Author Information >Copyright and License information >
1Department of Cardiology, Changi General Hospital, Singapore 2Care and Health Integration, Changi General Hospital, Singapore 3Family Medicine Academic Clinical Programme, SingHealth Duke-NUS Academic Medical Centre, Singapore Correspondence: Dr Huang Weiliang, Associate Consultant, Department of Cardiology, Changi General Hospital, 2 Simei Street 3, Singapore 529889. huang.weiliang@singhealth.com.sg
Mdm Teo Ah Mui, an 88-year-old woman, visited your clinic for her regular follow-up, as she had done for the past 20 years. She had just been discharged from the hospital after being admitted for an episode of heart failure last month. She asked about her new medications to protect her heart and regulate her fluid status, wanting to know if they were indeed good for her.
WHAT IS HEART FAILURE?
Heart failure (HF) is a clinical syndrome comprising signs and symptoms that result from a structural or functional cardiac abnormality, causing a compromise in cardiac output and/or elevated intracardiac filling pressures at rest or stress.(1) It is the result of any insult, such as coronary, valvular or arrhythmic, causing a disturbance to cardiac function.
HOW RELEVANT IS THIS TO MY PRACTICE?
HF is extremely prevalent in Singapore. About 20% of deaths in Singapore in 2017 were due to ischaemic heart disease and other cardiac diseases.(2) 4.5% of Singaporeans live with HF, compared to 1%–2% in the United States and Europe.
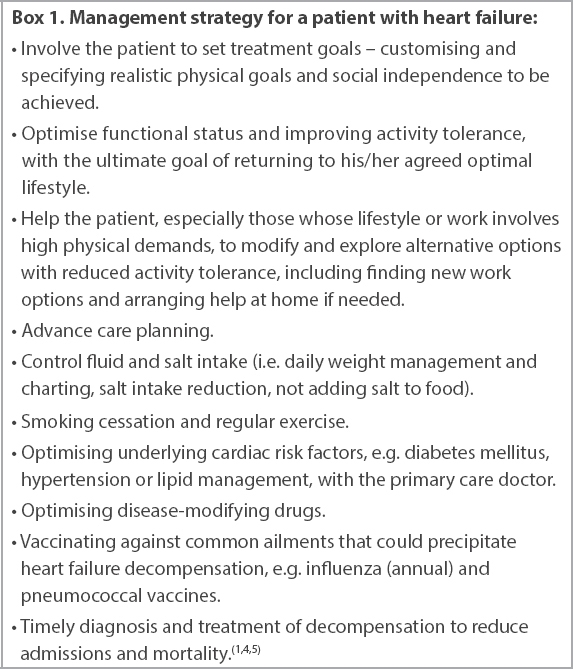
Many Singaporeans are also at risk of HF, with the most prevalent risk factors being insufficient physical activity (34% of the population), smoking (16%), obesity (35%), diabetes mellitus (10%) and hypertension (14%).(3) These risk factors need to be adequately controlled to minimise the chance of developing HF or, in the case of a HF patient, controlled to retard progression of HF. Management of HF requires the patient’s involvement and a multidisciplinary team approach (Box 1).
Box 1
Management strategy for a patient with heart failure:
Common signs and symptoms at presentation
The patient typically develops and presents with fluid overload, which causes dyspnoea, orthopnoea, jugular venous distension, pulmonary crepitations and ankle oedema.(1,6) When there is severely depressed cardiac output, there can be hypotension, cold extremities, decreased urine output and altered mentation when the cardiac output is unable to support adequate tissue perfusion.(1) These patients should be promptly referred to the accident and emergency department.
A medical history of cardiovascular disease or cardiovascular risk factors makes the diagnosis of HF more likely. All stable patients suspected to have newly diagnosed HF should have electrocardiography (ECG) performed and be referred to a cardiologist for early evaluation.
WHAT CAN I DO IN MY PRACTICE?
After diagnosis, the HF patient should ideally be managed in the community, with follow-up to ensure that the patient has few or no symptoms. Repeated hospitalisations for HF is a strong predictor of mortality.(7)
Patient self-care
Treatment goals should first be discussed and established with the patient, preferably with the support of caregivers and family members.
