Singapore Med J 2017; 58(7): 438-445 doi: 10.11622/smedj.2017072
Measuring the effectiveness of a novel CPRcard™ feedback device during simulated chest compressions by non-healthcare workers
Alexander E White1, JD, MPH, Han Xian Ng2, MBBS, Wai Yee Ng3, BSc, Eileen Kai Xin Ng1, BN, Stephanie Fook-Chong3,4, MSc, CStat, Phek Hui Jade Kua5, MBBS, MRCSE, Marcus Eng Hock Ong6,7, MBBS, MPH
Author Information >Copyright and License information >
1Unit for Prehospital Emergency Care, Singapore General Hospital, Singapore 2Barts and the London School of Medicine and Dentistry, United Kingdom 3Health Services Research, Division of Research, Singapore General Hospital, Singapore 4Centre for Quantitative Medicine, Duke-NUS Medical School, Singapore 5Department of Emergency Medicine, KK Women’s and Children’s Hospital, Singapore 6Department of Emergency Medicine, Singapore General Hospital, Singapore 7Health Services and Systems Research, Duke-NUS Medical School, Singapore Correspondence: Mr Alexander E White, Co-investigator, Policy and Research Group Lead, Unit for Prehospital Emergency Care, Singapore General Hospital, 226 Outram Road, Singapore 169039. alexander.elgin.white@sgh.com.sg
There is a need for a simple-to-use and easy-to-carry CPR feedback device for laypersons. We aimed to determine if a novel CPRcard™ feedback device improved the quality of chest compressions.
METHODS
We compared participants’ chest compression rate and depth with and without feedback. Compression data was captured through the CPRcard™ or Resusci Anne’s SimPad® SkillReporter™. Compression quality was defined based on 2010 international guidelines for rate, depth and flow fraction.
RESULTS
Overall, the CPRcard group achieved a better median compression rate (CPRcard 117 vs. control 122, p = 0.001) and proportion of compressions within the adequate rate range (CPRcard 83% vs. control 47%, p < 0.001). Compared to the no-card and blinded-card groups, the CPRcard group had a higher proportion of adequate compression rate (CPRcard 88% vs. no-card 46.8%, p = 0.037; CPRcard 73% vs. blinded-card 43%, p = 0.003). Proportion of compressions with adequate depth was similar in all groups (CPRcard 52% vs. control 48%, p = 0.957). The CPRcard group more often met targets for compression rate of 100–120/min and depth of at least 5 cm (CPRcard 36% vs. control 4%, p = 0.022). Chest compression flow fraction rate was similar but not statistically significant in all groups (92%, p = 1.0). Respondents using the CPRcard expressed higher confidence (mean 2.7 ± 2.4; 1 = very confident, 10 = not confident).
CONCLUSION
Use of the CPRcard by non-healthcare workers in simulated resuscitation improved the quality of chest compressions, thus boosting user confidence in performing compressions.
Studies of innovative cardiopulmonary resuscitation (CPR) feedback devices have shown promising results.(1-8) However, at least one study has highlighted the potential problems of reliance on devices, and another study has concluded that there was no benefit derived among trained responders.(9,10) In these studies, the feedback devices were attached to an automated external defibrillator (AED) or paired with a phone application; some were also hospital-based and could not be readily carried around by laymen. Also, in many of these studies, mixed results were observed in the CPR performance of healthcare workers or experienced life-savers.(11) Therefore, there is a need for a simple-to-use and easy-to-carry CPR feedback device for laypersons. Such a device could possibly improve the quality of bystander CPR.
The present study was nested in a community-based Dispatcher-Assisted first REsponder (DARE) training initiative, which simulates a rescuer-dispatcher sequence that is initiated by a call to Singapore’s emergency medical service (EMS). Dispatchers who suspect a cardiac arrest then coach the caller to perform CPR until an ambulance crew arrives. Singapore’s largely urban setting presents multiple challenges for EMS response. An ambulance takes an average of 11 minutes to arrive at the scene (less than 11 minutes in 85% of cases in 2015).(12) Since most collapses in Singapore occur at home in high-rise buildings, paramedics must also contend with vertical travel time. These challenges make it all the more important for bystanders to perform CPR while waiting for the arrival of the EMS.
The DARE training programme teaches compression-only CPR. Conventional standards for quality CPR entail adequate depth and rate of compressions with minimal pauses to provide rescue breaths. The quality and timeliness of compressions is vital to survival and good neurological outcomes.(13-17) Several studies comparing conventional CPR with compression-only CPR have found that the compression-only approach results in equal or slightly better outcomes.(18-20) When designing DARE, we asked ourselves the question, “Practically, what will lay rescuers remember and perform in an emergency?” We then aimed to train laypeople on what is effective, simple to remember and presents a lower risk of delaying a response.(20-24)
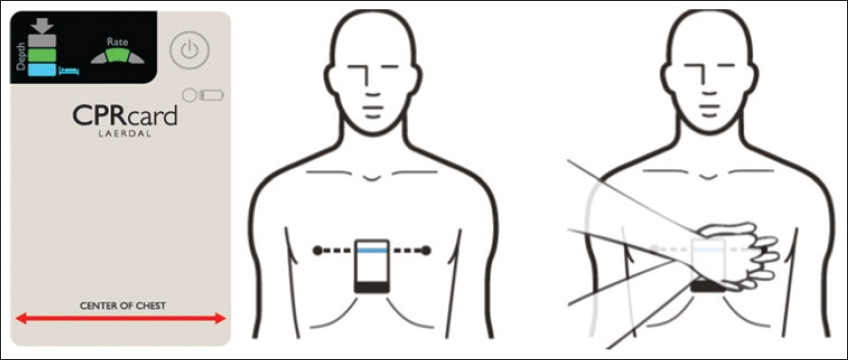
In this study, we provided each participant with a novel CPR feedback device, CPRcard™ (Laerdal Medical, Stavanger, Norway). The CPRcard has the look and feel of a typical credit card (55 mm × 85 mm × 1 mm) and contains a built-in accelerometer (Fig. 1).(6) It provides real-time visual feedback on compression rate and depth through two meters displayed on the card. By watching the displays, one can regulate the rate and depth of compressions to achieve and sustain good quality compressions. Administering chest compressions aided by feedback should, theoretically, help the lay responder consistently perform better quality chest compressions compared to compressions done without feedback. Our goal was to observe whether laypersons using this novel feedback device for the first time during their training would indeed perform better quality chest compressions.
Fig. 1
Image shows the CPRcard and its placement during compression.
