, we assessed the participant’s level of awareness by asking her if she had heard of the method before. If she had heard of it, we asked her four true/false questions that assessed various knowledge aspects and myths about the method (e.g. how it is used, efficacy, side effects, duration of action, reversibility and protection against sexually transmitted infections). The questionnaire was developed after we conducted a thorough search on existing literature and obtained expert opinion about contraceptive methods. Participants who had ≥ 2 correct answers for a method (out of four questions) were considered to have good knowledge of that method, while those who had one or no correct answers were deemed to have poor knowledge of the method.
The demographic information of the participants (i.e. age, marital status, years of marriage, highest education level, ethnicity, religion, parity and fertility intention) was collected. Information about their current and previous contraceptive use was also collected. To identify reasons for the adoption or non-adoption of contraceptive methods, intrinsic factors (i.e. properties of the contraceptive methods) and extrinsic factors (i.e. sociocultural influences) that could affect contraceptive choice were studied. Participants were asked to rate each factor as important or not important in their choice of contraception.
All statistical analyses were performed using IBM SPSS Statistics for Windows version 21.0 (IBM Corp, Armonk, NY, USA). Univariate descriptive statistics were used for all study variables. Fisher’s exact test was used to identify the predictors of good knowledge of each method of contraception. A p-value < 0.05 was considered statistically significant.
RESULTS
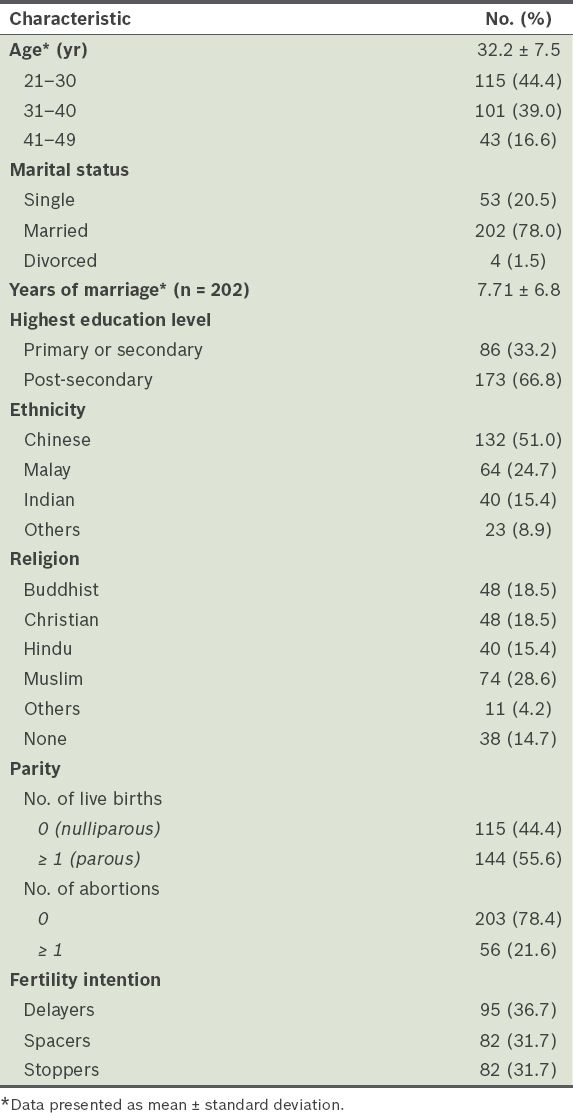
A total of 275 women were approached, but 16 declined to participate. Hence, 259 questionnaires were completed, yielding a response rate of 94.2%. The mean age of the participants was 32.2 ± 7.5 years (Table I). Most of the participants were married (78.0%) and most had post-secondary education (66.8%). The majority were Chinese (51.0%), followed by Malays (24.7%), Indians (15.4%) and others (8.9%). Among the study group, 55.6% were parous and 21.6% had a previous abortion. In terms of fertility intention, the proportions of women who intended to delay, space or stop pregnancy were 36.7%, 31.7% and 31.7%, respectively.
Table I
Sociodemographic characteristics of the participants (n = 259).
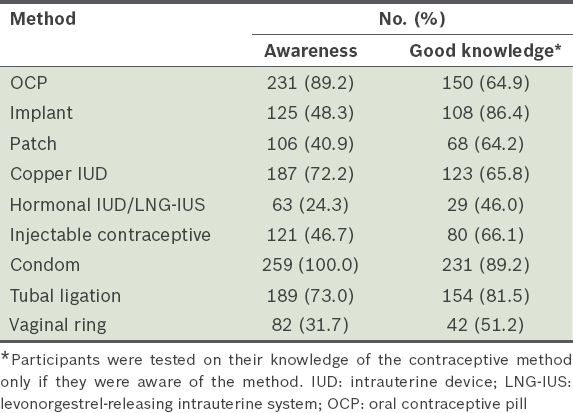
Table II shows the number of women who were aware or had good knowledge of the nine contraceptive methods. All of the 259 women were aware of the condom as a contraceptive method and more than half of them were aware of OCP, tubal ligation and copper IUD. Less than half of the women were aware of the other five methods, with hormonal IUD/LNG-IUS ranking the lowest (24.3%). In terms of knowledge about the contraceptive methods, 89.2% of the women had good knowledge of the condom (the highest among the nine methods). On the other hand, only 46.0% of those who were aware of hormonal IUD/LNG-IUS had good knowledge of it.
