Singapore Med J 2022; 63(5): 274-282 doi: 10.11622/smedj.2020137
Mentoring a surgical team towards procedural competence in the early learning curve for selective fetoscopic laser photocoagulation
Lalitha Natarajan1,2, MD, MRCOG, Arundhati T Gosavi2,3, MRCOG, Tuangsit Wataganara4, MD, Lin Lin Su2,3, MRCOG, Zubair Amin5, MHPE, Tak Yeung Leung6, MD, FRCOG, Mahesh Choolani2,3, FRCOG, PhD, Arijit Biswas2,3, MD, FRCOG, Citra NZ Mattar2,3, MRANZCOG, PhD
Author Information >Copyright and License information >
1Fetal Medicine Unit, PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India 2Department of Obstetrics and Gynaecology, National University Health System, Singapore 3Department of Obstetrics and Gynaecology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore 4Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Faculty of Medicine, Siriraj Hospital, Bangkok, Thailand 5Department of Neonatology, National University Health System, Singapore 6Department of Obstetrics and Gynaecology, Faculty of Medicine, the Chinese University of Hong Kong, Shatin, Hong Kong SAR, China Correspondence: Dr Citra Mattar, Consultant, Department of Obstetrics and Gynaecology, Yong Loo Lin School of Medicine, National University of Singapore, NUHS Tower Block, Level 12, 1E Kent Ridge Road, Singapore 119228. citramattar@nus.edu.sg
Selective fetoscopic laser photocoagulation (SFLP) for twin-to-twin transfusion syndrome (TTTS) is challenging for new surgeons at the start of their learning curve. We described an approach utilising telementoring and team-based training to facilitate rapid attainment of the skills required for safe and efficient practice with a limited caseload.
METHODS
We conducted a prospective observational study of SFLP performed by the novice primary surgical team in three stages: under direct on-site supervision from an expert mentor (Group 1), with remote tele-guidance from that mentor (Group 2) and independently (Group 3), at an academic tertiary hospital in Singapore. The primary team undertook regular training on high-fidelity tissue models to accelerate skills acquisition and complement the surgical performance.
RESULTS
9 patients diagnosed with Stage 2 TTTS were assessed for procedural characteristics, surgical outcomes and perinatal survival following SFLP. There were no significant differences in operative duration, anastomoses ablated, gestational age or birth weight at delivery. The complications observed were: recurrent TTTS (22.2% of pregnancies), twin anaemia polycythaemia sequence (33.3%), preterm prelabour membrane rupture (22.2%) and delivery at < 32 weeks (44.4%). ≥ 1 twin was live-born in 88.9% of cases, while postnatal survival to six months of ≥ 1 twin occurred in 77.8% of cases.
CONCLUSION
Systematic mentoring and specialised skills training are useful in aiding new surgeons to negotiate the steep learning curve and achieve good outcomes at the start of a new practice, particularly in the setting of low patient numbers. This is best paired with dedicated model training to achieve and maintain surgical dexterity for this complex procedure.
Monochorionic twinning affects 30% of multiple pregnancies, while twin-to-twin transfusion syndrome (TTTS) occurs in 10%–15% of monochorionic diamniotic (MCDA) pregnancies, with an untreated mortality of 70%–100%.(1,2) TTTS results in unilateral blood transfusion from the donor to the recipient twin, mostly via arteriovenous anastomoses (AVAs), causing oligohydramnios from the hypovolaemic and oliguric donor, and polyhydramnios from the hypervolaemic recipient. This can progress eventually to cardiac failure and the eventual death of one or both twins.(2) Of the various treatments offered for TTTS, only selective fetoscopic laser photocoagulation (SFLP) of causative AVAs at the inter-twin vascular equator is potentially curative and permits the rescue of both twins (compared to selective reductive techniques that cause the death of one twin), and in experienced centres, is associated with a 75% chance of survival of both twins.(3,4) Twin anaemia polycythaemia sequence (TAPS), caused by slow blood transfusion through a few small-calibre (< 1 mm) placental AVAs, may complicate SFLP and result in anaemia and polycythaemia of the donor and the recipient twins, respectively.(5) SFLP has been available in Singapore at two tertiary maternity units since 2011 and 2015; both have published perinatal outcomes from their initial experiences that were comparable to international reports.(6,7) Prior to this, patients with affected pregnancies were offered palliative therapies or referral to a regional fetal therapy centre for SFLP, options that delay the institution of definitive treatment and substantially inflate expenses. The initiation of this advanced fetal therapy service at two Singapore hospitals has ensured that SFLP is accessible to local and foreign affected patients for whom it is the best therapeutic option.