HF patients should restrict their salt and fluid intake, albeit to varying degrees based on the individual patient’s profile and severity of HF. They should be counselled on smoking cessation and avoidance of alcohol (especially for alcohol-related cardiac dysfunction), and screened for depression and managed accordingly.(8) Patients should also be taught self-care, symptom surveillance and weight monitoring, and advised to purchase a suitable water jug (e.g. 1-L jug) specifically for regulating water intake and a reliable weighing machine for daily weight measurements and recording. They should try as much as possible to comply with the fluid restrictions, and monitor themselves closely for symptoms such as ankle swelling if they exceed their restrictions on a hot day. Regular aerobic exercise should be encouraged to improve functional capacity and symptoms.(9)
Changes in functional status and/or a rapid gain in weight could herald decompensation. Early intervention, such as by temporarily increasing the diuretic dose, could restore equilibrium and avoid an admission to hospital.
HF patients who are unable to return to previous physically demanding work can be referred to Family Service Centres or Workforce Singapore Career Centres to find suitable employment.
Physician’s tasks
During a routine clinic visit, the physician should document effort tolerance (New York Heart Association [NYHA] class), review weight charts, assess blood pressure and examine the patient’s fluid status, as well as assess medication compliance and side effects. The primary care physician also needs to screen HF patients for depression, for which the Patient Health Questionnaire-9 is a useful tool.(8) HF patients should receive an annual influenza vaccination and a course of pneumococcal vaccination. Advance care planning, as well as work placement and financial help, should be discussed if required.
The dose of diuretics, usually oral frusemide, is patient-dependent (usually affected by cardiac and renal function) and, if required, can be increased temporarily to deal with decompensation episodes, such as doubling the dose for short periods with frequent re-assessment. Disease-modifying drugs for chronic HF are prescribed and titrated based on the patient’s left ventricular ejection fraction (LVEF). Patients are divided into HFrEF (HF with reduced ejection fraction < 40%), HFpEF (HF with preserved ejection fraction ≥ 50%) and HFmrEF (HF with mid-range ejection fraction 40%–49%) groups based on their LVEF on echocardiography.
HFrEF (HF with reduced ejection fraction < 40%)
While many evidence-based disease-modifying drugs are available for the treatment of chronic HF, HFrEF patients are notoriously undertreated.(3) An angiotensin-converting enzyme (ACE) inhibitor (or angiotensin receptor blocker [ARB])(10) and beta-blocker(11) are recommended for a patient with symptomatic (NYHA Class II–IV) HFrEF. A mineralocorticoid receptor antagonist(12) is recommended in symptomatic patients with LVEF ≤ 35%. These drugs should be administered at the target dose as long as the patient does not experience symptomatic hypotension (i.e. blood pressure remains > 90/60 mmHg). Starting at a lower dose with judicious up-titration could help encourage acceptance and minimise adverse drug effects. Should the patient still have HF symptoms, the ACE inhibitor (or ARB) can be replaced with an angiotensin receptor-neprilysin inhibitor (ARNI). The PARADIGM-HF trial showed that sacubitril/valsartan (an ARNI) is superior to enalapril in reducing morbidity and mortality in HFrEF patients.(13) Renal function, and in particular potassium levels, should be monitored 1–2 weeks after initiation or dosage change, then 3–6 monthly in patients on ACE-inhibitor/ARB/ARNI to ensure stability.
Beta-blockers are the first-line therapy in controlling the heart rate of a patient with chronic HFrEF. A target heart rate of 50–70 beats per minute (bpm) is advised. Adding an If-channel blocker is reasonable if the patient is in sinus rhythm and has a heart rate that is persistently > 70 bpm despite being on the maximum tolerated dose of beta-blocker.(14)
For diabetic patients with HFrEF, metformin(15) and a sodium-glucose cotransporter-2 (SGLT-2) inhibitor(16) should be included in their drug regimen. Both the EMPA-REG OUTCOME trial(17) and DECLARE-TIMI 58 trial(18) showed significant mortality and morbidity benefit of SGLT-2 inhibitors over placebo in HFrEF patients. However, thiazolidinediones,(19) saxagliptin,(20) nonsteroidal anti-inflammatory drugs and COX-2 inhibitors(21) are not recommended in HF patients.