Table II
Awareness and knowledge of contraceptive methods among the participants (n = 259).
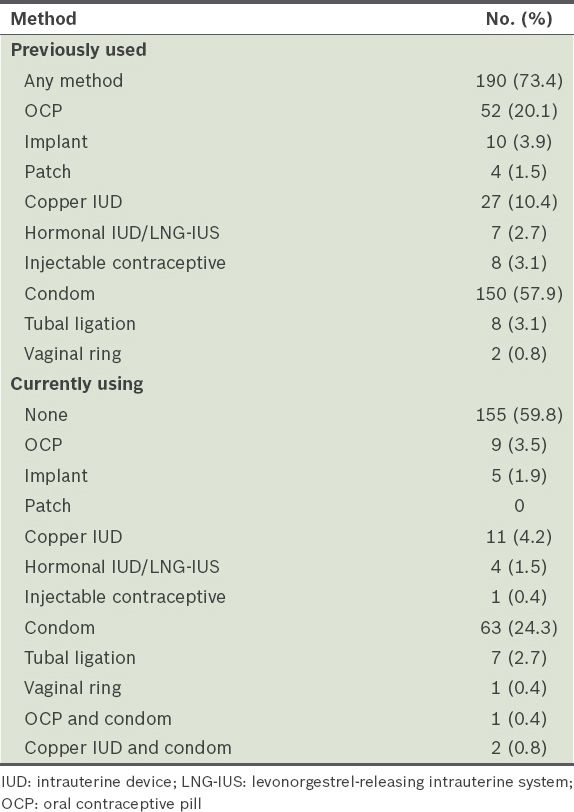
Table III shows the pattern of contraceptive use among the 259 participants. Despite their mean age of 32.2 years, 59.8% were not currently using contraception. The most commonly used method was the condom (60.6% of the 104 women who were currently using contraception). Although 48.3% of the women were aware of the implant as a contraceptive method and 86.4% of those who were aware had good knowledge about it, the uptake of this method was low (only 4.8% of the 104 women currently using contraception). Methods that the participants had poor awareness and knowledge of, such as hormonal IUD/LNG-IUS, the patch and the vaginal ring, had correspondingly negligible uptake.
Table III
Pattern of contraception use among the participants (n = 259).
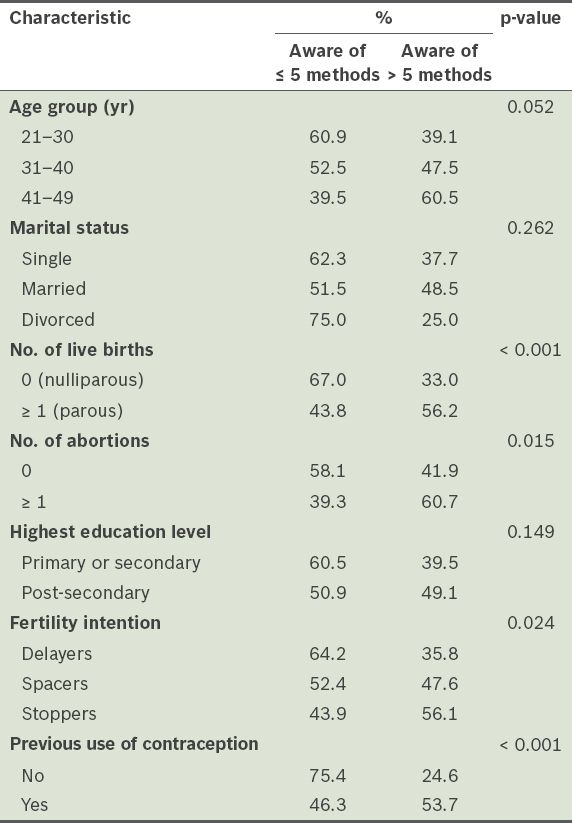
Table IV shows the association between awareness of contraceptive methods and selected characteristics. Parity was found to be significantly associated with greater awareness of contraceptive methods; 56.2% of the parous women were aware of > 5 methods, compared to only 33.0% of the nulliparous women (odds ratio [OR] 2.61, 95% confidence interval [CI] 1.57–4.34). Previous abortion was also significantly associated with greater awareness of contraceptive methods. 60.7% of women with ≥ 1 abortion were aware of > 5 methods as compared to 41.9% of the women who had no previous abortions (OR 2.15, 95% CI 1.17–3.93). Stoppers and spacers were also more likely to be aware of > 5 contraceptive methods as compared to delayers (56.1%, 47.6% and 35.8%, respectively; p = 0.024). Women who had used contraception before were more likely to be aware of > 5 contraceptive methods as compared to those who had no experience with contraception (53.7% vs. 24.6%; OR 3.55, 95% CI 1.91–6.57).