SFLP is a complex procedure that has been associated with a steep learning curve and significant maternal and fetal morbidity.(8-10) As with the majority of complex surgeries, the acquisition of skills in SFLP usually follows the traditional path of surgical apprenticeship vis-a-vis close observation, followed by progressive hands-on performance under direct supervision.(11,12) This classic training model is less time- and cost-efficient for new fetal therapy centres, and may limit patient access to SFLP.(13) We have experienced similar challenges as other low-volume fetal therapy centres in terms of negotiating the long surgical learning curve while achieving procedural aptitude, maintaining competent and safe practice with a limited number of patients (not meeting the suggested minimum of 25 annual procedures)(10) and providing rapid access to SFLP to an underserved population.(7,13) This is a common experience, given that 48% of fetal laser surgery centres, mostly situated in Asia, Australia and South America, perform under 20 procedures annually.(14)
To overcome these limitations, a ‘collaborative surgical services’ model has been proposed, in which personnel and resources are pooled and shared to improve timely access to surgery and quality care in low-volume centres.(13) New models of surgical training are designed to emulate the benefits of traditional surgical apprenticeship, especially the skills-focused training supervised by a surgeon-mentor, while minimising the cost of specialist surgeons spending time away from their primary clinical practice, including expenditures incurred in temporary relocation and lost manpower. These models utilise teleconferencing advances to bring the expert to the surgical team across geographical barriers, employing the mentoring process in the primary clinical setting to assist the surgical team in adopting new procedures successfully.(15-18) Continued off-site mentoring after the initial training phase, combined with skills practice on high-fidelity models and competence-based assessments, can be an effective strategy to overcome the aforementioned situational limitations and ensure that procedural competence is maintained beyond the period of formal training.(19-22)
We have previously described our team-based approach to implementing SFLP, which relied on model practice and stepwise skills learning with an on-site (‘hands-off’) proctor for the first three cases performed at our institution.(7) We herein discuss a natural extension of this arrangement to include continued off-site mentoring for the second phase of cases, leading to independent surgery without a stand-by mentor, updating the ‘see one, do one, teach one’ approach.(23-25) We compared the outcomes and complications of our first nine cases to determine the utility of this collaborative approach as an alternative to the lengthy and costly surgical apprenticeship model.