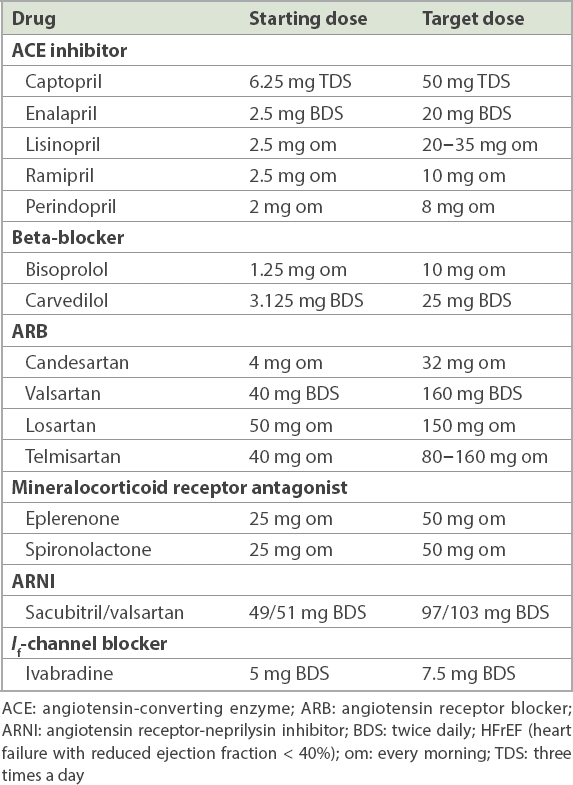
An automated implanted cardioverter-defibrillator device should be considered in patients with LVEF ≤ 35% and NYHA Class II–III after optimising medical therapy for prevention of sudden cardiac death.(22) Cardiac resynchronisation therapy should be considered in symptomatic patients who are in sinus rhythm, with left bundle branch block on ECG, who have QRS duration ≥ 150 ms and LVEF ≤ 35% despite optimal medical therapy.(23) Commonly used drugs for HFrEF are shown in Table I.
Table I
Commonly used drugs in HFrEF and their appropriate target doses.(1)
HFmrEF (HF with mid-range ejection fraction 40%–49%)
Patients with HFmrEF are a distinct group for whom there is currently no evidence-based medication to reduce mortality or morbidity. However, in the recent PARAGON-HF trial, the therapeutic benefits of ARNI vary by LVEF and appear to extend to HFmrEF patients, particularly for hospitalisation for HF.(24)
HFpEF (HF with preserved ejection fraction ≥ 50%)
HFpEF is on the rise in Southeast Asia due to the high prevalence of rapidly ageing societies and hypertension.(3) Compared to HFrEF, HFpEF patients tend to be older and female, have hypertension and atrial fibrillation, and less likely to have myocardial infarction.(25)
Currently, no specific pharmacological treatment has been shown to reduce mortality and morbidity in HFpEF patients. Several studies are ongoing. The current aim of treatment is to alleviate symptoms and improve quality of life, such as by prescribing diuretics to congested patients,(1,26) as well as aggressive control of comorbidities such as hypertension.
In conclusion, HF is a common problem in Singapore and requires a multidisciplinary approach. A combination of appropriate disease-modifying drugs, lifestyle modifications, and accessibility to care can help to reduce morbidity and hospitalisation rates.
TAKE HOME MESSAGES
Newly diagnosed, clinically stable HF patients require early specialist evaluation, while unstable or hypotensive patients need emergency attention.
Treatment goals should be discussed and agreed on with patients before being clearly documented in a care plan.
Decompensation should be detected early and treated with a temporary increase in diuretics.
Fluid and salt restrictions should be encouraged and enforced, with measurement of fluid intake and daily weight.
Smoking cessation and regular exercise should be encouraged.
Patients with HF should receive influenza and pneumococcal vaccines.
Patients can be screened for depression at clinic visits.
Diabetes mellitus, hypertension and lipid control should be optimised.
In patients with in HFrEF, disease-modifying drugs should be optimised to achieve appropriate target doses or at least maximally tolerated doses.
Patients should be encouraged to re-integrate into society with help from community resources.
USEFUL LINKS
Workforce Singapore: https://www.ssg-wsg.gov.sg (accessed April 16, 2020)
Advance care planning: https://www.livingmatters.sg (accessed April 16, 2020)
Family Service Centres: https://www.msf.gov.sg/dfcs/familyservice (accessed April 16, 2020)
Mdm Teo was happy to learn what her two new medications ‒ beta-blockers and ACE inhibitors – were for. Her domestic helper, Mary, would help to prepare a small 1-L water flask and monitor her fluid intake, chart her weight daily and remind her to take her medications. You also reminded Mary to chart Mdm Teo’s diet and drop by your clinic 2‒3 days later after her morning walk to hand her charts to your clinic assistants.