METHODS
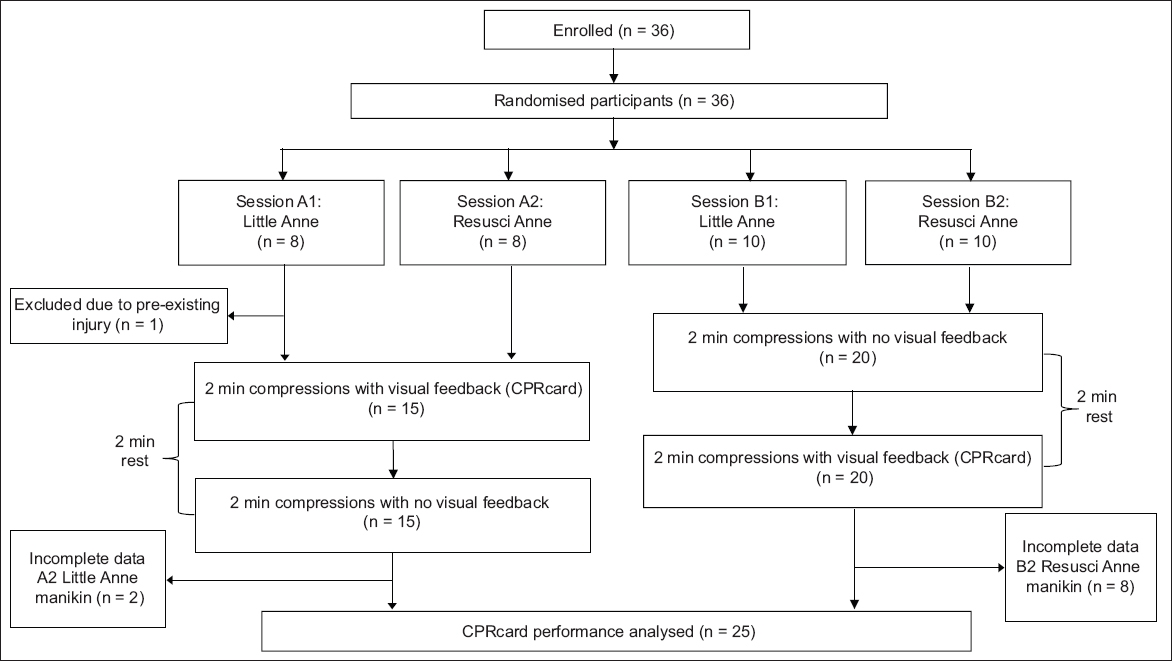
In this prospective observational study, teachers from a local junior college were selected to participate. They were randomly selected to be trained at the school on a specific day, and each participant was then scheduled to attend one of two training sessions. The two training sessions differed in that one group started with feedback, while the other group started without. After a short two-minute break, each of the two arms crossed over and performed compressions under opposite conditions. For example, the group that started the first round with feedback did their second round without feedback. Fig. 2 shows the selection of participants and the training sequence.
Fig. 2
Flowchart shows the selection of participants and training sequence.
To assess the compression quality of CPR, we provided each participant with one CPRcard. Participants performed compressions on either the Resusci Anne® or Little Anne® manikins (Laerdal Medical, Stavanger, Norway). The CPRcard collected real-time performance data for all cases, except for the no-card, no-feedback study arm, which used Resusci Anne’s telemetry to record and assess compression quality.
The CPRcard feedback was calibrated to 2010 international guidelines for compression rate and depth. This was the standard extant at the time the study was conducted. The newly promulgated 2015 international guidelines define the parameters of quality CPR as: compression depth 5–6 cm; compression rate 100–120 per minute; compression flow fraction at least 60%; full chest recoil; and non-excessive ventilations.(25-27) The 2016 Singapore evidence-based standard varies only in the depth metric with a new standard of 4–6 cm.
Chest compression data was downloaded and calculated for the CPRcard group and the blinded-card control group. All chest compression performances were evaluated based on seven variables: (a) mean compression rate (i.e. mean number of compressions per minute); (b) mean compression depth in cm; (c) adequate compression rate (percentage of total compressions that were within the optimal 100–120 compressions per minute range); (d) adequate compression depth (percentage of total compressions that were ≥ 5 cm); (e) mean pause length in seconds (pauses are defined as ≥ 3 seconds of no compressions); (f) adequate flow fraction > 80% (flow fraction rate is the percentage of time when chest compressions are being performed without ≥ 3-second pause); and (g) adequate compression rate and depth combined (%).
Frequencies and percentages were used to describe elements of the participants’ profile. The primary outcome – whether participants met targets for both compression rate (100–120 per minute) and depth (at least 5 cm) – was compared between the CPRcard group and control group using McNemar’s test. We also compared the outcome between the two control groups performing compressions on the Little Anne (blinded-card) and Resusci Anne (no-card) manikins. We analysed other CPR parameters using Wilcoxon signed-rank test, as the distribution of the parameters was skewed. Medians and interquartile ranges were also calculated. McNemar’s test was used for categorical variables. These CPR parameters were compared among the overall CPRcard group and the two control groups.
McNemar’s test was used to compare the proportion of correct answers for CPR and AED knowledge between pre- and post-training surveys. Descriptive statistics (such as mean, median, standard deviation, minimum and maximum) were calculated to determine the participants’ attitude toward and experience with using the CPRcard. This was measured using the Likert point scale score, where a lower number indicated a better experience. A two-tailed p-value < 0.05 was considered statistically significant. Analyses were completed using the STATA 13.0 statistical software package (StataCorp, College Station, TX, USA) with alpha set at 0.05. Study data was managed using REDCap (Research Electronic Data Capture, Vanderbilt University, Nashville, TN, USA), which was hosted at Singapore General Hospital. This study was conducted with the approval of the SingHealth Centralised Institutional Review Board (CIRB reference #2015/2475).
