

Abstract
INTRODUCTION
Singapore has a rapidly ageing population and an increasing prevalence of Alzheimer’s disease (AD). Compliance to AD medications is associated with treatment effectiveness. We investigated compliance to acetylcholinesterase inhibitors (AChEIs) and N-methyl-D-aspartate (NMDA) receptor antagonist and treatment persistence among patients seen at the General Memory Clinic of National University Hospital, Singapore. We also identified the reasons for non-compliance.
METHODS
Patients seen at the General Memory Clinic between 1 January 2013 and 31 December 2014, who were prescribed AChEIs and NMDA receptor antagonist, were included in this retrospective cohort study. Non-compliance to medications was indirectly measured by failure to renew prescription within 60 days of the last day of medication supplied by the previous prescription. The reasons for non-compliance were identified.
RESULTS
A total of 144 patients were included. At one year, 107 patients were compliant to AD medications, while 37 patients were non-compliant. Around 60% of the non-compliant patients discontinued the use of AD medications within the first six months, and the mean persistent treatment period among this group of patients was 10.3 ± 3.5 months. The main reason for non-compliance was patients’ and caregivers’ perception that memory loss was of lower priority than other coexisting illnesses. Other reasons for non-compliance included side effects of medications (18.9%), perceived ineffectiveness of treatment (16.2%), inability to attend clinic (5.4%) and high cost of medications (2.7%).
CONCLUSION
Our findings suggest that the reasons for medication non-compliance can be identified early. Better compliance may be achieved through a multidisciplinary approach to patient education.
INTRODUCTION
In 2015, it was estimated that around 50 million individuals suffered from dementia globally,(1) with Alzheimer’s disease (AD) being the most common cause of dementia.(2) This number is projected to increase to 135 million by 2050.(2) Singapore has one of the fastest ageing populations in the Asia Pacific region and the prevalence of dementia is expected to increase substantially.(3) Dementia is a major healthcare challenge, as it is a leading cause of disability and high healthcare cost.(3) The main class of drug approved for the management of mild to severe dementia due to AD is the acetylcholinesterase inhibitors (AChEIs),(4) which antagonise the action of acetylcholinesterase(5) and target the cholinergic deficit in AD,(6) hence improving mood, cognition and behaviour. Memantine, an N-methyl-D-aspartate (NMDA) receptor antagonist, is recommended for use in AD patients with moderate to severe dementia.
Compliance to the use of AD medications is crucial to achieving maximal treatment efficacy.(7) However, medication compliance in AD patients is a problem due to their diminished cognition.(8) Furthermore, the side effects and high cost of AD medications makes compliance even more challenging. In an Austrian study, more than 50% of patients with dementia discontinued the use of AChEIs within 12 months of therapy initiation.(9) Similarly, a Canadian study reported a non-compliance rate of 46% for galantamine, 54% for donepezil and 60% for rivastigmine after one year of initiation of AChEIs.(4) Borah et al found that more than 40% of AD patients were non-compliant to medications, and attributed it to overall pill burden (odds ratio [OR] 1.192, p < 0.001).(10) A recent review identified several determinants of non-compliance to AD medications, including patients’ belief that AD is age-related, medication side effects and caregivers’ unrealistic expectations of treatment benefits.(11) Medication non-compliance has critical negative implications on achieving optimal treatment outcome and indirectly imposes significant economic cost to the healthcare system.(12) In addition, medication non-compliance among AD patients was found to be associated with a higher risk of hospital admission.(13)
As no local data on medication compliance in AD is available, this study aimed to identify the reasons for non-compliance to medications and estimate the time-point of treatment discontinuation among AD patients in Singapore. We opine that treatment continuation and medication compliance are influenced by a country’s unique cultural and social factors. Hence, this study may provide a foundation to improve the overall management of AD in Singapore.