References Ponikowski P, Voors AA, Anker SD, et al. Authors/Task Force Members;Document Reviewers. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure:the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC.Eur J Heart Fail. 2016;18:891-975. Ministry of Health SingaporePrincipal Causes of Death. Available at: https://www.moh.gov.sg/resources-statistics/singapore-health-facts/principal-causes-of-death. Accessed April 15 2020. Lam CSP.Heart failure in Southeast Asia:facts and numbers.ESC Heart Failure. 2015;2:46-9. Cleland JG, Cohen-Solal A, Aguilar JC, et al. IMPROVEMENT of Heart Failure Programme Committees and Investigators. Improvement programme in evaluation and management;Study Group on Diagnosis of the Working Group on Heart Failure of The European Society of Cardiology. Management of heart failure in primary care (the IMPROVEMENT of Heart Failure Programme):an international survey.Lancet. 2002;360:1631-9. Feltner C, Jones CD, Cené CW, et al. Transitional care interventions to prevent readmissions for persons with heart failure:a systematic review and meta-analysis.Ann Int Med. 2014;160:774-84. Vijayakrishnan R, Steinhubl SR, Ng K, et al. Prevalence of heart failure signs and symptoms in a large primary care population identified through the use of text and data mining of the electronic health record.J Card Fail. 2014;20:459-64. Lin AH, Chin JC, Sicignano NM, Evans AM.Repeat hospitalisations predict mortality in patients with heart failure.Mil Med. 2017;182:e1932-e1937. National Institute for Health and Clinical Excellence Chronic heart failure:management of chronic heart failure in adults in primary and secondary care [online]NICE clinical guideline 108. Available at: http://www.wales.nhs.uk/sitesplus/documents/861/NICE%20Guidelines%20-%20Chronic%20Heart%20Failure.pdf.. Accessed April 15 2020. Ismail H, McFarlane JR, Nojoumian AH, Dieberg G, Smart NA.Clinical outcomes and cardiovascular responses to different exercise training intensities in patients with heart failure:a systematic review and meta-analysis.JACC Heart Fail. 2013;1:514-22. Garg R, Yusuf S.Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative Group on ACE Inhibitor Trials.JAMA. 1995;273:1450-6. Hjalmarson A, Goldstein S, Fagerberg B, et al. Effects of controlled-released metoprolol on total mortality, hospitalizations, and well-being in patients with heart failure:the Metoprolol CR/XL Randomized Intervention Trial in congestive heart failure (MERIT-HF). MERIT-HF Study Group.JAMA. 2000;283:1295-302. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators.N Engl J Med. 1999;341:709-17. McMurray JJ, Packer M, Desai AS, et al. PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure.N Engl J Med. 2014;371:993-1004. Swedberg K, Komajda M, Böhm M, et al. SHIFT Investigators. Ivabradine and outcomes in chronic heart failure (SHIFT):a randomised placebo-controlled study.Lancet. 2010;376:875-85. MacDonald MR, Each DT, Majumdar SR, et al. Treatment of type 2 diabetes and outcomes in patients with heart failure:a nested case-control study from the U.K. General Practice Research Database.Diabetes Care. 2010;33:1213-8. SeferovÄ PM, Petrie MC, Filippatos GS, et al. Type 2 diabetes mellitus and heart failure:a position statement from the Heart Failure Association of the European Society of Cardiology.Eur J Heart Fail. 2018;20:853-72. Zinman B, Wanner C, Lachin JM, et al. EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes.N Engl J M. 2015;373:2117-28. Wiviott SD, Raz I, Bonaca MP, et al. DECLARE–TIMI 58 Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes.N Engl J Med. 2019;380:347-57. Hernandez AV, Usmani A, Rajamanickam A, Moheet A.Thiazolidinediones and risk of heart failure in patients with or at high risk of type 2 diabetes mellitus:a meta-analysis and meta-regression analysis of placebo-controlled randomized clinical trials.Am J Cardiovasc Drugs. 