RESULTS
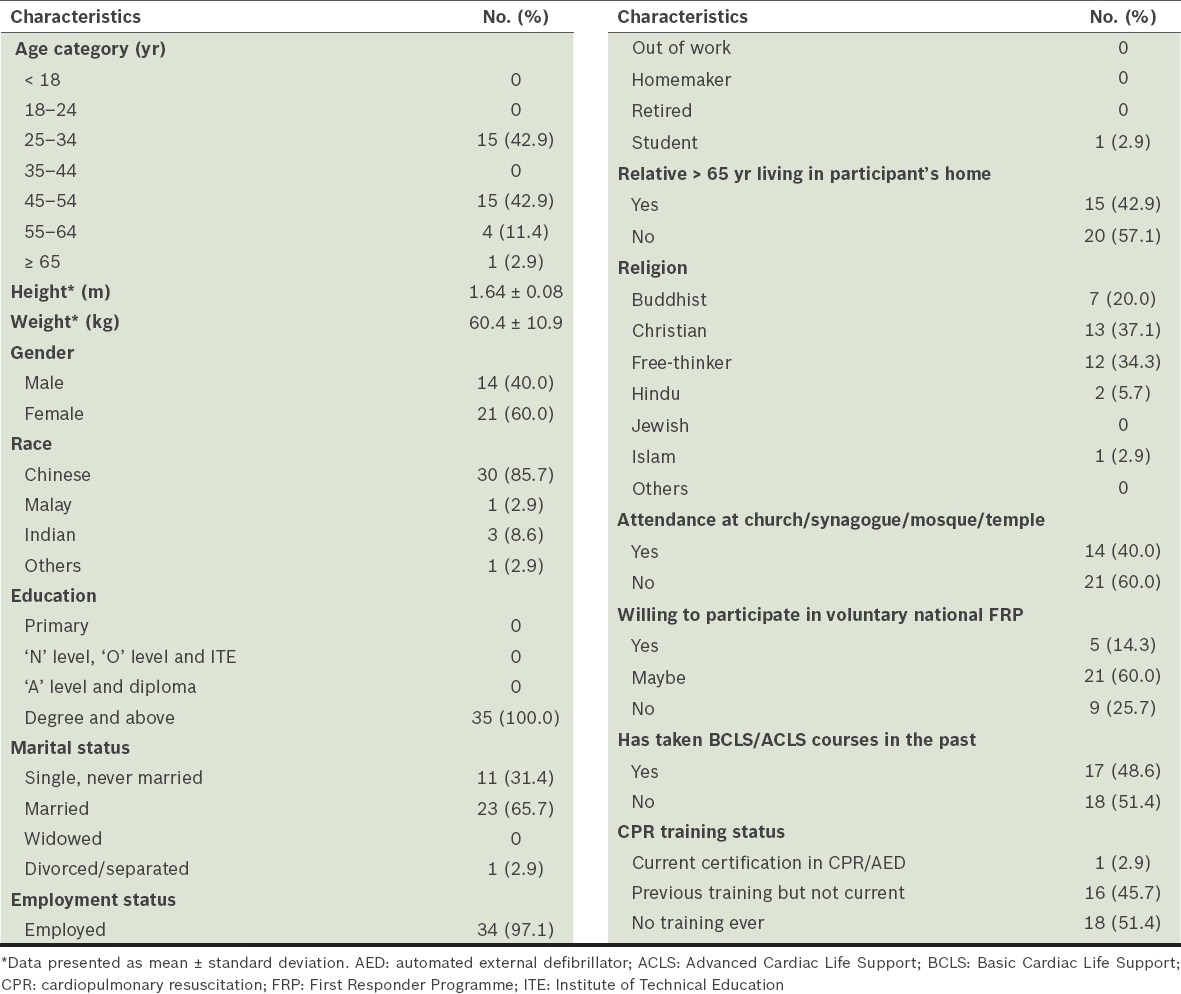
A total of 36 participants aged 25–70 years were enrolled in the study. One enrollee was unable to participate due to pre-existing injury and was excluded; 35 participants completed the training sessions, as well as the pre- and post-training surveys. Table I shows the demographic data of the participants. The majority of participants were 25–54 years old (85.7%), female (60.0%) and of Chinese ethnicity (85.7%). The average height and weight were 1.64 m and 60.4 kg, respectively. All the participants were university degree holders and 97.1% of them were employed as teachers. Almost half had been trained in basic life support skills in the past, which is not surprising since CPR is taught during compulsory national military service for all males. Only one person had a current certification. Due to incomplete data, only 25 participants with complete CPR compression data and survey data were included in the final analysis.
Table I
Participant demographics (n = 35).
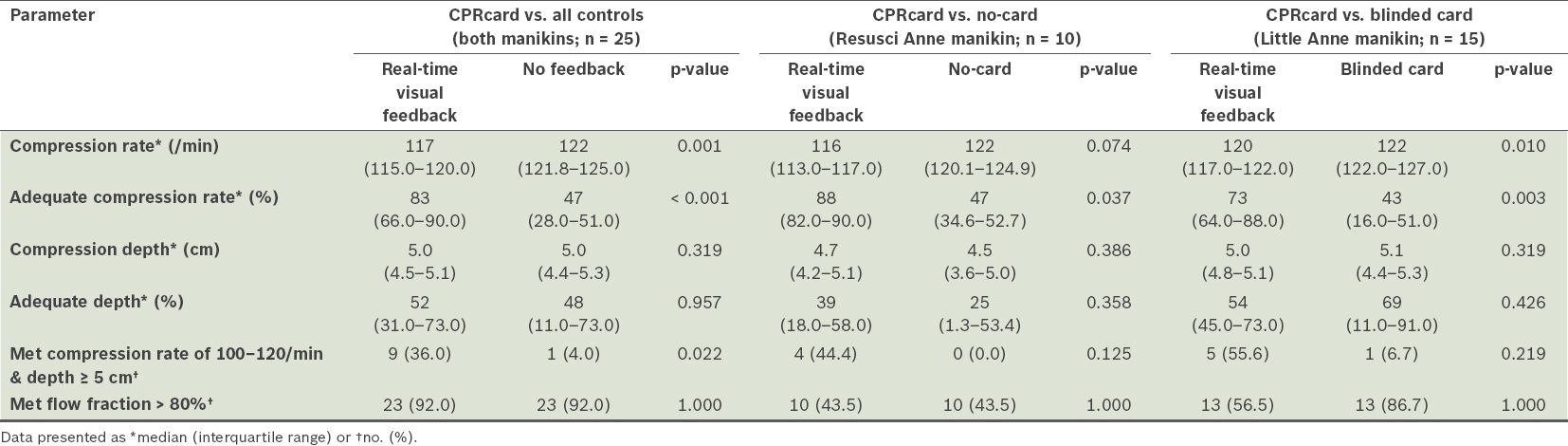
Table II presents the comparison of CPRcard compression parameters across the study arms. Participants in the CPRcard group achieved a better median compression rate compared to the group with no feedback (i.e. all controls), whose median compression rate fell slightly outside the optimal 100–120 compressions per minute range (CPRcard 117 vs. all controls 122, p = 0.001). The CPRcard group achieved a better median compression rate compared to the no-card group (CPRcard 116 vs. no-card 122, p = 0.074) and blinded-card group (CPRcard 120 vs. blinded-card 122, p = 0.010). It also had a higher rate of adequate compressions within the target rate range compared to all controls (CPRcard 83% vs. all controls 47%, p < 0.001), the no-card group (CPRcard 88% vs. no-card 47%, p = 0.037) and blinded-card group (CPRcard 73% vs. blinded-card 43%, p = 0.003). A comparison of median compression depth showed that the CPRcard group and all controls performed equally well across all arms (CPRcard 4.90 cm vs. all controls 4.99 cm, p = 0.319). The overall proportion of participants who achieved total compressions with adequate compression depth was similar in all the groups (CPRcard 52% vs. all controls 48%, p = 0.957); when the CPRcard group was compared solely to the no-card group, the difference was larger (CPRcard 39% vs. no-card 25%, p = 0.358). Although the blinded-card group had a higher rate of compression within the adequate depth range compared to the CPRcard group (CPRcard 54% vs blinded card 69%, p = 0.426), it also had a much wider interquartile range (11.0–91.0).
