Singapore Med J 2021; 62(9): 472-475 doi: 10.11622/smedj.2020047
Long-term effects of bariatric surgery on cardiovascular risk factors in Singapore
Vinay Panday1, MBBS, Asim Shabbir2, MMed, FRCS, Ivandito Kuntjoro3, MD, FAMS, Eric Yin Hao Khoo1, MBChB, MRCP, Jimmy Bok Yan So2,4, MBChB, FRCSEd, Kian Keong Poh3,4, MBBChir, FACC
Author Information >Copyright and License information >
1Department of Medicine, National University Health System, Singapore 2Department of Surgery, National University Hospital, Singapore 3Department of Cardiology, National University Heart Centre, National University Health System, Singapore 4NUS Yong Loo Lin School of Medicine, National University of Singapore, Singapore Correspondence: A/Prof Poh Kian Keong, Senior Consultant, Department of Cardiology, National University Heart Centre Singapore, National University Health System, 1E Kent Ridge Road, NUHS Tower Block, Level 9, Singapore 119228. kian_keong_poh@nuhs.edu.sg
Bariatric surgery is considered an effective treatment for weight loss and for improving the metabolic profile of patients with obesity. Obesity-related comorbidities such as hyperlipidaemia and type 2 diabetes mellitus (DM) are significant cardiovascular risk factors. Additionally, prospective clinical trials have shown that statins increase the risk of development of DM, and many patients with obesity are on statins. We retrospectively examined the effect of bariatric surgery on lipid profile, DM control and weight loss at the five-year follow-up.
METHODS
In total, 104 patients undergoing bariatric surgery from 2008 to 2012 were retrospectively studied. 36 patients were on preoperative statins. Their lipid profile, DM control and weight loss were examined at the one-year and five-year follow-ups.
RESULTS
Both high-density lipoprotein and triglyceride levels showed significant improvement at the one-year and five-year follow-ups (p = 0.01). Total cholesterol showed significant improvement at the one-year follow-up (−0.30 mmol/dL, p = 0.0338); however, better control was not sustained at the five-year follow-up (−0.15 mmol/dL, p = 0.133). Low-density lipoprotein did not show any considerable improvement at the one- and five-year follow-ups (−0.27 mmol/dL, p = 0.150 and −0.24 mmol/dL, p = 0.138, respectively). A statistically significant improvement in DM control was observed in these patients and in those on preoperative statins. Weight loss was sustained at one and five years.
CONCLUSION
Bariatric surgery does not confer a uniform improvement in lipid profile in the long term. It does, however, induce efficient weight loss and improvement in diabetic profile, even in patients on preoperative statins.
Keywords: bariatric surgery, cardiovascular risk factors, diabetes mellitus, lipids, long term
INTRODUCTION
Obesity is recognised as a global epidemic, with increasing incidence in recent years.(1-4) It is considered as a severe health hazard and a risk factor for chronic conditions such as Type 2 diabetes mellitus (DM), hypertension and hyperlipidaemia, as well as an established independent risk factor for cardiovascular diseases.(5,6) Bariatric procedures are reportedly the most effective strategy to reduce weight loss and have been demonstrated to be more effective than non-surgical means.(7,8) Many studies have documented the benefits of bariatric surgery in weight loss and its associated comorbidities. However, most of the studies are based on follow-up data of two years’ duration or less.(9) Studies on both the intermediate and long-term impact of bariatric surgery on hyperlipidaemia and its comorbidities are limited, especially in the Asian population.(10) We aimed to evaluate the impact of bariatric surgery on the lipid profile, glycaemic control and weight loss of patients with obesity at the five-year follow-up.
METHODS
Patients undergoing bariatric surgery from 2008 to 2012 at National University Hospital, Singapore, were evaluated for this study. Patients undergoing different types of bariatric surgery, including sleeve gastrectomy, gastric bypass and gastric banding were included. A total of 104 patients were enrolled, and their basic demography, preoperative statin use, lipid profile and DM status were recorded. Subsequently, lipid and glycaemic profile were evaluated at one- and five-year intervals. Some patients were lost to follow-up during the study period. At the one- and five-year intervals, 76 and 72 patients were evaluated, respectively. A subgroup of patients who were on statins preoperatively was also evaluated. This study was approved by the institutional ethics review board.