METHODS
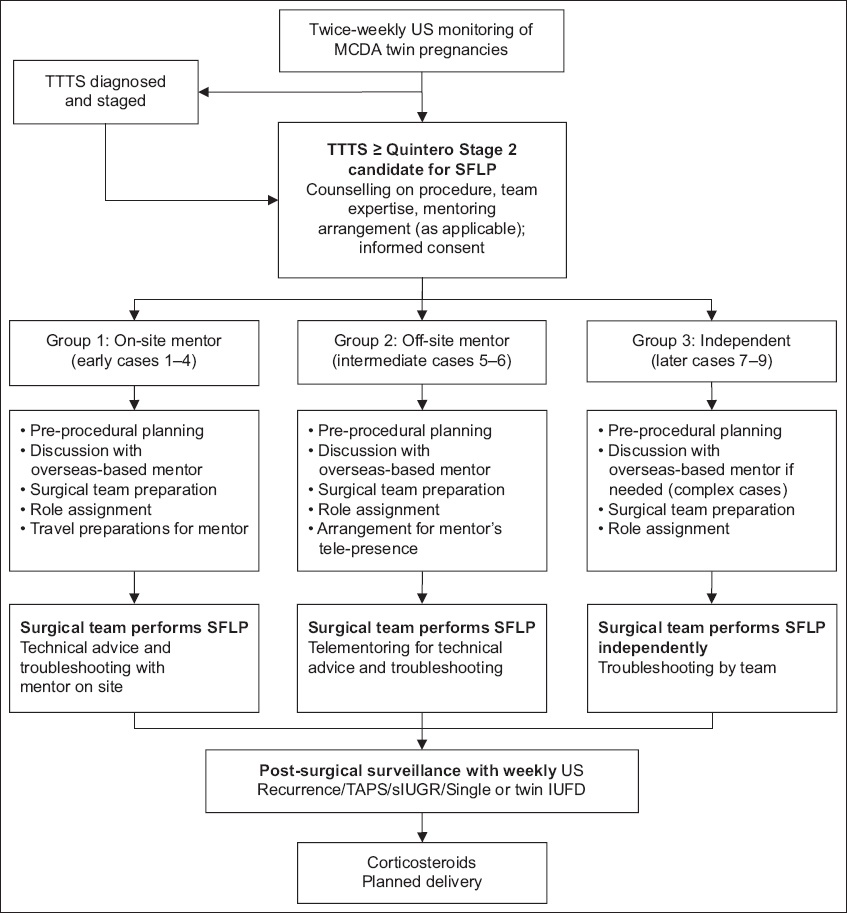
Patients diagnosed with MCDA twin pregnancies at booking visits were monitored fortnightly from 16 weeks’ gestation for TTTS, which was diagnosed and staged using the Quintero criteria (Fig. 1).(1,26-29) All patients were offered combined first-trimester screening at 11.0–13.9 weeks or non-invasive prenatal testing according to the clinical protocol, followed by early anatomic survey at 18 weeks. Inter-twin discordance in nuchal translucency of > 20%, crown-rump length > 10%, nuchal translucency > 95th centile, or cardiac dysfunction in one twin were considered as early indicators of TTTS based on meta-analyses of MCDA biomarkers.(30,31) Patients with Stage 1 TTTS were monitored at least twice weekly for clinical progression, including cardiac failure in the recipient twin,(29) and were offered SFLP based on the following criteria: (a) at least Stage 2 TTTS; (b) gestational age < 26 weeks; and (c) the absence of perinatally lethal structural or genetic anomalies in either fetus. Patients were extensively counselled regarding the diagnosis, alternative therapeutic options and potential complications of SFLP.(3) The multidisciplinary team consisted of fetal therapists, maternal-fetal medicine specialists, obstetric anaesthetists, nurse specialists and administrative support staff, who had prepared for this clinical service together with workflow drills and training on high-fidelity models.(7,19) Patients were informed upfront about the relative inexperience of the surgical team and the on-site or telepresence of the overseas-based surgeon-mentors for support and supervision. All patients provided written informed consent for the SFLP, video recording, photography and placental dye studies, and agreed to the mentoring arrangement. Pre-procedural planning involved placental and vascular equator mapping to determine the point of fetoscope entry.(7,19) Surgery was scheduled as soon as the mentor could travel to our centre; when this was not possible, real-time telementoring was arranged via multiple-user internet teleconferencing applications Skype (Skype Technologies SARL, Palo Alto, CA, USA) and WhatsApp (WhatsApp Inc, Mountain View, CA, USA) over fourth-generation (4G) broadband cellular networks, as the operating room was not equipped for formal videoconferencing. Fetoscopic images were captured directly from the screen and transmitted to the mentor, who was able to follow the entire surgery and advise on the proceedings. Patients diagnosed with TTTS who underwent SFLP were assigned into Groups 1–3 chronologically. The first cases were performed with a mentor on-site (Group 1) and the last cases were performed by the primary surgical team independently (Group 3). Cases 5 and 6 (Group 2) were performed by the team with the mentor observing remotely (i.e. telementoring) to assist with technical difficulties.