Table II
Comparison of CPRcard parameters.
In our composite measure of quality, participants in the CPRcard group delivered a higher percentage of quality CPR (i.e. met targets for both compression rate of 100–120 per minute and depth ≥ 5 cm) compared to the controls (CPRcard 36% vs. all controls 4%, p = 0.022), and this was statistically significant. The CPRcard group performed better than both the no-card (CPRcard 44.4% vs. no-card 0%, p = 0.125) and blinded-card (CPRcard 55.6% vs. blinded-card 6.7%, p = 0.219) groups. There was a shorter mean length of pause between the CPRcard and no-card groups (CPRcard 0 seconds vs. no-card 0.85 seconds, p = 0.028). Although flow fraction rate > 80% was the same overall (92.0%), a higher percentage of participants in the blinded-card group met the flow fraction target.
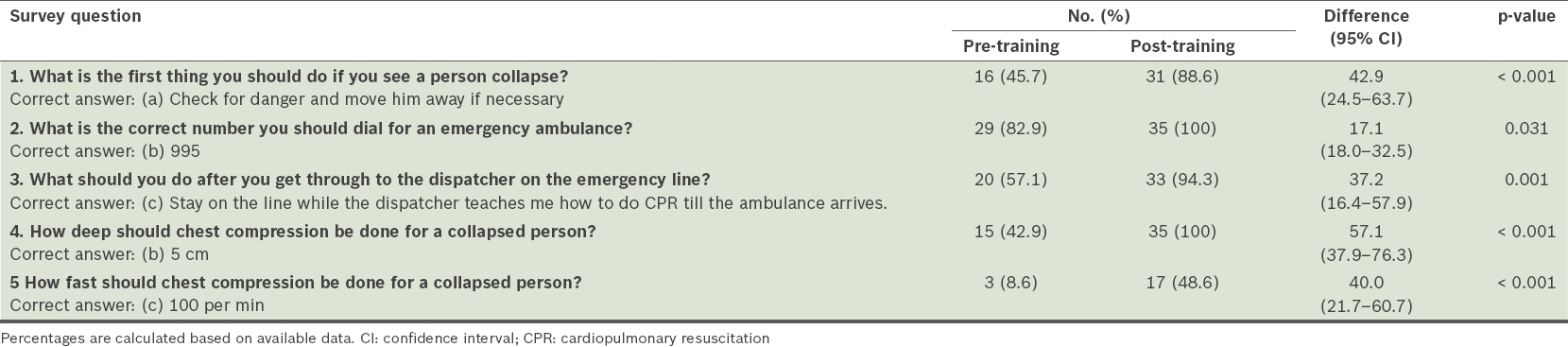
Table III presents the pre- and post-training survey results. When measuring the change in participants’ knowledge of CPR, we found a statistically significant improvement in the post-training survey results (p ≤ 0.001), with the greatest improvement seen in the correct answer for Question 4 (pre-training 43% vs. post-training 100%; 57% increase, p ≤ 0.001). The poorest result (i.e. furthest from 100% correct) was observed for Question 5, with only 50% of participants giving the correct answer in the post-training survey.
Table III
Comparison of correct answers between pre-training and post-training surveys regarding knowledge about CPR and automated external defibrillator (n = 35).
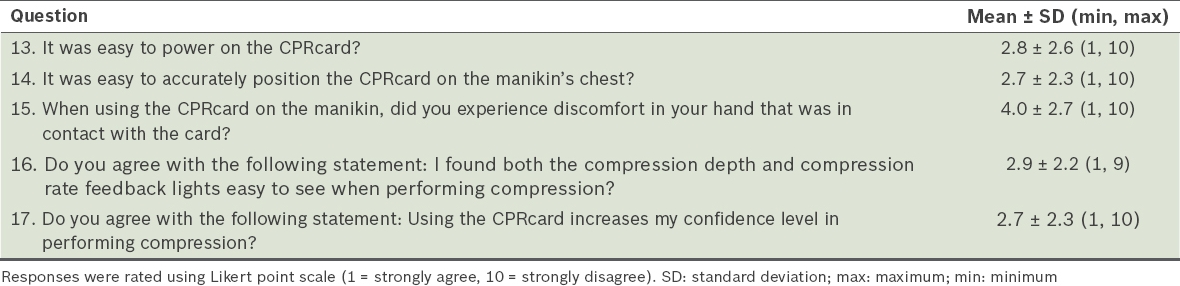
Table IV shows the results of the post-training survey section pertaining to users’ experience with the CPRcard. Participants strongly agreed with the statement, “Using the CPRcard increases my confidence level in performing compression”, with a mean score of 2.7 ± 2.3, where 1 = very confident and 10 = not confident. Questions regarding the ease of accurately positioning the CPRcard on the manikin’s chest and viewing the feedback lights during compressions also received good scores (mean 2.7 ± 2.3 and 2.9 ± 2.2, respectively, where 1 = very easy and 10 = not easy). The poorest score was received for Question 15, which asked participants if they experienced discomfort to their hand during compressions (mean 4.0 ± 2.7).
Table IV
Participants’ responses regarding usage of CPRcard (n = 35).
DISCUSSION
Overall, participants using the CPRcard performed better quality chest compressions compared to those who performed compressions without feedback. This is consistent with the results of other studies on feedback devices.(3,8,11) The positive effects of feedback from the CPRcard were observed in the higher number of compressions that came within the target range and the tighter grouping of performance data in and around the target rate and depth.