Statistical analysis was performed using the Stata 14 system (StataCorp, College Station, TX, USA). Continuous data was presented as median (interquartile range) if the variables followed a non-normal distribution. Categorical variables were expressed as percentage. The Wilcoxon signed-rank test for paired samples was employed as a non-parametric equivalent of the paired sample t-test used for continuous variables.
RESULTS
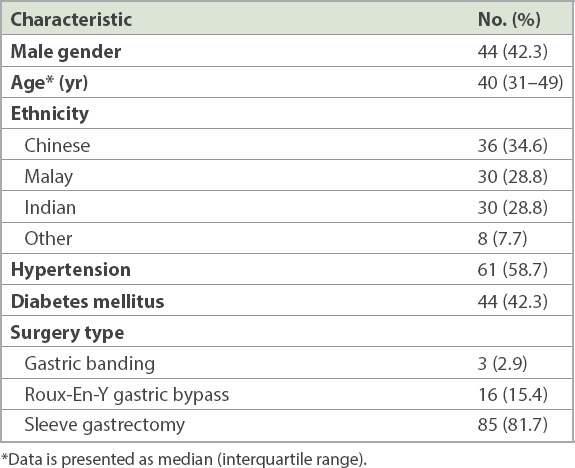
The demographic profile and comorbidities of our study population are presented in Table I. The patients had a median age of 40 years. They were predominantly of Chinese ethnicity (34.6%), and slightly over half of all patients were female. The most common associated comorbidity was hypertension (58.7%), followed by DM (42.3%). 34.2% of the patients were on statins preoperatively. The majority (81.7%) of the patients underwent sleeve gastrectomy. Gastric bypass surgery was the next most common surgery (15.4%), followed by gastric banding (2.9%).
Table I
Clinical and demographic characteristics of patients who underwent gastric banding, sleeve gastrectomy and Roux-en-Y gastric bypass (n = 104).
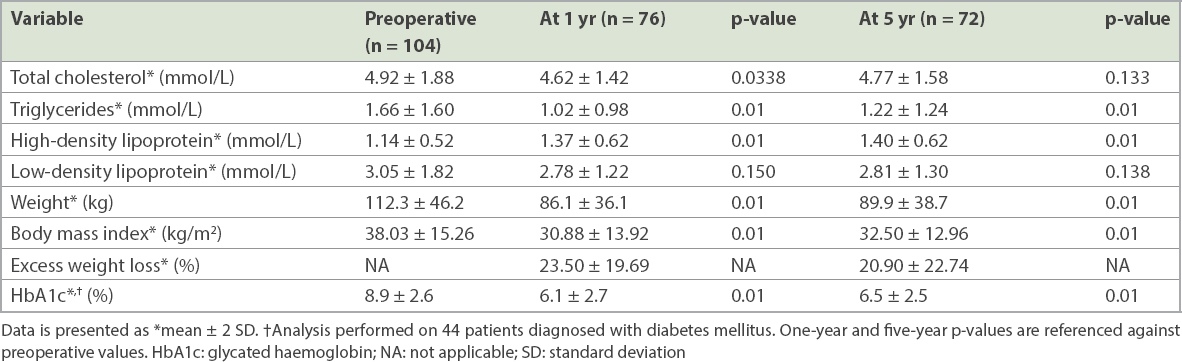
Changes in the lipid profile, glycaemic status and weight profile of our study population at baseline and at one- and five-year intervals are presented in Table II. Both high-density lipoprotein (HDL) and triglyceride (TG) levels showed significant improvement at the one- and five-year follow-ups. Total cholesterol (TC) showed significant improvement at the one-year follow-up (−0.30 mmol/dL, p = 0.0338); however, better control was not sustained at the five-year follow-up (−0.15 mmol/dL, p = 0.133). Low-density lipoprotein (LDL) did not improve at both the one-year and five-year follow-ups (−0.27 mmol/dL, p = 0.150 and −0.24 mmol/dL, p = 0.138, respectively).
Table II
Changes in metabolic profile at one year and five years after surgery.
Patients with DM experienced a significant improvement in glycaemic control. Weight loss was sustained at one-year and five-year intervals (−26.2 kg, p = 0.01 and −22.4 kg, p = 0.01, respectively), with a corresponding sustained improvement in body mass index. Percentage excess weight loss after surgery was 23.50% and 20.90% at the one-year and five-year time points, respectively.