METHODS
Participants of this study were drawn from patients whose first visit to the General Memory Clinic, National University Hospital, Singapore, was between 1 January 2013 and 31 December 2014. All patients were diagnosed using clinical and neuropsychological assessment results at a weekly consensus meeting attended by clinicians and neuropsychologists. This study included patients who had been diagnosed with AD and prescribed with AChEIs and/or NMDA receptor antagonist. Information on the study population, such as demographics, education level, clinical history and medications, was extracted from hospital records. Compliance to AD medications was tracked for at least one year. Telephone calls were made to the caregiver of patients who defaulted on appointment without specific reasons to understand their reasons for non-compliance to medication. The duration of treatment persistence was also recorded for this group of patients to determine the proportion of patients who persisted with treatment for < 6 months, 6–12 months and > 12 months after their first visit to the General Memory Clinic.
The definition of medication compliance in this study aligns to that of the World Health Organization (WHO), which is the degree of conformity to the recommendations on medications prescribed with respect to the timing, frequency and dosage by a healthcare provider.(14) Non-compliance to medication in this study was indirectly measured by the failure to renew prescription within 60 days of the last day of medication supplied by the previous prescription. The duration of 60 days was selected, as it is the average follow-up duration between visits for each patient. Several studies have also used failure to renew a prescription during a 60-day follow-up period as an indicator of non-compliance.(15-17) Patients discharged from regular follow-up with the General Memory Clinic to another clinical provider or discharged to outpatient community care were considered to be compliant to medication use. Treatment persistence in the study was defined as the duration for which a patient complied with the treatment without defaulting at least one scheduled follow-up appointment with the General Memory Clinic.
Factors for non-compliance to AD medications were reported in accordance with the five dimensions classified by the WHO:(14) (1) social and economic factors such as illiteracy, unstable living conditions and high cost of medications; (2) healthcare team- and system-related factors such as healthcare provider-patient relationship and healthcare costs; (3) condition-related factors such as severity of symptoms and comorbidities; (4) therapy-related factors such as complexity of medical regimen, duration of treatment and previous treatment failures; and (5) patient-related factors such as age, gender, resources, knowledge, perception, attitudes and beliefs.
Data analysis was performed using the IBM SPSS Statistics version 22.0 (IBM Corp, Armonk, NY, USA). All statistical tests were two-tailed with a significance level (a) of 0.05. Univariate analysis was performed (chi-square test for categorical and independent samples; t-test for continuous variables) to explore associations of demographic characteristics and compliance to medication use among AD patients. The following variables were analysed: age; gender; ethnicity; Mini Mental State Examination (MMSE) scores; and Montreal Cognitive Assessment (MoCA) scores. Approval to conduct this study was obtained from the National Healthcare Group Ethics Review Board (Domain-Specific Review Board).
RESULTS
A total of 426 patients had their first visit to the General Memory Clinic between 1 January 2013 and 31 December 2014. These patients were screened for eligibility and a total of 144 patients were included in the study (
Fig. 1
Flow chart for the inclusion of patients in the study. AChEIs: acetylcholinesterase inhibitors; AD: Alzheimer’s disease; CADASIL: cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; CIND: cognitive impaired, no dementia; DLB: dementia with Lewy bodies; DNOS: dementia with no specified cause; FTD: fronto-temporal dementia; MCI: mild cognitive impairment; NMDA: N-methyl-D-aspartate; PDD: Parkinson’s disease with dementia; VAD: vascular dementia; VCIND: vascular cognitive impairment, no dementia
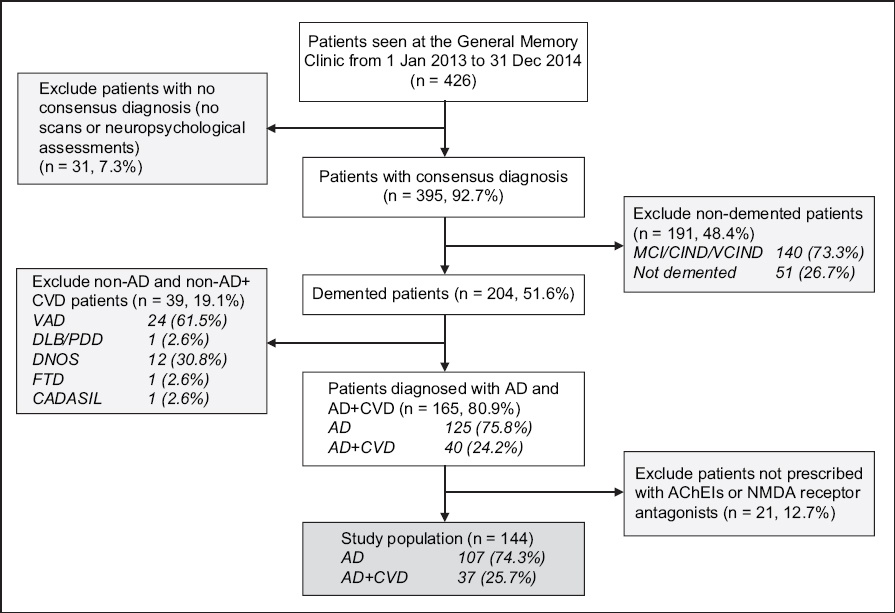
Table I
Characteristics of patients included in the study (n = 144).