We were particularly intrigued by the potential of the CPRcard as a readily available tool to help lay bystanders respond to cardiac arrest with better quality chest compressions. As Kirkbright et al concluded, the body of research seems to indicate that the use of feedback devices during resuscitation can result in the rescuer performing compressions that are close to recommended standards.(11) Cheng et al’s results with nursing students using the CPRcard were consistent with ours.(6) However, to the best of our knowledge, the present study is the first to test the effect of using this ultraportable personal feedback device among a non-healthcare cohort in simulated adult resuscitation.
We observed several clear advantages of the CPRcard. First, the card can be carried around like a standard credit card in a wallet or pocketbook. Its convenience makes it more likely to be immediately available and thus deployable early during an out-of-hospital cardiac arrest (OHCA; 70% of which occur in residential areas). Second, as the card is a discrete device that is not linked to another device, its utility is not dependent on possession of a smartphone or an AED, as with other feedback devices in the market; this observation is aligned with that of Cheng et al.(6) Third, the device provides constant feedback while compressions are performed and not ‘correctively’, as observed with other devices.(28) We contend that any device that provides constant feedback bestows a reaffirming effect and does not leave the users wondering if their compressions are on target or whether the device is working properly. At least one study has found that constant feedback staves off the onset of fatigue for some time compared to having no feedback.(29) Finally, the card stores compression performance data. If used for training, the data can help to track quality trends, which the user and trainer can use for performance improvement. When used in an emergency, the card can provide compression data for retrospective analysis of the event. If these advantages translate to the card’s prevalence and use in an emergency, researchers will be able to collect data on bystander compressions during the early onset of cardiac arrest before professionals arrive on the scene. This has promising implications for studying the association between the quality of bystander CPR and clinical outcomes, which is currently a glaring gap in resuscitation research.
We expected to see compression quality improve with the use of feedback. Cheng et al tested the CPRcard for paediatric application among nurses.(6) Comparing the just-in-time arms, which is most comparable with our study, they found a 39% difference for adequate compression rate and a 10% difference for adequate depth, similar to our results of 36% and 4% difference for the adequate or in-target compression rate and depth, respectively. In the study by Wee and colleagues, which also involved nurses, the differences in in-target compression rate and depth between the groups with feedback and without feedback were 12.22% and 7.37%, respectively.(8) Similar patterns of improvement are also shown in other studies.(30,31)
There was one peculiarity in our results. The present study was embedded in a training initiative (i.e. DARE) that was designed to have trainers simulate the dispatcher’s role, including counting out the compressions for proper pace. This counting should have synchronised the rate of both groups to some extent, resulting in similar outcomes. Instead, we observed a large difference between the in-target compression rates of the two groups (feedback 83% vs. no feedback 47%). This gap could be explained by the fact that the participants who did not receive feedback could not benefit from its reassuring effect and, thus, we see the effect of fatigue as posited in Buléon et al’s study.(29)
Between the CPRcard group and all controls, we did not observe a statistically significant difference in compressions within the adequate depth target range. Again, this could be explained by the ‘push hard-push fast’ core instruction for compressions taught in training, or it could be that on average, our largely homogeneous, ethnically Chinese participant pool may be comparable in their strength and ability to compress the chest of this particular model of manikin regardless of feedback. An association between low body weight and declining compression quality has been established in the literature.(32) However, the effect of feedback can be seen again in the relatively narrower dispersion of depth data in and around the target range of the CPRcard group. Our review of the aforementioned literature on feedback devices suggests that improvement in compression depth is smaller than improvement in compression rate.
We observed another peculiarity in that the blinded-card group had a higher percentage of compressions in the in-target depth range compared to the unblinded-card (i.e. CPRcard) group. This could be because the unblinded group was challenged with trying to regulate compression depth to generate an in-target light on the meter, whereas the blinded group was free to simply push down hard on the chest. Although this finding was not statistically significant, the effect of the card was again observed in the far narrower depth-data dispersion (unblinded 45–73 vs. blinded 11–91; Table II).
We observed improvements in the rate of correct answers across all questions (Table III). However, we were dismayed at the high rate of incorrect responses to Question 5, which pertains to ‘how fast’ compressions should be performed. We surmised that although the appropriate compression rate was mentioned in the training video, this information could have been missed by the participants amidst the copious amount of information being shared in the short span of time. Past research suggests that a longer duration of training could, with caveat, improve retention of skill and knowledge.(33) Similar to the findings of our study, Gombeski et al’s study also showed that the scores for questions on compression rate and depth were relatively lower than those for other questions in their review quiz.(33)
In previous DARE CPRcard trainings, some participants pointed out that they experienced minor discomfort to the palm of the hand that was in contact with the card during compressions. However, as this was reported in only a few cases (the exact number was not known), no alarm was raised. Anecdotally, from our observations of the impressions on the palms, we opine that this could have occurred in some participants (both men and women) because their palm is softer, which makes it more susceptible to discomfort during compression. It is also possible that older participants may experience more of such discomfort due to a thinning of the skin with age. During compression, the edge of the card leaves an impression that usually goes away shortly after, with no long-term effects that we are aware of. In our opinion, this is not a matter of great concern compared to the issues faced when using bulkier devices, as shown in other studies.(34,35) However, mindful of the implications for prolonged use in an emergency situation, we highlighted this problem to the manufacturer and suggested that a rubber rim be added to the edge of the card, or that the card’s edge be rounded to minimise discomfort to the palm.
Swor et al identified the following predictors of bystander CPR: (a) the collapse occurred in a public place; (b) witnessed arrest; (c) bystander had CPR training; (d) bystander had a post-high school education; and (e) bystander was in the young-old age group.(36) Overwhelmingly, participants in our study agreed that the CPRcard gave them more confidence as responders in performing CPR (Table IV). We hope that its ease of use and the hands-only approach to CPR, as well as the increased confidence it gives users, will motivate trained bystanders to respond to OHCAs in greater numbers and in any setting, particularly in residential areas where there is the greatest room for improvement.
The present study had several limitations. First, DARE training was designed to simulate emergency system activation and laymen participation in dispatcher-assisted CPR over the phone. As trainers took on the role of dispatcher and counted at proper cadence (i.e. ‘1 and 2 and 3…’ etc.) during the compression duty-cycle, the counting could have resulted in an underestimation of the card’s effect on compression rate. This could explain the similarity in median compression rate in the feedback vs. no feedback groups’ performances. Second, the Resusci Anne SkillReporter was used to measure the compressions for the no-card group; however, the SkillReporter and CPRcard data are not necessarily harmonised because of differences in technology. Although a crossover effect cannot be ruled out, we hypothesised that by alternating the order of feedback vs. no-feedback performances between the ‘A’ and ‘B’ arms (Fig. 2), the risk of this effect was neutralised. Finally, because this is an experiment nested in an actual training intervention, we could not ethically interfere with the trainers who corrected compression postures and hand positions, as required from time to time. This might have had an effect on performance (e.g. a participant may have stopped to adjust his or her hand position), but we surmised that these corrections were minimal and distributed evenly across the trial arms, and thus did not skew the results.
