Wolff-Parkinson-White (WPW) syndrome is characterised by the presence of an accessory pathway with typical electrocardiography (ECG) changes of short PR interval, slurred delta wave and widened QRS complexes. In WPW Type A, the presence of Q wave and Q/T vector discordance in inferior leads can simulate inferior infarction; at the same time, WPW syndrome can also mask the ECG changes of ST elevation myocardial infarction.(1) We herein report a case of a 63-year-old man with no known illness presenting with acute chest pain of six hours’ duration.
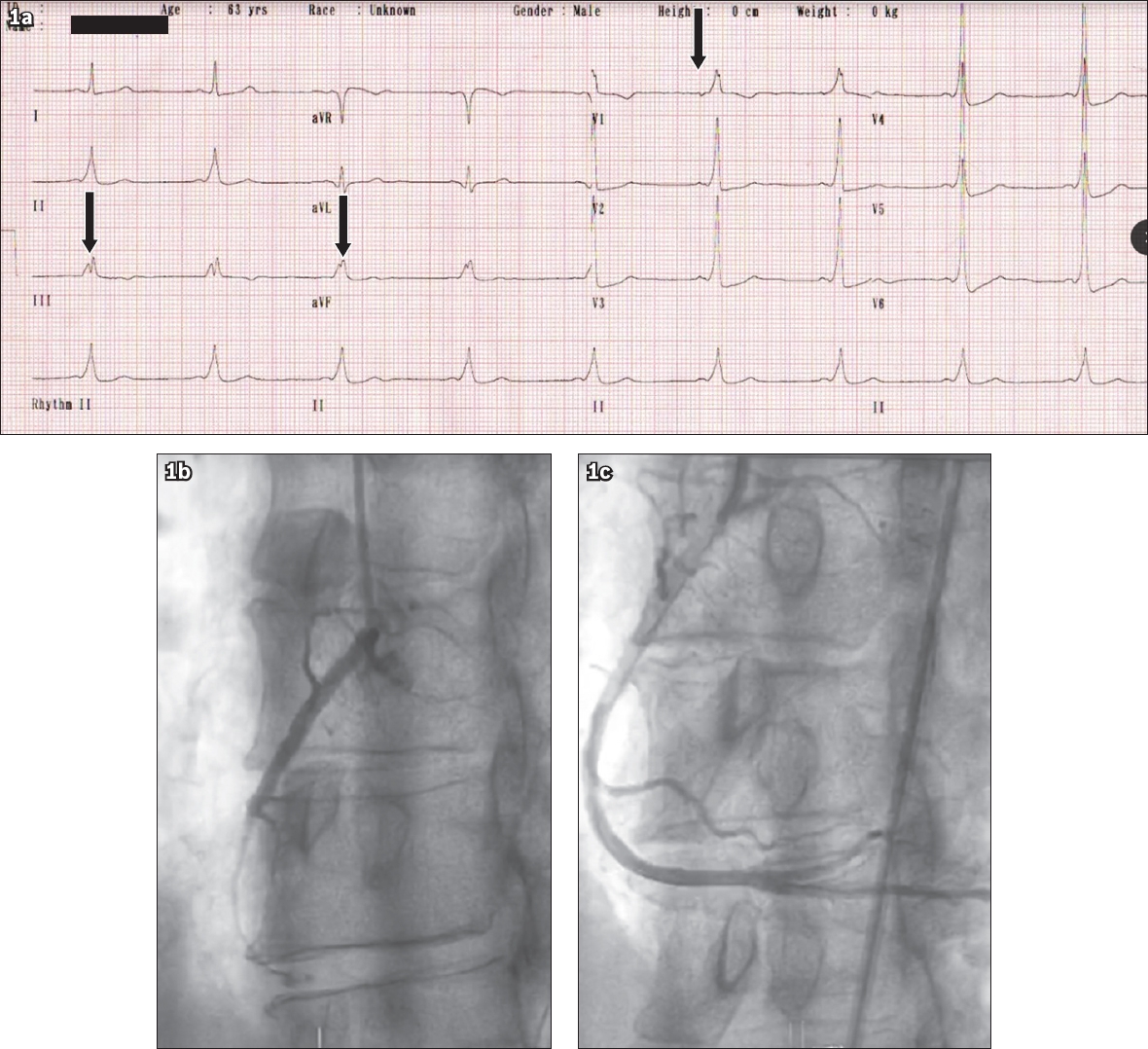
ECG showed the presence of WPW Type A (left accessory pathway) with no overt ST changes associated with infarction (Fig. 1a). However, fragmented QRS complexes (fQRS; arrows, Fig. 1a) and Q/T vector concordance were seen in inferior leads. Cardiac troponin T was elevated, confirming myocardial damage. Transthoracic echocardiogram showed preserved ejection fraction of 62% using the biplane Simpson’s method. Immediate coronary angiography was performed as the patient had persistent pain, showing an occluded right coronary artery (Fig. 1b). Percutaneous coronary intervention was done and the right coronary artery was stented with a drug-eluting stent, with a good angiographic result (Fig. 1c). The patient was discharged three days later with dual antiplatelet drugs (aspirin and ticagrelor).
Fig. 1
(a) ECG shows Wolff-Parkinson-White features in leads III and aVF, fragmented QRS complexes (black arrows) and Q/T vector concordance. Coronary angiograms show the (b) occluded and (c) post-stenting right coronary artery.