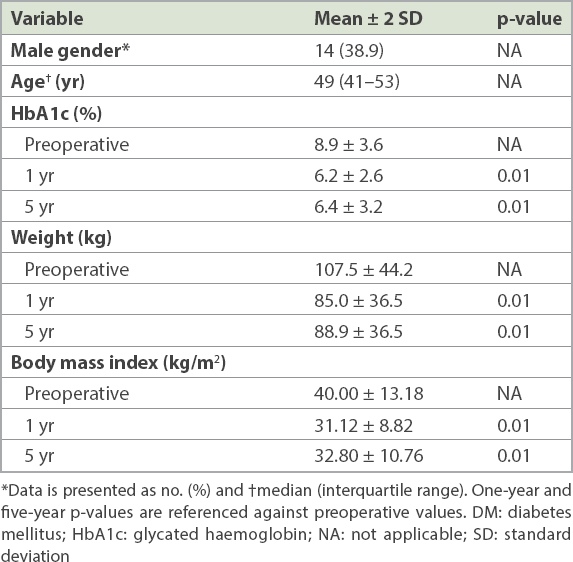
Table III details the profile of a subgroup of patients who were on statins preoperatively. This group had a median age of 49 years and was predominantly female (61.1%). Patients who were on preoperative statins showed significantly better DM control at one-year and five-year intervals (−2.7% HbA1c, p = 0.01 and −2.5% HbA1c, p = 0.01, respectively). Patients also had sustained weight loss at one-year and five-year intervals.
Table III
Demographic characteristics of patients on preoperative statins showing body weight and DM control at one year and five years after surgery (n = 36).
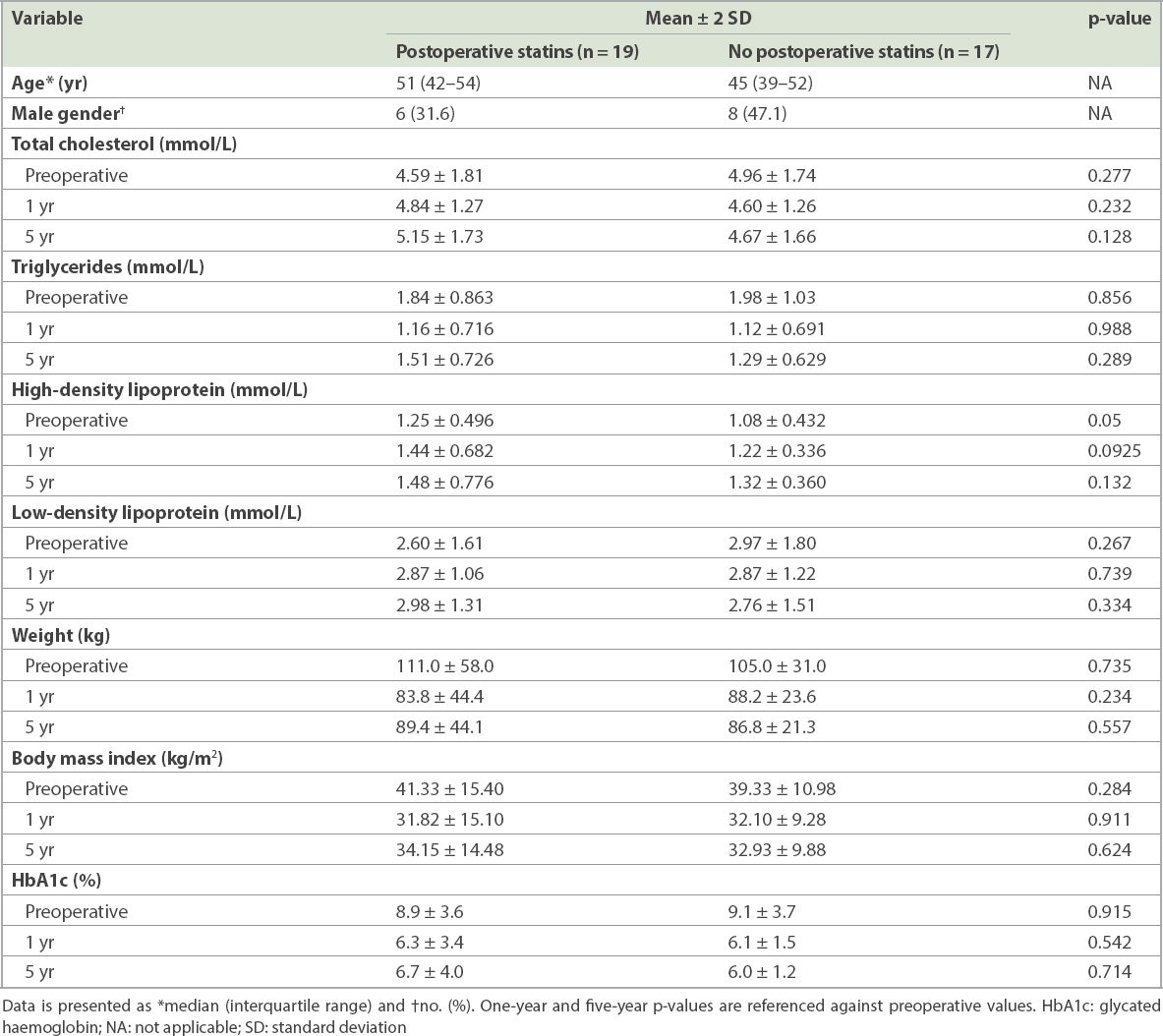
In the cohort of patients who were on preoperative statins, we further analysed the difference in the metabolic profile of patients who continued to be on statins postoperatively and those whose statins were discontinued after the operation (Table IV). No significant difference between the two cohorts was found in any component of lipid profile as well as DM profile and weight loss at the one- and five-year points. Additionally, no new onset of DM was noted in patients with preoperative statin use.
Table IV
Differences in the metabolic profiles of patients who were and were not on postoperative statins at one year and five years after surgery.
DISCUSSION
Limited data exists on whether bariatric surgery leads to a sustained improvement in the lipid profile of patients in the long term. In this retrospective analysis, we found that the improvement in lipid profile was not uniform. HDL and TG levels showed significant improvement, while TC and LDL did not show any improvement at the five-year follow-up. This trend in lipid profile following bariatric surgery has also been shown in other studies. An analysis of lipid profile after sleeve gastrectomy by Zhang et al reported that only HDL and TG levels improved significantly.