Fig. 1
Procedural flowchart shows the diagnosis and staging of patients with twin-to-twin transfusion syndrome (TTTS) who underwent selective fetoscopic laser photocoagulation (SFLP). IUFD: intrauterine fetal death; MCDA: monochorionic diamniotic; sIUGR: selective intrauterine growth restriction; TAPS: twin anaemia polycythaemia sequence
All procedures were performed under general anaesthesia in anticipation of a potentially lengthy surgery. Patient position and choice of fetoscope (curved or straight; Karl Storz Endoskope Berlin GmbH, Berlin, Germany) were determined by placental location, and surgical team members performed specific roles, as previously described.(7,19) Selective ablation of all identified AVAs along the vascular equator was achieved using a 400-μm or 600-μm diode laser at 15–30 W (Medilas D Multibeam; Dornier MedTech Asia, Singapore), followed by ablation of residual superficial anastomoses across the vascular equator from one placental margin to the other (Solomon technique), if technically feasible, to minimise the risk of post-SFLP TAPS.(32) Bleeding from ablated AVAs was handled using coagulation of feeder vessels and by applying transabdominal pressure to achieve a tamponade effect. Amnioreduction was performed at the end of the procedure from the recipient twin sac in all cases until the deepest vertical pocket reached ~4 cm. Cervical length and dilatation were assessed using transperineal ultrasonography (US). After the procedure, patients were observed in the ward for 48 hours, followed by repeat US before discharge. All patients were placed on a short course of prophylactic oral antibiotics and tocolytics (nifedipine and indomethacin) to maintain uterine quiescence.