Table IV
Association between awareness of contraceptive methods and selected characteristics (n = 259).
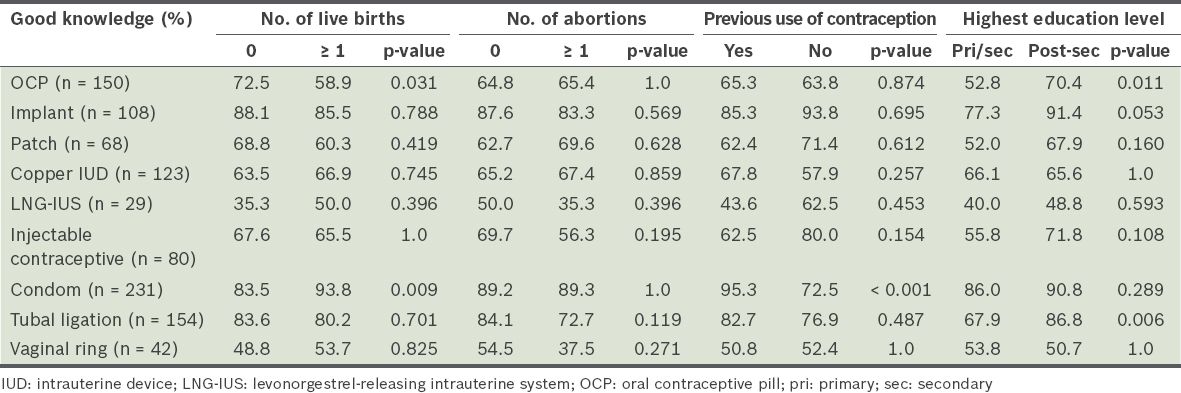
Table V shows the association between good knowledge of individual contraceptive methods and selected characteristics. A higher proportion of nulliparous women had good knowledge of OCP as compared to parous women (p = 0.031). On the other hand, a higher proportion of parous women had good knowledge of condoms as compared to nulliparous women (p = 0.009). For all nine contraceptive methods, there was no significant association between a previous abortion and good knowledge of the method. A higher proportion of women who had previously used contraception had good knowledge of condoms as compared to those who had never used contraception (p < 0.001). When the associations between education level and good knowledge of the various contraceptive methods were studied, only OCP (p = 0.011) and tubal ligation (p = 0.006) showed a significant association.
Table V
Association between good knowledge of a contraceptive method and selected characteristics.
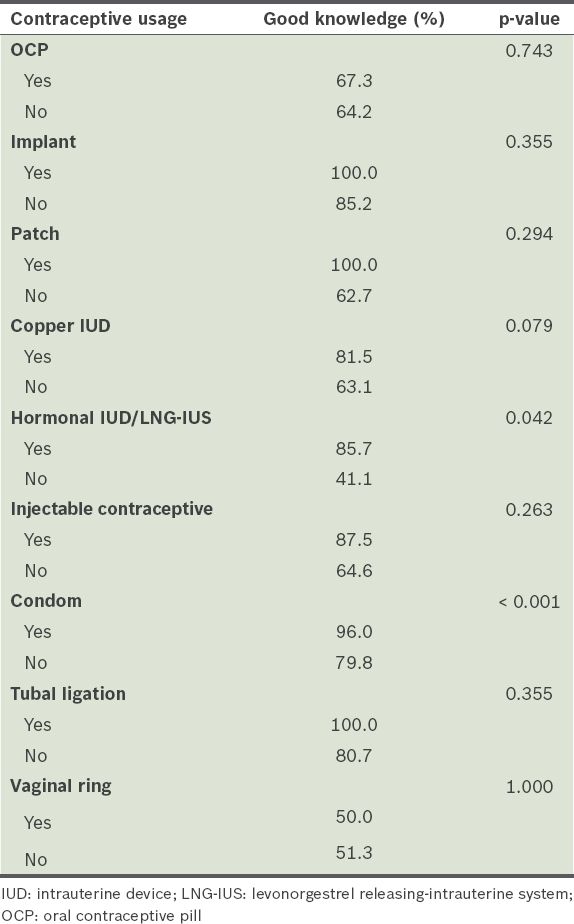
We also analysed the relationship between experience in using a specific contraceptive method and having good knowledge of that method (Table VI). We found that those who had experience using hormonal IUD/LNG-IUS (p = 0.042) and the condom (p < 0.001) were more likely to have good knowledge of those methods. No association between experience and good knowledge was found for the other methods.