(11) A meta-analysis of the impact of bariatric surgery on lipid profile also did not find significant improvement in TC.(9) One possible explanation is that the outcomes were procedure-related. The majority of our patients underwent sleeve gastrectomy, but Roux-En-Y gastric bypass (RYGB) has been shown to be more effective in lowering lipid level.(12,13) A study comparing the effect of RYGB with that of sleeve gastrectomy reported that RYGB reduced all lipid fractions, whereas LDL did not improve significantly in patients who underwent sleeve gastrectomy.(14)
The benefits of bariatric surgery on weight loss and glycaemic control have been studied,(15-18) and our results were consistent with the published literature: sustained weight loss and improved glycaemic control were observed at the one- and five-year intervals. The significant improvement in glycaemic level is attributed to a myriad of factors, including changes in absorption of metabolites after surgery and changes in gut-related hormones leading to increased insulin sensitivity and associated weight loss.(7)
Overall, our analysis points towards sustained and durable improvements in HDL and TG profile, glycaemic control and weight loss over a five-year duration. Our findings add to the growing body of evidence that improvements in metabolic comorbidities are indeed sustained over time. A recent study by Ikramuddin et al(19) demonstrated improvements in HbA1c, LDL and systolic blood pressure at five years after RYGB. Additionally, a recent seven-year analysis of health outcomes in the Longitudinal Assessment of Bariatric Surgery Study found durable improvements in all five comorbidities evaluated (DM, high LDL, high TG, low HDL and hypertension).(20) It is interesting to note that these two long-term studies examined patients who predominantly underwent RYGB, whereas our study population predominantly underwent sleeve gastrectomy. Hence, there seem to be sustained improvements across the different types of bariatric surgery.