2011;11:115-28. Scirica BM, Bhatt DL, Braunwald E, et al. SAVOR-TIMI 53 Steering Committee and Investigators. Saxagliptin and Cardiovascular Outcomes in Patients with type 2 diabetes mellitus.N Engl J Med. 2013;369:1317-26. Scott PA, Kingsley GH, Scott DL.Non-steroidal anti-inflammatory drugs and cardiac failure:meta-analyses of observational studies and randomised controlled trials.Eur J Heart Fail. 2008;10:1102-7. Theuns DA, Smith T, Hunink MG, Bardy GH, Jordaens L.Effectiveness of prophylactic implantation of cardioverter-defibrillators without cardiac resynchronization therapy in patients with ischaemic or non-ischaemic heart disease:a systematic review and meta-analysis.Europace. 2010;12:1564-70. Cleland JG, Daubert JC, Erdmann E, et al. Owan TE, Hodge DO, Herges RM, et al. Cardiac Resynchronization-Heart Failure (CARE-HF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. Trends in prevalence and outcome of heart failure with preserved ejection fraction. Trends in prevalence and outcome of heart failure with preserved ejection fraction.N Engl J Med. 2005;352:1539-49. 2006; 355:251-9. Solomon SD, Vaduganathan M, L Claggett B, et al. Sacubitril/valsartan across the spectrum of ejection fraction in heart failure.Circulation. 2020;141:352-61. Owan TE, Hodge DO, Herges RM, et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction.N Engl J Med. 2006;355:251-9. Lewis EF, Lamas GA, O'Meara E, et al. CHARM Investigators. Characterization of health-related quality of life in heart failure patients with preserved versus low ejection fraction in CHARM.Eur J Heart Fail. 2007;9:83-91.
REFERENCES:
1. Ponikowski P, Voors AA, Anker SD, et al; Authors/Task Force Members; Document Reviewers. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016; 18:891-975. https://doi.org/10.1002/ejhf.592
PMid:27207191
3. Lam CSP. Heart failure in Southeast Asia: facts and numbers. ESC Heart Failure 2015; 2:46-9. https://doi.org/10.1002/ehf2.12036
PMid:28834655 PMCid:PMC6410537
4. Cleland JG, Cohen-Solal A, Aguilar JC, et al; IMPROVEMENT of Heart Failure Programme Committees and Investigators. Improvement programme in evaluation and management; Study Group on Diagnosis of the Working Group on Heart Failure of The European Society of Cardiology. Management of heart failure in primary care (the IMPROVEMENT of Heart Failure Programme): an international survey. Lancet 2002; 360:1631-9. https://doi.org/10.1016/S0140-6736(02)11601-1
5. Feltner C, Jones CD, Cené CW, et al. Transitional care interventions to prevent readmissions for persons with heart failure: a systematic review and meta-analysis. Ann Int Med 2014; 160:774-84. https://doi.org/10.7326/M14-0083
PMid:24862840
6. Vijayakrishnan R, Steinhubl SR, Ng K, et al. Prevalence of heart failure signs and symptoms in a large primary care population identified through the use of text and data mining of the electronic health record. J Card Fail 2014; 20:459-64. https://doi.org/10.1016/j.cardfail.2014.03.008
PMid:24709663 PMCid:PMC4083004
7. Lin AH, Chin JC, Sicignano NM, Evans AM. Repeat hospitalisations predict mortality in patients with heart failure. Mil Med 2017; 182:e1932-e1937. https://doi.org/10.7205/MILMED-D-17-00017
PMid:28885958
8. National Institute for Health and Clinical Excellence Chronic heart failure: management of chronic heart failure in adults in primary and secondary care [online]. NICE clinical guideline 108. Available at: http://www.wales.nhs.uk/ sitesplus/documents/861/NICE%20Guidelines%20-%20Chronic%20Heart%20 Failure.pdf. Accessed April 15, 2020.