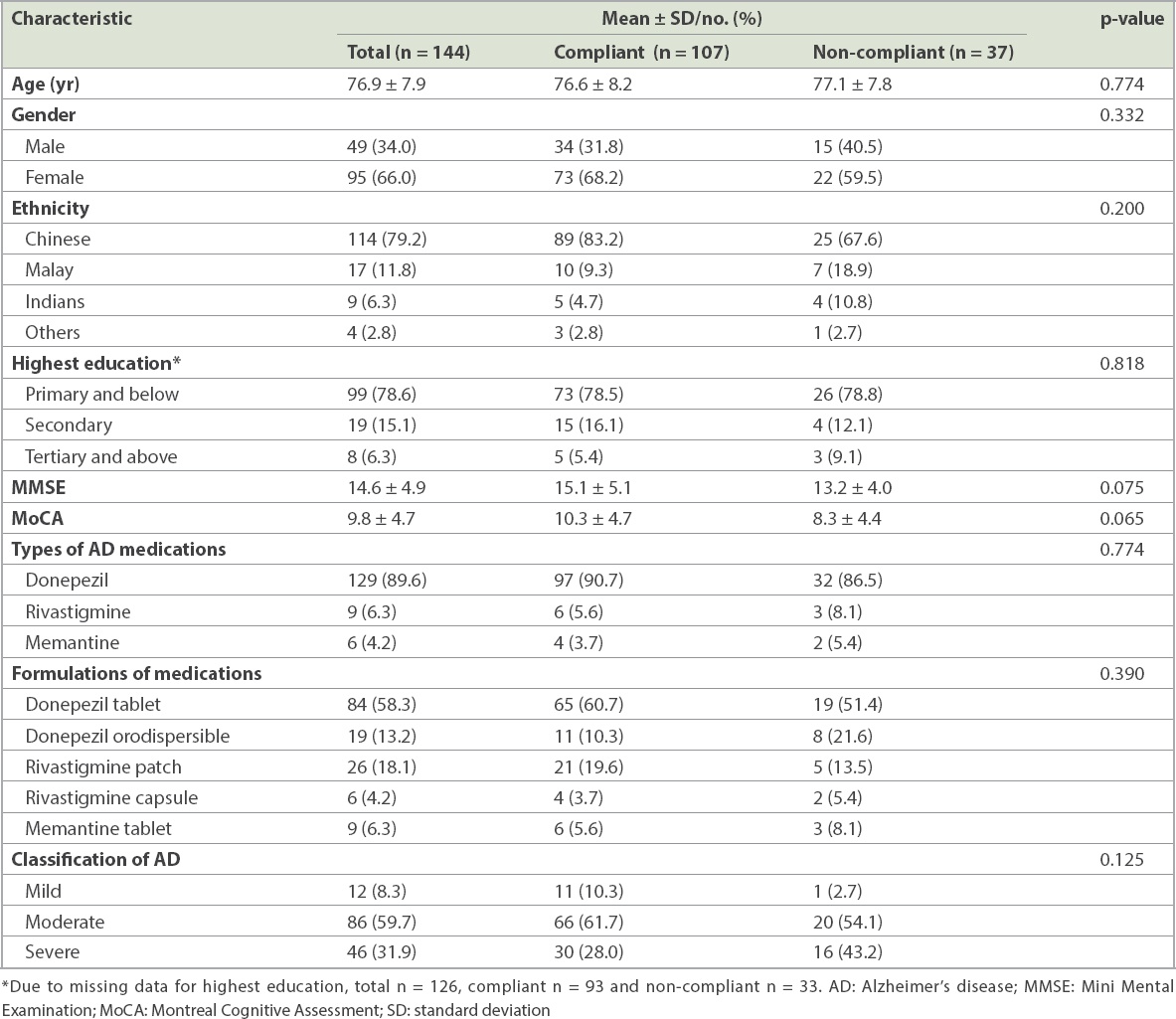
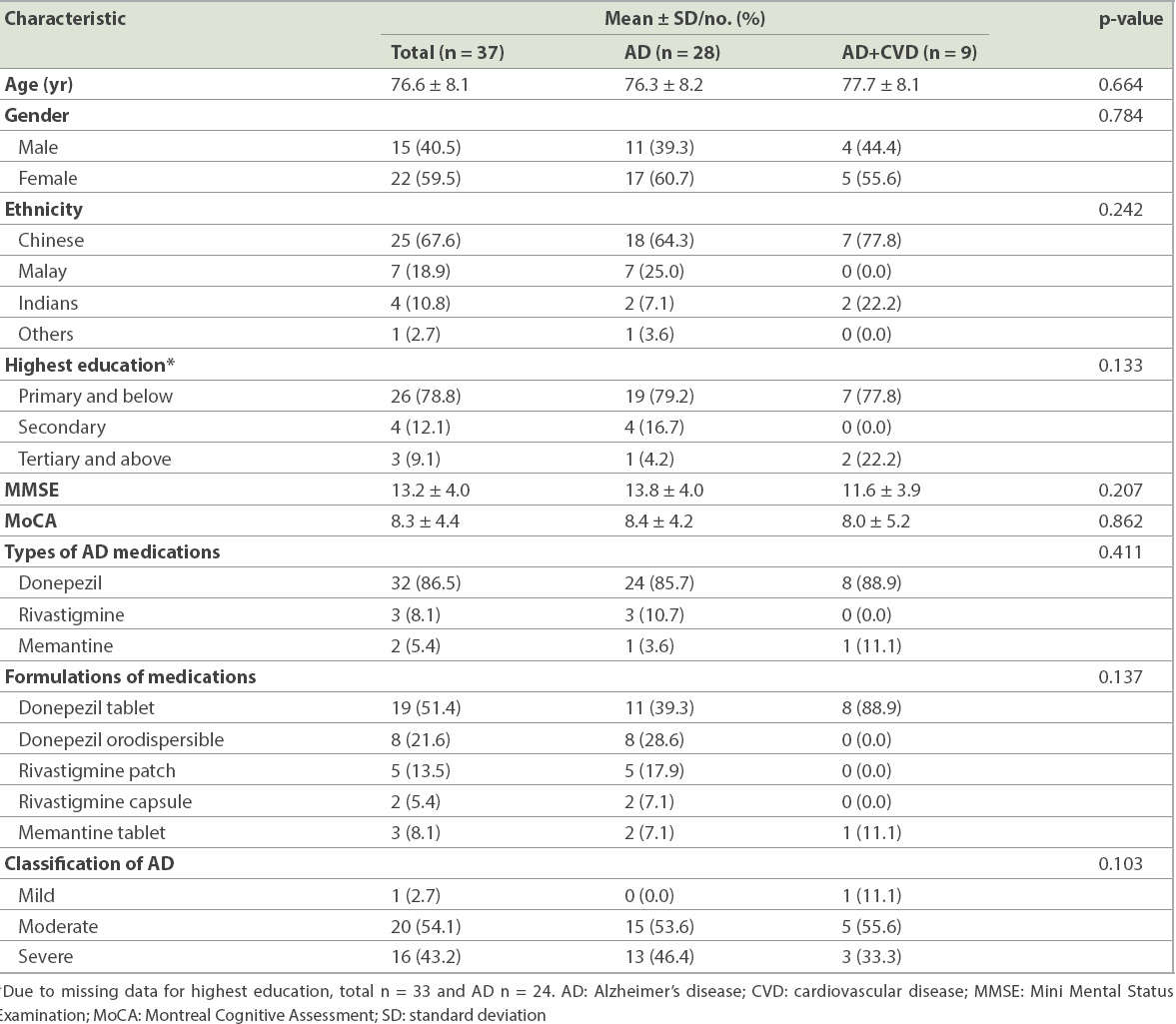
Table II
Characteristics of non-compliant patients included in this study (n = 37).