Statins have been associated with increased risk of development of DM in prospective clinical trials,(21) which poses a higher risk to patients who undergo bariatric surgery, as many of them are on statins. However, in our analysis, patients who continued taking statins postoperatively and those for whom statins were discontinued showed similar improvements in glycaemic control. This improvement in glycaemia despite being on statin therapy is similar to the findings of Taylor et al, who reported that DM resolves with bariatric surgery more often in patients who are on preoperative statins.(22) Additionally, we found no significant worsening of the metabolic profile of patients who were continued on statins postoperatively compared with those whose statins were discontinued. Further, the improved metabolic profile leads to improved cardiovascular outcomes and, therefore, the cardioprotective benefits of bariatric surgery.(23-26)
One of the limitations of our study was the relatively small sample size. As such, it may be underpowered to determine an improvement in glycaemic control between patients who were continued on postoperative statins and those who were not. Additionally, we did not adjust for multiple variables that could have affected glycaemic control, such as weight loss, type of surgery affecting the absorption of metabolites and increased health consciousness of patients.
The strength of our study was that it described the metabolic profiles of patients in our local population who underwent bariatric surgery at a relatively long, five-year time point. Moreover, our study was one of the first to compare the metabolic profiles of patients who were continued on statins postoperatively with those whose statins were discontinued. Cardiovascular risk scores such as Reynolds and Framingham scores were not used to assess improvements in cardiovascular risk profiles owing to the younger age of our study population.
In conclusion, although studies detailing the short-term effects of bariatric surgery on obesity-related comorbidities have been reported, long-term data on its effect in the Asian population remains sparse. Our study demonstrated that bariatric surgery confers sustained weight loss and improved glycaemic control. However, it did not lead to a uniform improvement in lipid profile at the five-year follow-up. Clinicians should be mindful of the durable benefits of bariatric surgery and consider its use for patients with obesity who show suboptimal metabolic profiles.
About the First Author
Dr Vinay Bahadur Panday is currently a Senior Resident in the Department of Cardiology, National University Heart Centre, Singapore. Dr Vinay graduated with the degree of Bachelor of Medicine and Surgery from the National University of Singapore. He underwent an Internal Medicine residency in National University Hospital and was subsequently conferred Membership of the Royal College of Physicians (United Kingdom) and Masters of Medicine (Internal Medicine). He is interested in research in the fields of cardiovascular disease and health services delivery.
References Kinlen D, Cody D, O'Shea D. Complications of obesity.QJM. 2018;111:437-43. Eckersley RM. Losing the battle of the bulge:causes and consequences of increasing obesity.Med J Aust. 2001;174:590-2. Wilkinson KM. Increasing obesity in children and adolescents:an alarming epidemic.JAAPA. 2008;21:31-6. 38. Sturm R, Ringel JS, Andreyeva T. Increasing obesity rates and disability trends.Health Aff (Millwood). 2004;23:199-205. Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease:a 26-year follow-up of participants in the Framingham Heart Study.Circulation. 1983;67:968-77. Must A, Spadano J, Coakley EH, et al. The disease burden associated with overweight and obesity.JAMA. 1999;282:1523-9. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery:a systematic review and meta-analysis.JAMA. 2004;292:1724-37. Monteforte MJ, Turkelson CM. Bariatric surgery for morbid obesity.Obes Surg. 2000;10:391-401. Heffron SP, Parikh A, Volodarskiy A, et al. Changes in lipid profile of obese patients following contemporary bariatric surgery:a meta-analysis.Am J Med. 2016;129:952-9. Moustarah F, Gilbert A, Després JP, Tchernof A. Impact of gastrointestinal surgery on cardiometabolic risk.Curr Atheroscler Rep. 2012;14:588-96. Zhang F, Strain GW, Lei W, et al. Changes in lipid profiles in morbidly obese patients after laparoscopic sleeve gastrectomy (LSG).Obes Surg. 2011;21:305-9. Buchwald H, Varco RL, Matts JP, et al. Effect of partial ileal bypass surgery on mortality and morbidity from coronary heart disease in patients with hypercholesterolemia. Report of the Program on the Surgical Control of the Hyperlipidemias (POSCH).N Engl J Med. 1990;323:946-55. Gleysteen JJ. Results of surgery:long-term effects on hyperlipidemia.Am J Clin Nutr. 1992;55:2 Suppl591S-593S. Benaiges D, Flores-Le-Roux JA, Pedro-Botet J, et al. Impact of restrictive (sleeve gastrectomy) vs hybrid bariatric surgery (Roux-en-Y gastric bypass) on lipid profile.Obes Surg. 2012;22:1268-75. Seki Y, Kasama K, Haruta H, et al. Five-year-results of laparoscopic sleeve gastrectomy with duodenojejunal bypass for weight loss and type 2 diabetes mellitus.Obes Surg. 2017;27:795-801. Ersoz F, Duzkoylu Y, Deniz MM, Boz M. Laparoscopic Roux-en-Y gastric bypass with ileal transposition - an alternative surgical treatment for type 2 diabetes mellitus and gastroesophageal reflux.Wideochir Inne Tech Maloinwazyjne. 2015;10:481-5. Quan Y, Huang A, Ye M, et al. Efficacy of laparoscopic mini gastric bypass for obesity and type 2 diabetes mellitus:a systematic review and meta-analysis.Gastroenterol Res Pract. 2015;2015:152852. Lee PC, Tan HC, Pasupathy S, et al. Effectiveness of bariatric surgery in diabetes prevention in high-risk Asian individuals.Singapore Med J. 2018;59:472-5. Ikramuddin S, Korner J, Lee WJ, et al. Lifestyle intervention and medical management with vs without Roux-en-Y gastric bypass and control of hemoglobin A1c, LDL cholesterol, and systolic blood pressure at 5 years in the Diabetes Surgery Study.JAMA. 2018;319:266-78. Shubeck S, Dimick JB, Telem DA. Long-term outcomes following bariatric surgery.JAMA. 2018;319:302-3. Wang KL, Liu CJ, Chao TF, et al. Statins, risk of diabetes, and implications on outcomes in the general population.J Am Coll Cardiol. 2012;60:1231-8. Taylor BA, Ng J, Stone A, et al. Effects of statin therapy on weight loss and diabetes in bariatric patients.Surg Obes Relat Dis. 2017;13:674-80. Ashrafian H, le Roux CW, Darzi A, Athanasiou T. Effects of bariatric surgery on cardiovascular function.Circulation. 2008;118:2091-102. Kwok CS, Pradhan A, Khan MA, et al. Bariatric surgery and its impact on cardiovascular disease and mortality:a systematic review and meta-analysis.Int J Cardiol. 2014;173:20-8. Vest AR, Heneghan HM, Agarwal S, Schauer PR, Young JB. Bariatric surgery and cardiovascular outcomes:a systematic review.Heart. 2012;98:1763-77. Buchwald H, Estok R, Fahrbach K, Banel D, Sledge I. Trends in mortality in bariatric surgery:a systematic review and meta-analysis.Surgery. 2007;142:621-35.
4. Sturm R, Ringel JS, Andreyeva T. Increasing obesity rates and disability trends. Health Aff (Millwood) 2004; 23:199-205. https://doi.org/10.1377/hlthaff.23.2.199
PMid:15046144
5. Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation 1983; 67:968-77. https://doi.org/10.1161/01.CIR.67.5.968
PMid:6219830
6. Must A, Spadano J, Coakley EH, et al. The disease burden associated with overweight and obesity. JAMA 1999; 282:1523-9. https://doi.org/10.1001/jama.282.16.1523
PMid:10546691
7. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004; 292:1724-37. https://doi.org/10.1001/jama.292.14.1724
PMid:15479938
9. Heffron SP, Parikh A, Volodarskiy A, et al. Changes in lipid profile of obese patients following contemporary bariatric surgery: a meta-analysis. Am J Med 2016; 129:952-9. https://doi.org/10.1016/j.amjmed.2016.02.004
PMid:26899751 PMCid:PMC4988934