9. Ismail H, McFarlane JR, Nojoumian AH, Dieberg G, Smart NA. Clinical outcomes and cardiovascular responses to different exercise training intensities in patients with heart failure: a systematic review and meta-analysis. JACC Heart Fail 2013; 1:514-22. https://doi.org/10.1016/j.jchf.2013.08.006
PMid:24622004
10. Garg R, Yusuf S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative Group on ACE Inhibitor Trials. JAMA 1995; 273:1450-6. https://doi.org/10.1001/jama.1995.03520420066040
PMid:7654275
11. Hjalmarson A, Goldstein S, Fagerberg B, et al. Effects of controlled-released metoprolol on total mortality, hospitalizations, and well-being in patients with heart failure: the Metoprolol CR/XL Randomized Intervention Trial in congestive heart failure (MERIT-HF). MERIT-HF Study Group. JAMA 2000; 283:1295-302. https://doi.org/10.1001/jama.283.10.1295
PMid:10714728
12. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999; 341:709-17. https://doi.org/10.1056/NEJM199909023411001
PMid:10471456
13. McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014; 371:993-1004. https://doi.org/10.1056/NEJMoa1409077
PMid:25176015
14. Swedberg K, Komajda M, Böhm M, et al; SHIFT Investigators. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet 2010; 376:875-85. https://doi.org/10.1016/S0140-6736(10)61198-1
15. MacDonald MR, Eurich DT, Majumdar SR, et al. Treatment of type 2 diabetes and outcomes in patients with heart failure: a nested case-control study from the U.K. General Practice Research Database. Diabetes Care 2010; 33:1213-8. https://doi.org/10.2337/dc09-2227
PMid:20299488 PMCid:PMC2875425
16. Seferovć PM, Petrie MC, Filippatos GS, et al. Type 2 diabetes mellitus and heart failure: a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2018; 20:853-72. https://doi.org/10.1002/ejhf.1170
PMid:29520964
17. Zinman B, Wanner C, Lachin JM, et al; EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J M 2015; 373:2117-28. https://doi.org/10.1056/NEJMoa1504720
PMid:26378978
18. Wiviott SD, Raz I, Bonaca MP, et al; DECLARE-TIMI 58 Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019; 380:347-57. https://doi.org/10.1056/NEJMoa1812389
PMid:30415602
19. Hernandez AV, Usmani A, Rajamanickam A, Moheet A. Thiazolidinediones and risk of heart failure in patients with or at high risk of type 2 diabetes mellitus: a meta-analysis and meta-regression analysis of placebo-controlled randomized clinical trials. Am J Cardiovasc Drugs 2011; 11:115-28. https://doi.org/10.2165/11587580-000000000-00000
PMid:21294599
20. Scirica BM, Bhatt DL, Braunwald E, et al; SAVOR-TIMI 53 Steering Committee and Investigators. Saxagliptin and Cardiovascular Outcomes in Patients with type 2 diabetes mellitus. N Engl J Med 2013; 369:1317-26. https://doi.org/10.1056/NEJMoa1307684
PMid:23992601
21. Scott PA, Kingsley GH, Scott DL. Non-steroidal anti-inflammatory drugs and cardiac failure: meta-analyses of observational studies and randomised controlled trials. Eur J Heart Fail 2008; 10:1102-7. https://doi.org/10.1016/j.ejheart.2008.07.013
PMid:18760966
22. Theuns DA, Smith T, Hunink MG, Bardy GH, Jordaens L. Effectiveness of prophylactic implantation of cardioverter-defibrillators without cardiac resynchronization therapy in patients with ischaemic or non-ischaemic heart disease: a systematic review and meta-analysis. Europace 2010; 12:1564-70. https://doi.org/10.1093/europace/euq329
PMid:20974768 PMCid:PMC2963481
23. Cleland JG, Daubert JC, Erdmann E, et al; Cardiac Resynchronization-Heart Failure (CARE-HF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med 2005; 352:1539-49. Owan TE, Hodge DO, Herges RM, et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006; 355:251-9. https://doi.org/10.1056/NEJMoa052256
PMid:16855265
24. Solomon SD, Vaduganathan M, L Claggett B, et al. Sacubitril/valsartan across the spectrum of ejection fraction in heart failure. Circulation 2020; 141:352-61. https://doi.org/10.1161/CIRCULATIONAHA.119.044586
PMid:31736342
25. Owan TE, Hodge DO, Herges RM, et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006; 355:251-9. https://doi.org/10.1056/NEJMoa052256
PMid:16855265
26. Lewis EF, Lamas GA, O'Meara E, et al; CHARM Investigators. Characterization of health-related quality of life in heart failure patients with preserved versus low ejection fraction in CHARM. Eur J Heart Fail 2007; 9:83-91. https://doi.org/10.1016/j.ejheart.2006.10.012
PMid:17188020