Patients were followed up with weekly US monitoring for resolution of TTTS features such as re-accumulation of donor twin amniotic fluid and improved recipient twin cardiac function. Umbilical artery and middle cerebral artery Doppler studies were performed to assess placental function, developing anaemia and cardiac dysfunction. US surveillance for procedure- and monochorionicity-related complications continued once to twice weekly, particularly for persistent TTTS, TAPS and selective fetal growth restriction. Placental dye injection was performed, as previously described, to assess completeness of laser ablation.(33)
Ethical approval for collection and use of human data was granted by the National Healthcare Group Domain Specific Review Board (reference no. DSRB/2017/01128). Statistical analysis was performed using GraphPad Prism version 6.04 (GraphPad Software Inc, La Jolla, CA, USA). Data was expressed as median and range. Groups were compared using two-way analysis of variance with Tukey correction for multiple comparisons. Statistical significance was set at p < 0.05.
RESULTS
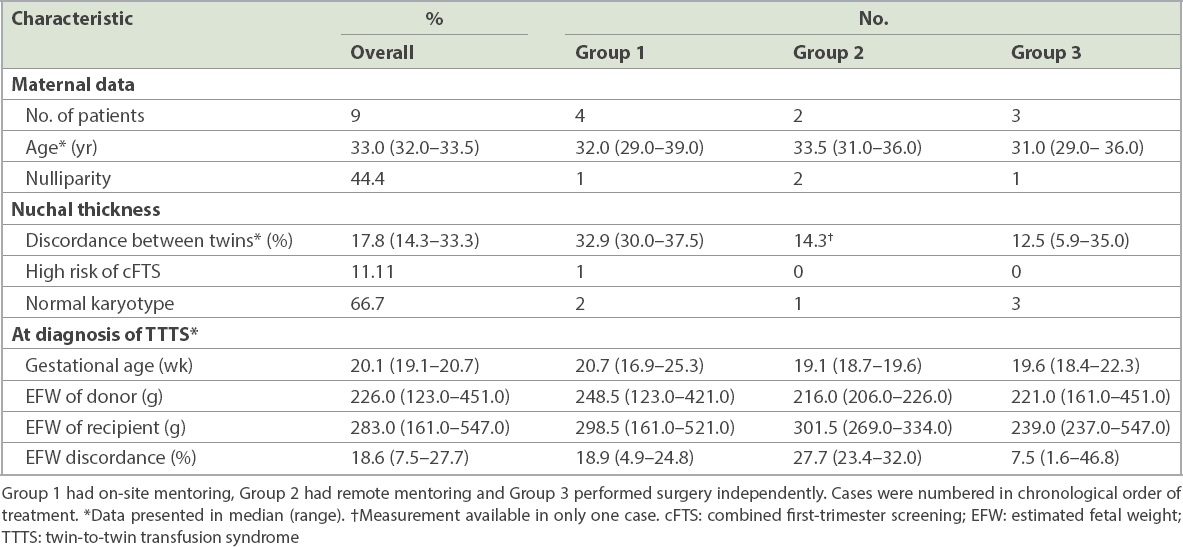
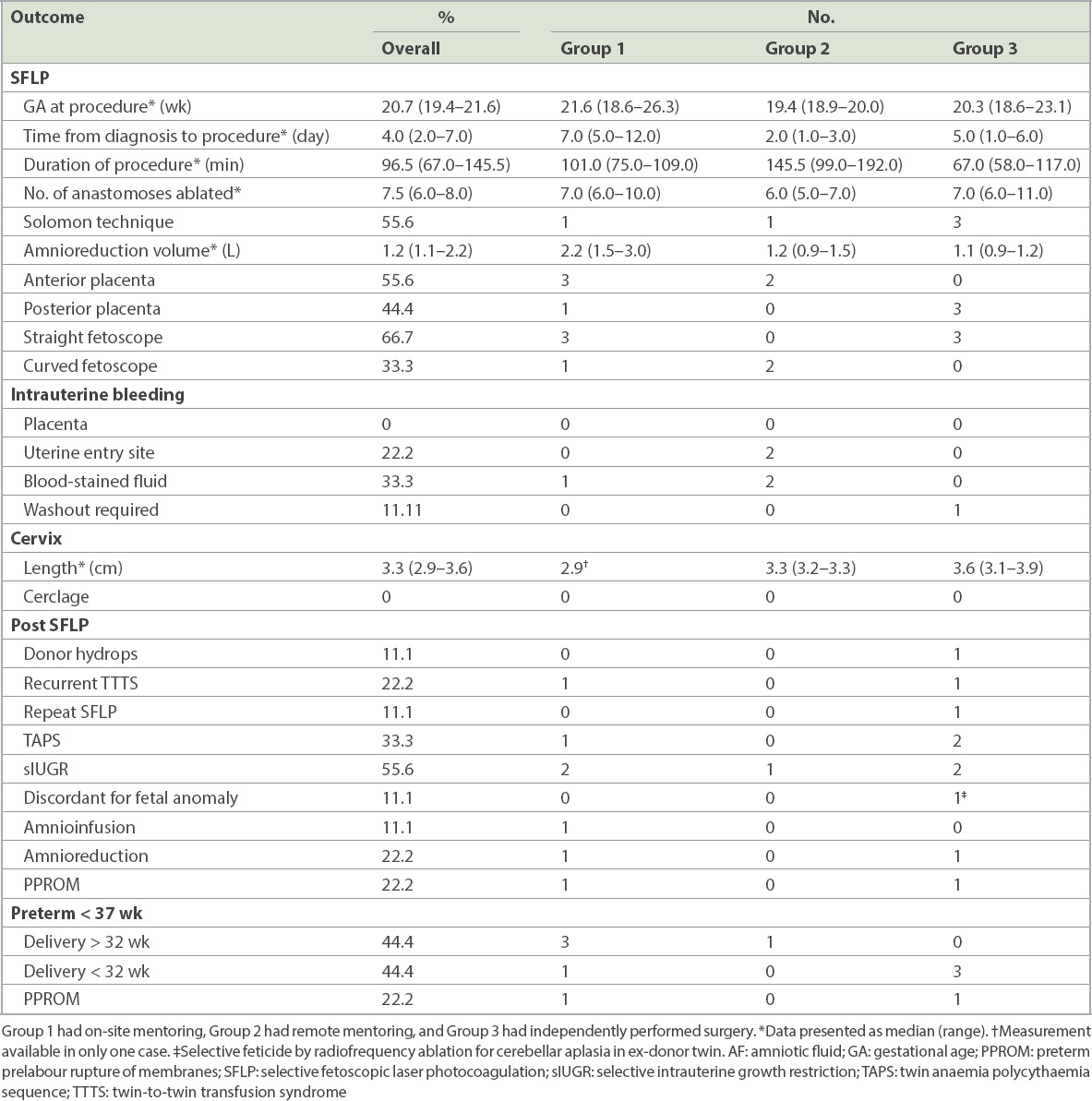
Between 2015 and 2017, nine pregnancies that were complicated by Stage 2 TTTS were treated with SFLP (Table I). Cases 1–4 were performed under on-site supervision by the surgeon-mentor (Group 1), Cases 5 and 6 were performed under off-site supervision via real-time videoconferencing (Group 2) and Cases 7–9 were performed independently with the expert proctor available by telephone