10. Moustarah F, Gilbert A, Després JP, Tchernof A. Impact of gastrointestinal surgery on cardiometabolic risk. Curr Atheroscler Rep 2012; 14:588-96. https://doi.org/10.1007/s11883-012-0288-2
PMid:23054664
11. Zhang F, Strain GW, Lei W, et al. Changes in lipid profiles in morbidly obese patients after laparoscopic sleeve gastrectomy (LSG). Obes Surg 2011; 21:305-9. https://doi.org/10.1007/s11695-010-0285-x
PMid:20859769
12. Buchwald H, Varco RL, Matts JP, et al. Effect of partial ileal bypass surgery on mortality and morbidity from coronary heart disease in patients with hypercholesterolemia. Report of the Program on the Surgical Control of the Hyperlipidemias (POSCH). N Engl J Med 1990; 323:946-55. https://doi.org/10.1056/NEJM199010043231404
PMid:2205799
13. Gleysteen JJ. Results of surgery: long-term effects on hyperlipidemia. Am J Clin Nutr 1992; 55(2 Suppl):591S-593S. https://doi.org/10.1093/ajcn/55.2.591s
PMid:1733134
14. Benaiges D, Flores-Le-Roux JA, Pedro-Botet J, et al. Impact of restrictive (sleeve gastrectomy) vs hybrid bariatric surgery (Roux-en-Y gastric bypass) on lipid profile. Obes Surg 2012; 22:1268-75. https://doi.org/10.1007/s11695-012-0662-8
PMid:22544352
15. Seki Y, Kasama K, Haruta H, et al. Five-year-results of laparoscopic sleeve gastrectomy with duodenojejunal bypass for weight loss and type 2 diabetes mellitus. Obes Surg 2017; 27:795-801. https://doi.org/10.1007/s11695-016-2372-0
PMid:27644433
16. Ersoz F, Duzkoylu Y, Deniz MM, Boz M. Laparoscopic Roux-en-Y gastric bypass with ileal transposition - an alternative surgical treatment for type 2 diabetes mellitus and gastroesophageal reflux. Wideochir Inne Tech Maloinwazyjne 2015; 10:481-5. https://doi.org/10.5114/wiitm.2015.54224
PMid:26649100 PMCid:PMC4653271
17. Quan Y, Huang A, Ye M, et al. Efficacy of laparoscopic mini gastric bypass for obesity and type 2 diabetes mellitus: a systematic review and meta-analysis. Gastroenterol Res Pract 2015; 2015:152852. https://doi.org/10.1155/2015/152852
PMid:26167173 PMCid:PMC4488176
18. Lee PC, Tan HC, Pasupathy S, et al. Effectiveness of bariatric surgery in diabetes prevention in high-risk Asian individuals. Singapore Med J 2018; 59:472-5. https://doi.org/10.11622/smedj.2018110
PMid:30310918 PMCid:PMC6158137
19. Ikramuddin S, Korner J, Lee WJ, et al. Lifestyle intervention and medical management with vs without Roux-en-Y gastric bypass and control of hemoglobin A1c, LDL cholesterol, and systolic blood pressure at 5 years in the Diabetes Surgery Study. JAMA 2018; 319:266-78. https://doi.org/10.1001/jama.2017.20813
PMid:29340678 PMCid:PMC5833547
20. Shubeck S, Dimick JB, Telem DA. Long-term outcomes following bariatric surgery. JAMA 2018; 319:302-3. https://doi.org/10.1001/jama.2017.20521
PMid:29340664
21. Wang KL, Liu CJ, Chao TF, et al. Statins, risk of diabetes, and implications on outcomes in the general population. J Am Coll Cardiol 2012; 60:1231-8. https://doi.org/10.1016/j.jacc.2012.05.019
PMid:22884288
22. Taylor BA, Ng J, Stone A, et al. Effects of statin therapy on weight loss and diabetes in bariatric patients. Surg Obes Relat Dis 2017; 13:674-80. https://doi.org/10.1016/j.soard.2016.11.018
PMid:28159561
23. Ashrafian H, le Roux CW, Darzi A, Athanasiou T. Effects of bariatric surgery on cardiovascular function. Circulation 2008; 118:2091-102. https://doi.org/10.1161/CIRCULATIONAHA.107.721027
PMid:19001033
24. Kwok CS, Pradhan A, Khan MA, et al. Bariatric surgery and its impact on cardiovascular disease and mortality: a systematic review and meta-analysis. Int J Cardiol 2014; 173:20-8. https://doi.org/10.1016/j.ijcard.2014.02.026
PMid:24636546
25. Vest AR, Heneghan HM, Agarwal S, Schauer PR, Young JB. Bariatric surgery and cardiovascular outcomes: a systematic review. Heart 2012; 98:1763-77. https://doi.org/10.1136/heartjnl-2012-301778
PMid:23077152
26. Buchwald H, Estok R, Fahrbach K, Banel D, Sledge I. Trends in mortality in bariatric surgery: a systematic review and meta-analysis. Surgery 2007; 142:621-35. https://doi.org/10.1016/j.surg.2007.07.018
PMid:17950357