In conclusion, the present study found that the use of the CPRcard feedback device during CPR training effectively improved the quality of CPR compressions performed by participants who were non-healthcare workers. Participants in our study found that the card was easy to use and that using it increased their confidence in performing compressions.
ACKNOWLEDGMENTS
The authors wish to thank the SingHealth Alice Lee Institute for Advanced Nursing for the loan of ten Resusci Anne manikins for this study and to Laerdal Medical (Norway) for their assistance throughout. This research is supported by the Ministry of Health, Singapore, and Singapore Totalisator Board under the ‘Bystander CPR and survival in six regions of Singapore saturated with trained and equipped volunteers with AED access’ study. The authors report no conflicts of interest.
References Kramer-Johansen J, Myklebust H, Wik L, et al. Quality of out-of-hospital cardiopulmonary resuscitation with real time automated feedback:a prospective interventional study.Resuscitation. 2006;71:283-92. Noordergraaf GJ, Drinkwaard BW, van Berkom PF, et al. The quality of chest compressions by trained personnel:the effect of feedback, via the CPREzy, in a randomized controlled trial using a manikin model.Resuscitation. 2006;69:241-52. Yeung J, Meeks R, Edelson D, et al. The use of CPR feedback/prompt devices dang training and CPR performance:a systematic review.Resuscitation. 2009;80:743-51. Skorning M, Beckers SK, Brokmann JCh, et al. New visual feedback device improves performance of chest compressions by professionals in simulated cardiac arrest.Resuscitation. 2010;81:53-8. Wutzler A, Bannehr M, von Ulmenstein S, et al. Performance of chest compressions with the use of a new audio-visual feedback device:a randomized manikin study in health care professionals.Resuscitation. 2015;87:81-5. Cheng A, Brown LL, Duff JP, et al. International Network for Simulation-Based Pediatric Innovation, Research & Education (INSPIRE). CPR InvestigatorsImproving cardiopulmonary resuscitation with a CPR feedback device and refresher simulations (CPR CARES Study):a randomized clinical trial.JAMA Pediatr. 2015;169:137-44. Bobrow BJ, Vadeboncoeur TF, Stolz U, et al. The influence of scenario-based training and real-time audiovisual feedback on out-of-hospital cardiopulmonary resuscitation quality and survival from out-of-hospital cardiac arrest.Ann Emerg Med. 2013;62:47-56.e1. Wee JC, Nandakumar M, Chan YH, et al. Effect of using an audiovisual CPR feedback device on chest compression rate and depth.Ann Acad Med Singapore. 2014;43:33-8. Zapletal B, Greif R, Stumpf D, et al. Comparing three CPR feedback devices and standard BLS in a single rescuer scenario:a randomised simulation study.Resuscitation. 2014;85:560-6. Lyngeraa TS, Hjortrup PB, Wulff NB, Aagaard T, Lippert A.Effect of feedback on delaying deterioration in quality of compressions dang 2 minutes of continuous chest compressions:a randomized manikin study investigating performance with and without feedback.Scand J Trauma Resusc Emerg Med. 2012;20:16. Kirkbright S, Finn J, Tohira H, et al. Audiovisual feedback device use by health care professionals dang CPR:a systematic review and meta-analysis of randomised and non-randomised trials.Resuscitation. 2014;24:460-71. Singapore Civil Defence ForceEmergency Medical Services Statistics January-December 2015 [online]. Available at: https://www.scdf.gov.sg/sites/www.scdf.gov.sg/files/Emergency%20Medical%20Services%20Statistics%20Jan-Dec%202015.pdf. Accessed May 27 2017. Abella BS, Sandbo N, Vassilatos P, et al. Chest compression rates dang cardiopulmonary resuscitation are suboptimal:a prospective study dang in-hospital cardiac arrest.Circulation. 2005;111:428-34. Idris AH, Guffey D, Aufderheide TP, et al. Resuscitation Outcomes Consortium (ROC) InvestigatorsRelationship between chest compression rates and outcomes from cardiac arrest.Circulation. 2012;125:3004-12. Stiell I, Brown SP, Christenson J, et al. Resuscitation Outcomes Consortium (ROC) InvestigatorsWhat is the role of chest compression depth dang out-of-hospital cardiac arrest?.Crit CareMed. 2012;40:1192-98. Stiell IG, Brown SP, Nichol G, et al. Resuscitation Outcomes Consortium InvestigatorsWhat is the optimal chest compression depth dang out-of-hospital cardiac arrest resuscitation of adult patients?.Circulation. 2014;130:1962-70. Bobrow BJ, Clark LL, Ewy GA, et al. Minimally interrupted cardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest.JAMA. 2008;299:1158-65. Bobrow BJ, Spaite DW, Berg RA, et al. Chest compression-only CPR by lay rescuers and survival from out-of-hospital cardiac arrest.JAMA. 2010;304:1447-54. Hallstrom AP.Dispatcher-assisted “phone” cardiopulmonary resuscitation by chest compression alone or with mouth-to-mouth ventilation.Crit Care Med. 2000;28:11 SupplN190-2. Svensson L, Bohm K, Castrèn M, et al. Compression-only CPR or standard CPR in out-of-hospital cardiac arrest.N Engl J Med. 2010;363:434-42. Min Ko RJ, Wu VX, Lim SH, San Tam WW, Liaw SY.Compression-only cardiopulmonary resuscitation in improving bystanders’cardiopulmonary resuscitation performance:a literature review.Emerg Med J. 2016;33:882-8. Yao L, Wang P, Zhou L, et al. Compression-only cardiopulmonary resuscitation vs standard cardiopulmonary resuscitation:an updated meta-analysis of observational studies.Am J Emerg Med. 2014;32:517-23. Cho GC, Sohn YD, Kang KH, et al. The effect of basic life support education on laypersons’willingness in performing bystander hands only cardiopulmonary resuscitation.Resuscitation. 