Factors influencing medication non-compliance included patient-related, therapy-related, condition-related and socioeconomic factors (
Table III
Reasons for non-compliance to medication use (n = 37).
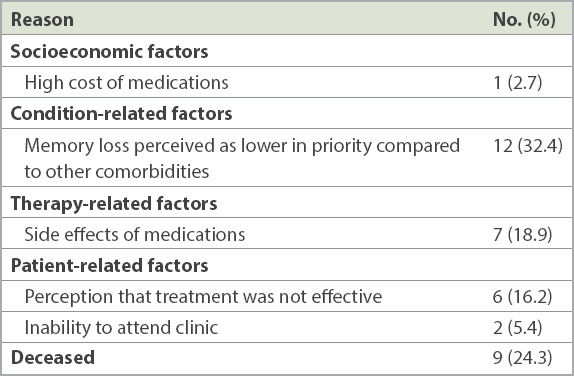
For therapy-related factors, 7 (18.9%) patients were non-compliant due to side effects from the AD medications: six patients reported side effects from donepezil and one patient from rivastigmine patch. Side effects of donepezil were generally gastrointestinal-related, including nausea, diarrhoea and bloatedness, while the side effect of rivastigmine patch was headache.
In terms of condition-related factors, 12 (32.4%) of the non-compliant patients and their caregivers viewed a decline in memory as a natural phenomenon of ageing, and hence perceived memory loss as being less important than other comorbidities. Among these patients, many were diagnosed with concomitant cardiovascular diseases, such as hypertension, heart failure and atrial fibrillation, which were managed with several medications. As these cardiovascular comorbidities were considered more critical than the memory loss experienced in AD, these patients and their caregivers inevitably neglected AD treatment and compliance to AD medications. Among this group of patients, two were undergoing chemotherapy, which compounded their social and emotional burden. The main socioeconomic factor that contributed to non-compliance was high medication costs (n = 1, 2.7%). While other studies have found illiteracy and low level of education to be significantly associated with poor medication compliance,(19) our study did not find such associations.
The mean duration of persistent treatment was 10.3 ± 3.5 months. Out of the 144 patients, 114 (79.2%) persisted in their treatment for > 12 months from their first visit to the General Memory Clinic, 9 (6.3%) persisted for 6–12 months, and 21 (14.6%) persisted for < 6 months. All the compliant patients persisted in treatment for > 12 months, whereas 60% of the non-compliant patients persisted for < 6 months.
DISCUSSION
The majority of patients were compliant to the use of AD medications, as measured by the renewal of their previous prescription within 60 days; about 25% of the patients were non-compliant to medication use. This finding is consistent with a recent study conducted in Taiwan, where the non-compliance rate of AChEIs use was 24%.(20) Similarly, AChEI non-compliance rates ranging from 25% to 50% have been reported in other observational studies.(4,9,21) A systematic review also found that compliance to AD medications ranged from 17% to 42% across seven studies.(18) This illustrates the need for compliance assessment in the individual society, as each is determined by its unique sociocultural background.