for troubleshooting (Group 3). There were no demographic differences between the groups. The median gestational age (GA) at TTTS diagnosis was 20.1 (range 19.1–20.7) weeks. SFLP was performed at a median GA of 20.7 (19.4–21.6) weeks (Table II). The median diagnosis-to-procedure time was 4.0 (2.0–7.0) days, with lower intervals in Group 2 (2.0 [range 1.0–3.0] days) and Group 3 (5.0 [range 1.0–6.0] days) compared to Group 1 (7.0 [range 5.0–12.0] days).
Table I
Patient and fetal characteristics at diagnosis of TTTS.
Table II
Surgical outcomes.
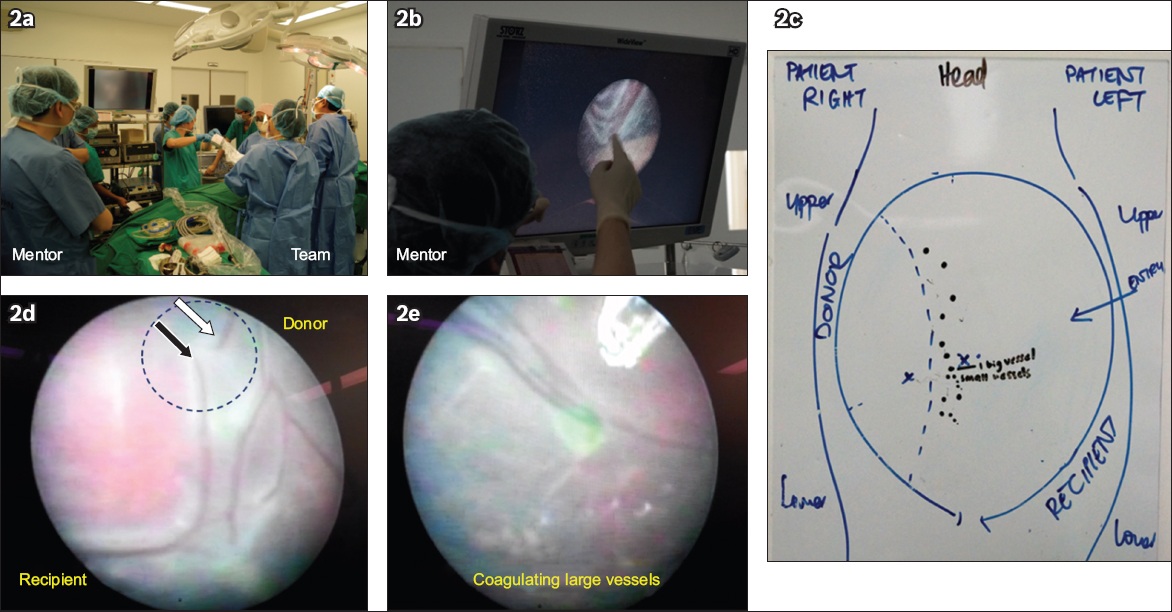
The mentor’s advice on team and equipment organisation (Fig. 2a), fetoscope entry, identification and photocoagulation of individual AVAs at the vascular equator (Fig. 2b) assisted the primary surgical team in completing the surgery and troubleshooting complications (e.g. placental-site bleeding). Residents recorded the locations of AVAs within the recipient twin amniotic sac during the initial fetoscopic end-to-end examination of the vascular equator (Fig. 2c). Detailed evaluation was performed after each surgery with critical feedback on the team’s performance and improvements required. When telementoring arrangements were required on challenging cases, real-time images were continuously provided to the remote mentor using a mobile smartphone and 4G Internet connection (Figs. 2d & e). The image quality provided was generally satisfactory for the mentor to confirm the correct anastomoses (if the appearance raised doubts) and to advise a suitable approach for large vessels at risk of rupture. The mentor stayed online throughout the surgery.