2010;81:691-4. Vaillancourt C, Grimshaw J, Brehaut JC, et al. A survey of attitudes and factors associated with successful cardiopulmonary resuscitation (CPR) knowledge transfer in an older population most likely to witness cardiac arrest:design and methodology.BMC Emerg Med. 2008;8:13. Neumar RW, Shuster M, Callaway CW, et al. Part 1:Executive Summary:2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.Circulation. 2015;132:18 Suppl 2315-67. Travers AH, Perkins GD, Berg RA, et al. Basic Life Support Chapter CollaboratorsPart 3:Adult basic life support and automated external defibrillation:2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations.Circulation. 2015;132:16 Suppl 151-83. Perkins GD, Handley AJ, Koster RW, et al. Adult basic life support and automated external defibrillation section CollaboratorsEuropean Resuscitation Council Guidelines for Resuscitation 2015:Section 2. Adult basic life support and automated external defibrillation.Resuscitation. 2015;95:81-99. Hostler D, Everson-Stewart S, Rea TD, et al. Resuscitation Outcomes Consortium InvestigatorsEffect of real-time feedback dang cardiopulmonary resuscitation outside hospital:prospective, cluster-randomised trial.BMJ. 2011;342:d512. Buléon C, Delaunay J, Parienti JJ, et al. Impact of a feedback device on chest compression quality dang extended manikin cardiopulmonary resuscitation:a randomized crossover study.Am J Emerg Med. 2016;34:1754-60. Truszewski Z, Szarpak L, Kurowski A, et al. Randomized trial of the chest compressions effectiveness comparing 3 feedback CPR devices and standard basic life support by nurses.Am J Emerg Med. 2016;34:381-5. Skorning M, Derwall M, Brokmann JC, et al. External chest compressions using a mechanical feedback device:cross-over simulation study.Anaesthesist. 2011;60:717-22. Hasegawa T, Daikoku R, Saito S, Saito Y.Relationship between weight of rescuer and quality of chest compression dang cardiopulmonary resuscitation.J Physiol Anthropol. 2014;33:16. Gombeski WR, JrEffron DM, Ramirez AG, Moore TJ.Impact on retention:comparison of two CPR training programs.Am J Public Health. 1982;72:849-52. Hong JY, Oh JH, Kim CW, Lee DH.Hand injaes caused by feedback device usage dang cardiopulmonary resuscitation training.Resuscitation. 2016;107:3-4. Perkins GD, Augré C, Rogers H, Allan M, Thickett DR.CPREzy:an evaluation dang simulated cardiac arrest on a hospital bed.Resuscitation. 2005;Jan64:103-8. Swor R, Khan I, Domeier R, Honeycutt L, Chu K, Compton S.CPR training and CPR performance:do CPR-trained bystanders perform CPR?.Acad Emerg Med. 2006;13:596-601.
REFERENCES
1. Kramer-Johansen J, Myklebust H, Wik L, et al. Quality of out-of-hospital cardiopulmonary resuscitation with real time automated feedback: a prospective interventional study. Resuscitation 2006; 71:283-92. https://doi.org/10.1016/j.resuscitation.2006.05.011
PMid:17070980
2. Noordergraaf GJ, Drinkwaard BW, van Berkom PF, et al. The quality of chest compressions by trained personnel: the effect of feedback, via the CPREzy, in a randomized controlled trial using a manikin model. Resuscitation 2006; 69:241-52. https://doi.org/10.1016/j.resuscitation.2005.08.008
PMid:16457935
3. Yeung J, Meeks R, Edelson D, et al. The use of CPR feedback/prompt devices during training and CPR performance: a systematic review. Resuscitation 2009; 80:743-51. https://doi.org/10.1016/j.resuscitation.2009.04.012
PMid:19477574
4. Skorning M, Beckers SK, Brokmann JCh, et al. New visual feedback device improves performance of chest compressions by professionals in simulated cardiac arrest. Resuscitation 2010; 81:53-8. https://doi.org/10.1016/j.resuscitation.2009.10.005
PMid:19913346
5. Wutzler A, Bannehr M, von Ulmenstein S, et al. Performance of chest compressions with the use of a new audio-visual feedback device: a randomized manikin study in health care professionals. Resuscitation 2015; 87:81-5. https://doi.org/10.1016/j.resuscitation.2014.10.004
PMid:25449342
6. Cheng A, Brown LL, Duff JP, et al; International Network for Simulation-Based Pediatric Innovation, Research, & Education (INSPIRE) CPR Investigators. Improving cardiopulmonary resuscitation with a CPR feedback device and refresher simulations (CPR CARES Study): a randomized clinical trial. JAMA Pediatr 2015; 169:137-44. https://doi.org/10.1001/jamapediatrics.2014.2616
PMid:25531167
7. Bobrow BJ, Vadeboncoeur TF, Stolz U, et al. The influence of scenario-based training and real-time audiovisual feedback on out-of-hospital cardiopulmonary resuscitation quality and survival from out-of-hospital cardiac arrest. Ann Emerg Med 2013; 62:47-56 e1.
8. Wee JC, Nandakumar M, Chan YH, et al. Effect of using an audiovisual CPR feedback device on chest compression rate and depth. Ann Acad Med Singapore 2014; 43:33-8.