A mixture of patient-related, therapy-related, condition-related and socioeconomic factors were found to influence the compliance level of our included patients. In terms of patient-related factors, age (p = 0.774), ethnicity (p = 0.200), and gender (p = 0.332) were not associated with medication compliance. This is unlike the findings of Borah et al’s study, which found that older patients were more likely to be compliant to dementia medications (OR 1.401, p < 0.001).(10) In the same study, male gender was also found to be positively associated with compliance to AD medications (OR 1.175, p < 0.05).(10)
Patients with AD are generally older and more susceptible to medication non-compliance issues,(22-24) especially as cognitive impairment progresses. The main reason for non-compliance in our study was patients’ and caregivers’ perceptions that memory loss is a natural ageing process and that medical treatment for AD is less important than treatment for other chronic diseases, such as hypertension, diabetes mellitus and dyslipidaemia. This dismissal of AD treatment is supported by studies, which showed that perception has a significant influence on patients’ compliance to medications.(25) Furthermore, Singaporeans tend to perceive dementia as part of ‘normal ageing’ and ‘a stigmatised mental illness’;(26) this view is supported by a previous study on perception of dementia in Singapore.(27) Hence, a multidisciplinary approach is necessary to educate patients and their caregivers about the importance of medication compliance and to aid patients in understanding their medical condition. This can be in the form of pharmacists’ engagement, where pharmacists play an active role in educating and raising awareness of AD among patients seen at the General Memory Clinic. In Japan, this approach has been shown to be effective in reducing medication non-compliance by 50%–70%.(28) Patient and caregiver education can also be achieved through web-based intervention, such as the use of videos to improve understanding of the importance of medication compliance.(28)
In terms of therapy-related factors, seven of our patients were non-compliant due to side effects from the AD medications. Of these, six patients suffered gastrointestinal and cerebral side effects from donepezil use. Side effects as a contributing factor for non-compliance has been reported in several studies conducted in Asia and Europe.(29,30) Thus, it may be necessary to explore new drug delivery methods so as to improve medication compliance among AD patients. In the present study, a majority (n = 32, 86.5%) of the non-compliant patients were prescribed a once-daily donepezil tablet. Apart from the once-daily normal film-coated donepezil tablet, the donepezil orodispersible tablet has been shown to have a lower incidence of gastric side effects and transdermal rivastigmine has been found to improve adherence.(25) Comparing transdermal patch application of rivastigmine to the capsule formulation, the patch has shown increased tolerance, consistent drug delivery and ease of titration with improved efficacy at lower doses.(25) Better treatment efficacy may indirectly play a role in improving patients’ compliance to medication.(31) For instance, Molinuevo and Arranz showed an improvement in compliance to AD medications using patches instead of oral tablets or capsules.(32)
Regarding condition-related factors, caregivers and patients with comorbidities perceived comorbidities as being more critical than memory loss and dementia. Cardiovascular comorbidities and other chronic conditions such as diabetes mellitus are managed with several medications, resulting in the issue of polypharmacy in this group of patients. While no direct epidemiological studies for AD patients are available locally, the WiSE study conducted in Singapore suggested that diabetes mellitus, ischaemic heart disease and hypertension may be the common comorbidities among AD patients.(33) In view of this perception, interventions should involve equipping patients and caregivers with knowledge about dementia, the importance of medication compliance and the implications of progressive deteriorating AD. The involvement of caregivers is crucial, especially for severe AD patients, who might not have the autonomy to make decisions regarding treatment and medication use. A systematic review has reported successful interventions in caregiver’s education and subsequent improvement in the medication compliance level of AD patients.(18)
In the present study, only one patient was non-compliant due to the high cost of medications (socioeconomic factor). Despite the small number, it is important to consider socioeconomic factors as a component for assessment of compliance in AD patients. A study conducted in India found that the high cost of medications was associated with non-compliance.(19) In terms of healthcare financing, Singapore adopts a co-payment model, with a medical savings account.(34) In Singapore, the amount of medication subsidies depends on the financial classification of the medications; medications under the Standard Drug List (SDL) or Medication Assistance Fund are heavily subsidised by the government, while medications classified as ‘non-standard’ are not subsidised.(35) While donepezil is an SDL drug, rivastigmine and memantine remain as non-standard drugs. Apart from medication costs, dementia treatment itself incurs high societal and direct/indirect individual costs, as revealed by a systematic review.(36) In 2013, the total cost of dementia in Singapore was estimated at SGD 532 million, with an annual cost per person of approximately SGD 10,245.(37) This high societal cost will inevitably translate to high treatment and medication costs for patients and their caregivers. This suggests the need for cost-effectiveness analysis to be conducted in Singapore, as well as interventions to improve medication compliance that would take into account both direct and indirect costs.