Table VI
Association between previous use of a particular contraceptive method and good knowledge of the method.
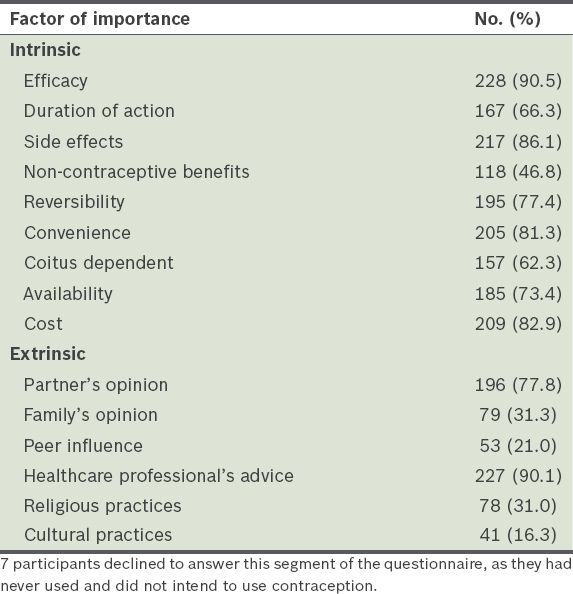
Table VII shows the intrinsic and extrinsic factors that the participants rated as important in their choice of contraception. Seven participants declined to answer this segment of the questionnaire, as they had never used and did not intend to use contraception. In terms of intrinsic factors, efficacy was rated as important by most of the participants (90.5%); a substantial proportion were concerned about side effects (86.1%), while only 46.8% thought that non-contraceptive benefits such as reducing menstrual flow or acne were important. In terms of extrinsic factors, 90.1% and 77.8% of the participants, respectively, considered the advice of a healthcare professional and their partner’s opinion to be important. Few rated peer influence (21.0%) and cultural practices (16.3%) as important.
Table VII
Factors of importance in participants’ choice of contraception (n = 252).
DISCUSSION
Global trends over the last two decades highlight the need for increased investments in interventions aimed at managing the surge in demand for contraception.(15) This is the first survey study to assess the awareness and knowledge of available methods of contraception in Singapore among Singaporean women. Although most of the women in the study were highly educated (i.e. had post-secondary education), most had poor awareness and knowledge of long-acting reversible methods of contraception and newer combined hormonal methods. These results are similar to those of previous studies on contraceptive knowledge conducted in developed countries.(16-19) In our study, the uptake of long-acting reversible methods of contraception and newer combined hormonal methods was also very low. This is despite the fact that long-acting reversible methods are highly recommended due to their high efficacy, low side-effect profile, high satisfaction and high continuation rates (even in adolescents and young women).(20-22) The cost-effectiveness of long-acting reversible methods has also been well established.(23)
In the present study, participants scored highest in awareness and good knowledge of the condom, which was similar to the finding of a study conducted on European and American women.(24) This is likely due to condoms being widely available and highly publicised in safe sex campaigns. Poor publicity by doctors, limited availability and patient discomfort with invasive methods are possible reasons for the poor awareness and knowledge of methods such as LNG-IUS, the patch and the vaginal ring among Singaporean women.
While OCP is the most commonly used contraceptive method in countries like the United States, the United Kingdom, Italy and Germany,(24) the condom was the method with the highest uptake in our study. This is in keeping with the finding that the participants had the highest level of awareness and knowledge of condoms. Low uptake of the implant, which was observed in this study and in studies conducted in other countries,(24) could be due to the invasive nature of this method, the greater one-time cost and the necessity for visits to a doctor.
Positive associations between increased awareness of contraceptive methods and both parity and a history of abortion suggest that current postnatal and pre-abortion contraception counselling practices may be effective in promoting awareness. However, these counselling sessions may not be effective in promoting good knowledge of contraceptive methods, as no association was found between good knowledge of doctor-dependent contraceptive methods and parity or a history of abortion. Moreover, we found that participants who had used a particular method were not more likely to have good knowledge of that method (with the exception of LNG-IUS), suggesting that the women were not properly educated about the methods that were prescribed to them.
Education level was generally not associated with greater awareness or good knowledge of contraceptive methods among our participants; even those who had post-secondary education did not have good knowledge about long-acting contraceptives. The sex education that is conducted in Singapore schools (up to the pre-university level) promotes abstinence, with little focus on contraception. As such, women have to obtain information on contraceptives from other sources such as healthcare professionals or the Internet. Thus, doctors and nurses play a crucial role in educating women about contraception and making recommendations on methods that best meet their needs.(24-26)
Similar to the findings of other studies,(13,14) efficacy was the biggest concern among the women in the present study when choosing a method of contraception. Thus, more emphasis should be placed on imparting information on the efficacy, side effects and reversibility of various types of contraceptives. As the women’s choice of contraception was also found to be heavily influenced by their partner’s opinion, we believe that partner education is equally important. Although previous studies found that the religious factor has a significant effect on contraceptive choice,(27,28) this was not found to be a major influence in our study.