PMid:24557463
9. Zapletal B, Greif R, Stumpf D, et al. Comparing three CPR feedback devices and standard BLS in a single rescuer scenario: a randomised simulation study. Resuscitation 2014; 85:560-6. https://doi.org/10.1016/j.resuscitation.2013.10.028
PMid:24215730
10. Lyngeraa TS, Hjortrup PB, Wulff NB, Aagaard T, Lippert A. Effect of feedback on delaying deterioration in quality of compressions during 2 minutes of continuous chest compressions: a randomized manikin study investigating performance with and without feedback. Scand J Trauma Resusc Emerg Med 2012; 20:16. https://doi.org/10.1186/1757-7241-20-16
PMid:22373499 PMCid:PMC3310737
11. Kirkbright S, Finn J, Tohira H, et al. Audiovisual feedback device use by health care professionals during CPR: a systematic review and meta-analysis of randomised and non-randomised trials. Resuscitation 2014; 24:460-71. https://doi.org/10.1016/j.resuscitation.2013.12.012
PMid:24361457
13. Abella BS, Sandbo N, Vassilatos P, et al. Chest compression rates during cardiopulmonary resuscitation are suboptimal: a prospective study during in-hospital cardiac arrest. Circulation 2005; 111:428-34. https://doi.org/10.1161/01.CIR.0000153811.84257.59
PMid:15687130
14. Idris AH, Guffey D, Aufderheide TP, et al; Resuscitation Outcomes Consortium (ROC) Investigators. Relationship between chest compression rates and outcomes from cardiac arrest. Circulation 2012; 125:3004-12. https://doi.org/10.1161/CIRCULATIONAHA.111.059535
PMid:22623717 PMCid:PMC3388797
15. Stiell I, Brown SP, Christenson J, et al; Resuscitation Outcomes Consortium (ROC) Investigators. What is the role of chest compression depth during out-of-hospital cardiac arrest?. Crit CareMed 2012; 40:1192-98. https://doi.org/10.1097/CCM.0b013e31823bc8bb
PMid:22202708 PMCid:PMC3307954
16. Stiell IG, Brown SP, Nichol G, et al; Resuscitation Outcomes Consortium Investigators. What is the optimal chest compression depth during out-of-hospital cardiac arrest resuscitation of adult patients? Circulation 2014; 130:1962-70. https://doi.org/10.1161/CIRCULATIONAHA.114.008671
PMid:25252721
17. Bobrow BJ, Clark LL, Ewy GA, et al. Minimally interrupted cardiac resuscitation by emergency medical services for out-of-hospital cardiac arrest. JAMA 2008; 299:1158-65. https://doi.org/10.1001/jama.299.10.1158
PMid:18334691
18. Bobrow BJ, Spaite DW, Berg RA, et al. Chest compression-only CPR by lay rescuers and survival from out-of-hospital cardiac arrest. JAMA 2010; 304:1447-54. https://doi.org/10.1001/jama.2010.1392
PMid:20924010
19. Hallstrom AP. Dispatcher-assisted "phone" cardiopulmonary resuscitation by chest compression alone or with mouth-to-mouth ventilation. Crit Care Med 2000; 28(11 Suppl):N190-2. https://doi.org/10.1097/00003246-200011001-00004
PMid:11098943
20. Svensson L, Bohm K, Castrèn M, et al. Compression-only CPR or standard CPR in out-of-hospital cardiac arrest. N Engl J Med 2010; 363:434-42. https://doi.org/10.1056/NEJMoa0908991
PMid:20818864
21. Min Ko RJ, Wu VX, Lim SH, San Tam WW, Liaw SY. Compression-only cardiopulmonary resuscitation in improving bystanders' cardiopulmonary resuscitation performance: a literature review. Emerg Med J 2016; 33:882-8. https://doi.org/10.1136/emermed-2015-204771
PMid:26830148
22. Yao L, Wang P, Zhou L, et al. Compression-only cardiopulmonary resuscitation vs standard cardiopulmonary resuscitation: an updated meta-analysis of observational studies. Am J Emerg Med 2014; 32:517-23. https://doi.org/10.1016/j.ajem.2014.01.055
PMid:24661781
23. Cho GC, Sohn YD, Kang KH, et al. The effect of basic life support education on laypersons' willingness in performing bystander hands only cardiopulmonary resuscitation. Resuscitation 2010; 81:691-4. https://doi.org/10.1016/j.resuscitation.2010.02.021
PMid:20347208
24. Vaillancourt C, Grimshaw J, Brehaut JC, et al. A survey of attitudes and factors associated with successful cardiopulmonary resuscitation (CPR) knowledge transfer in an older population most likely to witness cardiac arrest: design and methodology. BMC Emerg Med 2008; 8:13. https://doi.org/10.1186/1471-227X-8-13
PMid:18986547 PMCid:PMC2585573
25. Neumar RW, Shuster M, Callaway CW, et al. Part 1: Executive Summary: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015; 132(18 Suppl 2):S315-67. https://doi.org/10.1161/CIR.0000000000000252
PMid:26472989
26. Travers AH, Perkins GD, Berg RA, et al; Basic Life Support Chapter Collaborators. Part 3: Adult basic life support and automated external defibrillation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2015; 132(16 suppl 1):S51-83. https://doi.org/10.1161/CIR.0000000000000272
PMid:26472859
27. Perkins GD, Handley AJ, Koster RW, et al; Adult basic life support and automated external defibrillation section Collaborators. European Resuscitation Council Guidelines for Resuscitation 2015: Section 2. Adult basic life support and automated external defibrillation. Resuscitation 2015; 95:81-99. https://doi.org/10.1016/j.resuscitation.2015.07.015
PMid:26477420
28. Hostler D, Everson-Stewart S, Rea TD, et al; Resuscitation Outcomes Consortium Investigators. Effect of real-time feedback during cardiopulmonary resuscitation outside hospital: prospective, cluster-randomised trial. BMJ 2011; 342:d512. https://doi.org/10.1136/bmj.d512
PMid:21296838 PMCid:PMC3033623
29. Buléon C, Delaunay J, Parienti JJ, et al. Impact of a feedback device on chest compression quality during extended manikin cardiopulmonary resuscitation: a randomized crossover study. Am J Emerg Med 2016; 34:1754-60. 30. Truszewski Z, Szarpak L, Kurowski A, et al. Randomized trial of the chest compressions effectiveness comparing 3 feedback CPR devices and standard basic life support by nurses. Am J Emerg Med 2016; 34:381-5. https://doi.org/10.1016/j.ajem.2015.11.003
PMid:26612703
31. Skorning M, Derwall M, Brokmann JC, et al. External chest compressions using a mechanical feedback device: cross-over simulation study. Anaesthesist 2011; 60:717-22. https://doi.org/10.1007/s00101-011-1871-6
PMid:21437754
32. Hasegawa T, Daikoku R, Saito S, Saito Y. Relationship between weight of rescuer and quality of chest compression during cardiopulmonary resuscitation. J Physiol Anthropol 2014; 33:16. https://doi.org/10.1186/1880-6805-33-16
PMid:24957919 PMCid:PMC4079182
33. Gombeski WR Jr, Effron DM, Ramirez AG, Moore TJ. Impact on retention:comparison of two CPR training programs. Am J Public Health 1982; 72:849-52. https://doi.org/10.2105/AJPH.72.8.849
34. Hong JY, Oh JH, Kim CW, Lee DH. Hand injuries caused by feedback device usage during cardiopulmonary resuscitation training. Resuscitation 2016; 107:e3-4. https://doi.org/10.1016/j.resuscitation.2016.08.001
PMid:27521475
35. Perkins GD, Augré C, Rogers H, Allan M, Thickett DR. CPREzy: an evaluation during simulated cardiac arrest on a hospital bed. Resuscitation 2005 Jan; 64:103-8. https://doi.org/10.1016/j.resuscitation.2004.08.011
PMid:15629562
36. Swor R, Khan I, Domeier R, Honeycutt L, Chu K, Compton S. CPR training and CPR performance: do CPR-trained bystanders perform CPR? Acad Emerg Med 2006; 13:596-601. https://doi.org/10.1111/j.1553-2712.2006.tb01017.x
PMid:16614455