The present study showed that around 60% of non-compliant patients persisted in treatment for less than six months, with a mean duration of treatment of around ten months. This was in marked contrast with the results of a Taiwanese study, which showed a mean treatment duration of around 28 months.(20) This contrast illustrates the fact that it is essential to analyse and understand the factors leading to non-compliance that are unique to each society.
We have identified several factors leading to medication non-compliance, including patient and caregiver perceptions, side effects of medications, treatment efficacy and cost of medications. We opine that a multifaceted approach will be most effective at improving compliance in patients with multiple risk factors influencing their behaviour toward medication use.(21) This can be conducted in the form of a collaborative care model involving the following stakeholders:(38) (a) physicians who optimise medications and other behavioural therapies to ensure optimal treatment efficacy for the patient; (b) clinical psychologists who educate the patients on the importance of AD treatment and its implications; (c) pharmacists who manage the drug regimen, educate patients on side-effect management, and monitor medication use through building rapport with the patient and caregivers; and (d) social workers who manage the financial aspects of treatment and medications for AD patients with financial difficulties.
In 2017, a group of pharmacists who implemented a collaborative care model in the management of diabetes mellitus in Singapore reported an improvement in several humanistic and economic outcomes.(39) This form of collaborative care model can be adopted in the management of AD patients with the aims of concurrently improving medication compliance as well as humanistic/economic outcomes, the latter of which play an indirect role in ensuring that AD patients comply with medication use.
The present study was not without limitations. Firstly, as the study measured medication compliance indirectly based on the renewal of previous prescription within 60 days, we were unable to determine the patients’ actual use of AD medications. However, we opine that the duration of 60 days remained reasonable in our study context, as it is the average follow-up duration between visits for dementia patients at National University Hospital, and previous studies have also adopted durations that were specific to their study context.(15-17,40) Secondly, the study was limited by incomplete information from hospital records on patients’ lifestyle and social history, and other potential confounders. For example, patients might have obtained their prescription from other healthcare institutions, which we do not have data on. Patients might have also accumulated medications prescribed after hospitalisation and hence did not fill their outpatient prescription. To minimise the effect of this limitation, we contacted caregivers via the telephone to obtain information about the factors leading to the patients’ non-compliance to medications. In addition, the patients’ physical case notes were reviewed to ensure minimal missing data. Thirdly, the sample size of our study may not be large enough to yield small but statistically significant associations with demographic factors. Furthermore, patients discharged from regular follow-up with the General Memory Clinic (either to another clinical provider or outpatient community care) were considered to be compliant to medication use. This might have resulted in an underestimation of non-compliance, because subjects who became non-compliant while under the care of another clinical provider or outpatient community clinic would not have been counted as non-compliant subjects. In view of this limitation, compliance was tracked to the time-point at which the patient was discharged to another clinical provider.
Despite these limitations, the present study, being the first such study in Singapore, provides a good descriptive overview of factors leading to non-compliance to AD medications. It may serve to inform future practice in Singapore, catering to the needs generated by the unique sociocultural background of Singaporeans. Moving forward, this study may also provide a strong foundation for future behavioural and needs assessment of caregivers of AD patients, as well as for evaluation of the clinical, humanistic and economic outcomes of non-compliant AD patients.
In conclusion, AD significantly affects the patient’s quality of life,(25) and hence compliance to medications for dementia is of utmost importance. In this study, we determined the reasons for non-compliance to AChEIs and NMDA receptor antagonist, as well as the time-point of treatment discontinuation. The results showed no association between demographic characteristics and compliance to medication use, whereas the perceptions about dementia among patients and their caregivers played a major role. Further studies should be conducted to identify other reasons for non-compliance to AD medications. A multidisciplinary approach in educating patients and their caregivers about the importance of treatment and medication use is crucial, and the involvement of pharmacists should be considered, as it has been shown to improve compliance to medications.(41)