This study was not without limitations. For one, it was conducted in a subsidised specialist clinic of a restructured hospital and hence, the results may not be representative of the general population. The cross-sectional nature of the study was also a limitation, as it precluded us from studying the changes in contraceptive choice over the life course of these women. In addition, our criterion for good knowledge of contraception was arbitrarily set at ≥ 2 correct answers out of four questions, which is a fairly lenient standard. A stricter criterion would have led to results that showed poorer knowledge of contraception among the women.
There is a need for a nationwide, multicentre, longitudinal study involving a large group of women, with follow-up at regular intervals over an extended period of time. As age and reproductive experiences have been shown to impact contraceptive decisions,(29,30) such a large longitudinal study could also investigate factors affecting the actual use of contraceptives. Previous studies have demonstrated the presence of knowledge gaps and misconceptions about contraception among physicians, which affect their ability to recommend the use of contraception.(31-33) Thus, research could also be conducted to evaluate the knowledge, attitudes and practices of healthcare professionals in relation to contraception. Structured training of healthcare professionals can then be undertaken to overcome the barrier.(34) Factors affecting compliance to and continuation of contraception can also be studied in order to improve the management of women who are already using reliable methods of contraception.
The results of the present study can provide insights into available opportunities for improving contraception services in Singapore. We recommend that nurses who are specially trained in contraception counselling be stationed at postnatal wards, obstetrics and gynaecology specialist clinics, and contraception booths at primary healthcare facilities, to provide comprehensive counselling on contraception for couples. Such counselling has been shown to be effective in some centres.(35) Dedicated services by community workers, antenatal contraceptive counselling(36) and theory-based interventions (e.g. the use of motivational interviews and social cognitive theory) have been found to be clinically effective in increasing the uptake of IUD.(37) Well-designed leaflets and other audiovisual aids can be used to complement the personal interaction couples have with the healthcare provider during counselling sessions.(38) An online contraception advice service could also be set up to provide easy access to reliable and accurate information about contraception. We also recommend that opportunistic contraception education be offered to all women of child-bearing age during their general visits to healthcare facilities. Efforts to raise awareness on contraceptive methods may be better targeted at nulliparous women, as this group of women tends to have lower awareness of contraceptive methods.
To study the effectiveness of our recommended interventions in improving awareness and knowledge on contraception, and ultimately in reducing abortion rates, prospective trials would need to be carried out. Although we did not include teenagers in the present study, we would like to highlight the importance of contraception education for this age group, as teenagers were found to be more likely to not use contraception and present late for abortion.(4,5)
In conclusion, the present study provides evidence that women in Singapore have poor knowledge of a few contraceptive methods, such as hormonal IUD and vaginal ring. More effective ways of educating women on contraception are needed in order to increase the uptake of reliable methods of contraception and improve the reproductive health of Singaporean women.
References Cheng Y, Xu X, Xu J, et al. The need for integrating family planning and postabortion care in China.Int J Gynaecol Obstet. 2008;103:140-3. Ministry of Health, Singapore. Abortion statistics. Available at: http://www.moh.gov.sg/content/moh_web/home/pressRoom/Parliamentary_QA/2013/abortion-statistics.html. Accessed March 30 2014. Department of Statistics, SingaporeLatest data. Available at: http://www.singstat.gov.sg/statistics/latest-data. Accessed March 30 2014. Singh K, Fong YF, Loh SY.Profile of women presenting for abortions in Singapore at the National University Hospital.Contraception. 2002;66:41-6. Lim L, Wong H, Yong E, Singh K.Profiles of women presenting for abortions in Singapore: focus on teenage abortions and late abortions.Eur J Obstet Gynecol Reprod Biol. 2012;160:219-22. Royal College of Obstetricians and GynaecologistsThe care of women requesting induced abortion. Evidence-based clinical guideline number 7. 2011;3rd edUnited Kingdom RCOG Press. Singh K, Fong YF, Dong F.A viable alternative to surgical vacuum aspiration: repeated doses of intravaginal misoprostol over 9 hours for medical termination of pregnancies up to eight weeks.BJOG. 2003;110:175-80. United NationsThe millennium development goals report 2013. Available at: http://www.un.org/millenniumgoals/pdf/report-2013/mdg-report- 2013-english.pdf. Accessed March 30, 2014. World Health OrganizationPackages of interventions for family planning, safe abortion care, maternal, newborn and child health. Available at: http://apps.who.int/iris/bitstream/10665/70428/1/WHO_FCH_10.06_eng.pdf. Accessed March 30 2014. Marston C, Cleland J.Relationships between contraception and abortion: a review of the evidence.Int Fam Plan Perspect. 