The delta wave in WPW syndrome can simulate inferior infarction by producing pseudo-infarct Q waves in leads II, III and AVF. Goldberger(2) has suggested that a discordant T wave (opposite the Q wave) should be the norm in WPW Type A; however, if inferior infarction is suspected, the T wave should be concordant.(2) A lesser-known fact is that WPW syndrome can also mask the ECG changes of inferior myocardial infarction, as the delta wave vector will oppose and obliterate the initial vectors of infarction, producing a normal-looking ECG.(3) In our case, the subtle signs pointing to an ongoing infarction in Fig. 1a were concordant upright T wave(2) and fragmentation of the QRS complexes in leads III and aVF (Fig. 2).
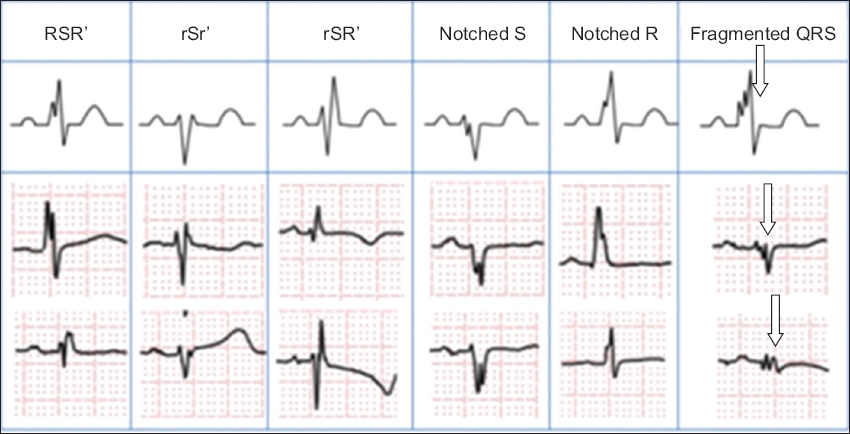
Fig. 2
Diagram shows different patterns of RSR and fragmented QRS complexes (white arrows).
Das et al defined fQRS as QRS complexes with the presence of an additional R wave (R’) or notching in the nadir of the R or S wave, or the presence of > 1 R’ (fragmentation) in two contiguous leads, corresponding to a major coronary territory (Fig. 1d).(3) fQRS represent distortion of the intraventricular conduction secondary to myocardial scarring and fibrosis. The zigzag conduction through these scarred tissue results in spikes in the QRS complexes (arrows, Fig. 2).(4) In acute coronary syndrome, fQRS appear within 24 hours from the onset of symptoms and persist thereafter. This has been reported in 55% of patients with ST elevation myocardial infarction and 50% of patients with non-ST elevation myocardial infarction, but in only 3.7% of patients with unstable angina pectoris.(5) The specificity of fQRS for infarction was 96%. In multivariate analysis, the presence of fQRS was a better independent predictor for all-cause mortality than Q waves (hazard ratio 1.68 vs. 1.47).(5)
In conclusion, this case illustrates how ST segment elevation acute myocardial infarction can be masked in patients with pre-existing WPW syndrome. However, comprehensive analysis of the ST-T wave concordance and fragmentation of the QRS complexes helped us to spot the infarction and identify the infarct-related artery.
Yours sincerely,
References Schamroth L, Lapinsky GB. The Wolff-Parkinson-White syndrome associated with myocardial infarction and right bundle branch block.J Electrocardiol. 1972;5:299-305. Goldberger AL. Pseudo-infarct patterns in the Wolff-Parkinson-White syndrome: importance of Q wave-T wave vector discordance.J Electrocardiol. 1980;13:115-8. Das MK, Khan B, Jacob S, Kumar A, Mahenthiran J. Significance of a fragmented QRS complex versus a Q wave in patients with coronary artery disease.Circulation. 2006;113:2495-501. Take Y, Morita H. Fragmented QRS: what is the meaning?.Indian Pacing Electrophysiol J. 2012;12:213-5. Das MK, Michael MA, Suradi H, et al. Usefulness of fragmented QRS on a 12-lead electrocardiogram in acute coronary syndrome for predicting mortality.Am J Cardiol. 2009;104:1631-7.
REFERENCES:
1. Schamroth L, Lapinsky GB. The Wolff-Parkinson-White syndrome associated with myocardial infarction and right bundle branch block. J Electrocardiol 1972; 5:299-305. https://doi.org/10.1016/S0022-0736(72)80012-8
2. Goldberger AL. Pseudo-infarct patterns in the Wolff-Parkinson-White syndrome: importance of Q wave-T wave vector discordance. J Electrocardiol 1980; 13:115-8. https://doi.org/10.1016/S0022-0736(80)80041-0
3. Das MK, Khan B, Jacob S, Kumar A, Mahenthiran J. Significance of a fragmented QRS complex versus a Q wave in patients with coronary artery disease. Circulation 2006; 113:2495-501. https://doi.org/10.1161/CIRCULATIONAHA.105.595892
PMid:16717150
5. Das MK, Michael MA, Suradi H, et al. Usefulness of fragmented QRS on a 12-lead electrocardiogram in acute coronary syndrome for predicting mortality. Am J Cardiol 2009; 104:1631-7. https://doi.org/10.1016/j.amjcard.2009.07.046
PMid:19962466