2003;29:6-13. de Irala J, Osorio A, Carlos S, Lopez-del Burgo C.Choice of birth control methods among European women and the role of partners and providers.Contraception. 2011;84:558-64. Oddens BJ.Determinants of contraceptive use among women of reproductive age in Great Britain and Germany. II: Psychological factors.J Biosoc Sci. 1997;29:437-70. Steiner MJ, Trussell J, Mehta N, et al. Communicating contraceptive effectiveness: a randomized controlled trial to inform a World Health Organization family planning handbook.Am J Obstet Gynecol. 2006;195:85-91. Grady WR, Klepinger DH, Nelson-Wally A.Contraceptive characteristics: the perceptions and priorities of men and women.Fam Plann Perspect. 1999;31:168-75. Alkema L, Kantorova V, Menozzi C, Biddlecom A.National, regional, and global rates and trends in contraceptive prevalence and unmet need for family planning between 1990 and 2015: a systematic and comprehensive analysis.Lancet. 2013;381:1642-52. Eisenberg DL, Secura GM, Madden TE, et al. Knowledge of contraceptive effectiveness.Am J Obstet Gynecol. 2012;206:479-e1-9. Kumar MM, Lim R, Langford C, et al. Sexual knowledge of Canadian adolescents after completion of high school sexual education requirements.Paediatr Child Health. 2013;18:74-80. Sokkary N, Mansoa R, Yoost J, et al. A multicenter survey of contraceptive knowledge among adolescents in North America.J Pediatr Adolesc Gynecol. 2013;26:274-6. Reina MF, Ciaravino H, Llovera N, Castelo-Branco C.Contraception knowledge and sexual behaviour in secondary school students.Gynecol Endocrinol. 2010;26:479-83. Committee on Adolescent Health Care Long-Acting Reversible Contraception Working Group, The American College of Obstetricians and Gynecologists. Committee opinion no. 539: adolescents and longacting reversible contraception: implants and intrauterine devices.Obstet Gynecol. 2012;120:983-8. Peipert JF, Zhao Q, Allsworth JE, et al. Continuation and satisfaction of reversible contraception.Obstet Gynecol. 2011;117:1105-13. Winner B, Peipert JF, Zhao Q, et al. Effectiveness of long-acting reversible contraception.N Engl J Med. 2012;366:1998-2007. Mavranezouli I.LARC Guideline Development GroupThe cost-effectiveness of long-acting reversible contraceptive methods in the UK: analysis based on a decision-analytic model developed for a National Institute for Health and Clinical Excellence (NICE) clinical practice guideline.Hum Reprod. 2008;23:1338-45. Johnson S, Pion C, Jennings V.Current methods and attitudes of women towards contraception in Europe and America.Reprod Health. 2013;10:7. Mansour D, Rosales C, Cox M.Women’s awareness of long-acting, reversible contraceptive methods (LARCs) in community family planning clinics and general practice.Eur J Contracept Reprod Health Care. 2008;13:396-9. Bitzer J, Gemzell-Danielsson K, Roumen F, et al. The CHOICE study: effect of counselling on the selection of combined hormonal contraceptive methods in 11 countries.Eur J Contracept Reprod Health Care. 2012;17:65-78. Hayat H, Khan PS, Imtiyaz B, Hayat G, Hayat R.Knowledge, attitude and practice of contraception in rural Kashmir.J Obstet Gynaecol India. 2013;63:410-4. Goldscheider C, Mosher WD.Patterns of contraceptive use in the United States: the importance of religious factors.Stud Fam Plann. 1991;22:102-15. Jacobs J, Stanfors M.Racial and ethnic differences in U.S. women’s choice of reversible contraceptives, 1995-2010.Perspect Sex Reprod Health. 2013;45:139-47. Dehlendorf C, Park SY, Emeremni CA, et al. Racial/ethnic disparities in contraceptive use: variation by age and women’s reproductive experiences.Am J Obstet Gynecol. 2014;210:526-e1-9. Tang J, Maurer R, Bartz D.Intrauterine device knowledge and practices: a national survey of obstetrics and gynecology residents.South Med J. 2013;106:500-5. Stanwood NL, Garrett JM, Konrad TR.Obstetrician-gynecologists and the intrauterine device: a survey of attitudes and practice.Obstet Gynecol. 2002;99:275-80. Moreau C, Bohet A, Hassoun D, Ringa V, Bajos N.FECOND groupIUD use in France: women’s and physician’s perspectives.Contraception. 2014;89:9-16. Lewis C, Darney P, Thiel de Bocanegra H.Intrauterine contraception: impact of provider training on participant knowledge and provision.Contraception. 2013;88:226-31. Lopez LM, Hiller JE, Grimes DA, Chen M.Education for contraceptive use by women after childbirth.Cochrane Database Syst Rev. 2012;8:CD001863. Arrowsmith ME, Aicken CR, Saxena S, Majeed A.Strategies for improving the acceptability and acceptance of the copper intrauterine device.Cochrane Database Syst Rev. 2012;3:CD008896. Lopez LM, Tolley EE, Grimes DA, Chen M, Stockton LL.Theory-based interventions for contraception.Cochrane Database Syst Rev. 2013;8:CD007249. Lopez LM, Steiner M, Grimes DA, Hilgenberg D, Schulz KF.Strategies for communicating contraceptive effectiveness.Cochrane Database Syst Rev. 2013;4:CD006964.
REFERENCES
1. Cheng Y, Xu X, Xu J, et al. The need for integrating family planning and postabortion care in China. Int J Gynaecol Obstet 2008; 103:140-3. https://doi.org/10.1016/j.ijgo.2008.06.013
PMid:18760783
4. Singh K, Fong YF, Loh SY. Profile of women presenting for abortions in Singapore at the National University Hospital. Contraception 2002; 66:41-6. https://doi.org/10.1016/S0010-7824(02)00317-7
5. Lim L, Wong H, Yong E, Singh K. Profiles of women presenting for abortions in Singapore: focus on teenage abortions and late abortions. Eur J Obstet Gynecol Reprod Biol 2012; 160:219-22. https://doi.org/10.1016/j.ejogrb.2011.11.017
PMid:22137571
6. Royal College of Obstetricians and Gynaecologists. The care of women requesting induced abortion. Evidence-based clinical guideline number 7, 3rd ed. United Kingdom: RCOG Press, 2011.
7. Singh K, Fong YF, Dong F. A viable alternative to surgical vacuum aspiration: repeated doses of intravaginal misoprostol over 9 hours for medical termination of pregnancies up to eight weeks. BJOG 2003; 110:175-80. https://doi.org/10.1046/j.1471-0528.2003.02225.x
PMid:12618162
10. Marston C, Cleland J. Relationships between contraception and abortion: a review of the evidence. Int Fam Plan Perspect 2003; 29:6-13. https://doi.org/10.2307/3180995
PMid:12709307
11. de Irala J, Osorio A, Carlos S, Lopez-del Burgo C. Choice of birth control methods among European women and the role of partners and providers. Contraception 2011; 84:558-64. https://doi.org/10.1016/j.contraception.2011.04.004
PMid:22078183
12. Oddens BJ. Determinants of contraceptive use among women of reproductive age in Great Britain and Germany. II: Psychological factors. J Biosoc Sci 1997; 29:437-70. https://doi.org/10.1017/S0021932097004379
PMid:9881146
13. Steiner MJ, Trussell J, Mehta N, et al. Communicating contraceptive effectiveness: a randomized controlled trial to inform a World Health Organization family planning handbook. Am J Obstet Gynecol 2006; 195:85-91. https://doi.org/10.1016/j.ajog.2005.12.053
PMid:16626610
14. Grady WR, Klepinger DH, Nelson-Wally A. Contraceptive characteristics: the perceptions and priorities of men and women. Fam Plann Perspect 1999; 31:168-75. https://doi.org/10.2307/2991589
PMid:10435215
15. Alkema L, Kantorova V, Menozzi C, Biddlecom A. National, regional, and global rates and trends in contraceptive prevalence and unmet need for family planning between 1990 and 2015: a systematic and comprehensive analysis. Lancet 2013; 381:1642-52. https://doi.org/10.1016/S0140-6736(12)62204-1
16. Eisenberg DL, Secura GM, Madden TE, et al. Knowledge of contraceptive effectiveness. Am J Obstet Gynecol 2012; 206:479.e1-9. https://doi.org/10.1016/j.ajog.2012.04.012
PMid:22521458 PMCid:PMC4007217
17. Kumar MM, Lim R, Langford C, et al. Sexual knowledge of Canadian adolescents after completion of high school sexual education requirements. Paediatr Child Health 2013; 18:74-80.
PMid:24421660 PMCid:PMC3567900
18. Sokkary N, Mansouri R, Yoost J, et al. A multicenter survey of contraceptive knowledge among adolescents in North America. J Pediatr Adolesc Gynecol 2013; 26:274-6. https://doi.org/10.1016/j.jpag.2013.04.010
PMid:23849092
19. Reina MF, Ciaravino H, Llovera N, Castelo-Branco C. Contraception knowledge and sexual behaviour in secondary school students. Gynecol Endocrinol 2010; 26:479-83. https://doi.org/10.3109/09513591003649856
PMid:20236027
20. Committee on Adolescent Health Care Long-Acting Reversible Contraception Working Group, The American College of Obstetricians and Gynecologists. Committee opinion no. 539: adolescents and long-acting reversible contraception: implants and intrauterine devices. Obstet Gynecol 2012; 120:983-8. https://doi.org/10.1097/AOG.0b013e3182723b7d
PMid:22996129
21. Peipert JF, Zhao Q, Allsworth JE, et al. Continuation and satisfaction of reversible contraception. Obstet Gynecol 2011; 117:1105-13. https://doi.org/10.1097/AOG.0b013e31821188ad
PMid:21508749 PMCid:PMC3548669
22. Winner B, Peipert JF, Zhao Q, et al. Effectiveness of long-acting reversible contraception. N Engl J Med 2012; 366:1998-2007. https://doi.org/10.1056/NEJMoa1110855
PMid:22621627
23. Mavranezouli I; LARC Guideline Development Group. The cost-effectiveness of long-acting reversible contraceptive methods in the UK: analysis based on a decision-analytic model developed for a National Institute for Health and Clinical Excellence (NICE) clinical practice guideline. Hum Reprod 2008; 23:1338-45. https://doi.org/10.1093/humrep/den091
PMid:18372257
24. Johnson S, Pion C, Jennings V. Current methods and attitudes of women towards contraception in Europe and America. Reprod Health 2013; 10:7. https://doi.org/10.1186/1742-4755-10-7
PMid:23384291 PMCid:PMC3599328
25. Mansour D, Rosales C, Cox M. Women's awareness of long-acting, reversible contraceptive methods (LARCs) in community family planning clinics and general practice. Eur J Contracept Reprod Health Care 2008; 13:396-9. https://doi.org/10.1080/13625180802255693
PMid:19117255
26. Bitzer J, Gemzell-Danielsson K, Roumen F, et al. The CHOICE study: effect of counselling on the selection of combined hormonal contraceptive methods in 11 countries. Eur J Contracept Reprod Health Care 2012; 17:65-78. https://doi.org/10.3109/13625187.2011.637586
PMid:22239264
27. Hayat H, Khan PS, Imtiyaz B, Hayat G, Hayat R. Knowledge, attitude and practice of contraception in rural Kashmir. J Obstet Gynaecol India 2013; 63:410-4. https://doi.org/10.1007/s13224-013-0447-6
PMid:24431689 PMCid:PMC3889271
28. Goldscheider C, Mosher WD. Patterns of contraceptive use in the United States: the importance of religious factors. Stud Fam Plann 1991; 22:102-15. https://doi.org/10.2307/1966780
PMid:1858103
29. Jacobs J, Stanfors M. Racial and ethnic differences in U.S. women's choice of reversible contraceptives, 1995-2010. Perspect Sex Reprod Health 2013; 45:139-47. https://doi.org/10.1363/4513913
PMid:24020775
30. Dehlendorf C, Park SY, Emeremni CA, et al. Racial/ethnic disparities in contraceptive use: variation by age and women's reproductive experiences. Am J Obstet Gynecol 2014; 210:526.e1-9. https://doi.org/10.1016/j.ajog.2014.01.037
PMid:24495671 PMCid:PMC4303233
31. Tang J, Maurer R, Bartz D. Intrauterine device knowledge and practices: a national survey of obstetrics and gynecology residents. South Med J 2013; 106:500-5. https://doi.org/10.1097/SMJ.0b013e3182a5ef0a
PMid:24002554
32. Stanwood NL, Garrett JM, Konrad TR. Obstetrician-gynecologists and the intrauterine device: a survey of attitudes and practice. Obstet Gynecol 2002; 99:275-80.
PMid:11814509
33. Moreau C, Bohet A, Hassoun D, Ringa V, Bajos N; FECOND group. IUD use in France: women's and physician's perspectives. Contraception 2014; 89:9-16. https://doi.org/10.1016/j.contraception.2013.10.003
PMid:24239330
34. Lewis C, Darney P, Thiel de Bocanegra H. Intrauterine contraception: impact of provider training on participant knowledge and provision. Contraception 2013; 88:226-31. https://doi.org/10.1016/j.contraception.2013.06.004
PMid:23845208
35. Lopez LM, Hiller JE, Grimes DA, Chen M. Education for contraceptive use by women after childbirth. Cochrane Database Syst Rev 2012; 8:CD001863. https://doi.org/10.1002/14651858.cd001863.pub3
36. Arrowsmith ME, Aicken CR, Saxena S, Majeed A. Strategies for improving the acceptability and acceptance of the copper intrauterine device. Cochrane Database Syst Rev 2012; 3:CD008896. https://doi.org/10.1002/14651858.cd008896.pub2
37. Lopez LM, Tolley EE, Grimes DA, Chen M, Stockton LL. Theory-based interventions for contraception. Cochrane Database Syst Rev 2013; 8:CD007249. https://doi.org/10.1002/14651858.cd007249.pub4
38. Lopez LM, Steiner M, Grimes DA, Hilgenberg D, Schulz KF. Strategies for communicating contraceptive effectiveness. Cochrane Database Syst Rev 2013; 4:CD006964. https://doi.org/10.1002/14651858.cd006964.pub3