Fig. 2
Photographs show on-site mentoring and telementoring during the first cases of selective fetoscopic laser photocoagulation (SFLP). (a) The primary surgical team was mentored in a hands-off manner, with a focus on team organisation and (b) completing SFLP efficiently and safely, especially in technically demanding situations (e.g. on large vessels). (c) Residents recorded the locations of arteriovenous anastomoses (black circles) within the recipient twin amniotic sac during the initial fetoscopic end-to-end examination of the vascular equator. (d) For telementoring, fetoscopic images were filmed directly from the screen using a mobile device and sent to the mentor via the internet through the course of the surgery. Good image quality was obtained, allowing the telementor and team to identify outlying anastomoses with the donor or recipient origins of vessels (arrows) and (e) carefully ‘shave’ larger vessels with photocoagulation to prevent rupture or bleeding.
The median duration of surgery was 96.5 (67.0–145.5) minutes (Table II). 5–11 AVAs were ablated in each patient. Large vessels were carefully ablated by ‘shaving’ the girth of the vessels from the periphery inwards and by coagulating the smaller feeder vessels to achieve satisfactory cessation of blood flow.(19) The main complications were brisk bleeding from uterine vessels that were lacerated upon entry; haemostasis was achieved by applying pressure with the fetoscope under direct vision. The Solomon technique was performed under direct supervision in Cases 3 and 6, and in all cases in Group 3 to minimise the risks of TTTS recurrence and TAPS. It was not performed in Cases 1, 2, 4 or 5, because the primary team decided that it would have been too technically demanding. No other adverse outcomes (e.g. placental abruption or hysterectomy) were encountered. Transient donor hydrops was observed in Case 8 within the first week after SFLP and resolved spontaneously.(34)
Cases 5 and 9 had persistent oligohydramnios and absence of the urinary bladder in the donor twin following satisfactory AVA ablation, with eventual re-accumulation of polyhydramnios in the recipient twin, and were classified under recurrent TTTS (incidence 22.2%, Table II). Both cases required amnioreduction from the recipient sac within a week of SFLP, which in Case 5, preceded preterm membrane rupture and emergency Caesarean delivery at 27.1 weeks, approximately 1.9 weeks post SFLP. In Case 9, post-SFLP sonographical surveillance showed rapidly progressing Stage 3 TTTS, with abnormal placental blood flows in the donor fetus and evidence of cardiac strain in the recipient fetus, requiring repeat SFLP. This was performed at another regional fetal centre that was better equipped to perform the complex surgery. Two large central anastomoses that had originally been ablated had recannulated, causing recurrence and were successfully re-ablated. The patient was eventually delivered for progressively abnormal placental blood flows. Three cases of TAPS that were diagnosed sonographically (Cases 2, 7 and 8, incidence 33.3%) were managed expectantly.(5)
Selective intrauterine growth restriction (sIUGR) was diagnosed in Cases 2, 4, 5, 7 and 9 based on > 25% intertwin discordance from the estimated fetal weight (range 25.3%–46.8%).(35) Case 2 was complicated by TAPS, while in Case 4, intrauterine death of the growth-restricted twin occurred at approximately 32 weeks. The incidence of sIUGR was 55.6% (n = 5) out of nine patients. The incidence of preterm prelabour membrane rupture (PPROM) was 22.2%. One sibling twin (Case 7) was selectively terminated post SFLP upon diagnosis of a serious structural anomaly by radiofrequency ablation.(36) The prenatal loss rate of at least one fetus was 33.3% (n = 3) and the loss rate of both fetuses was 11.1% (n = 1; Table III).
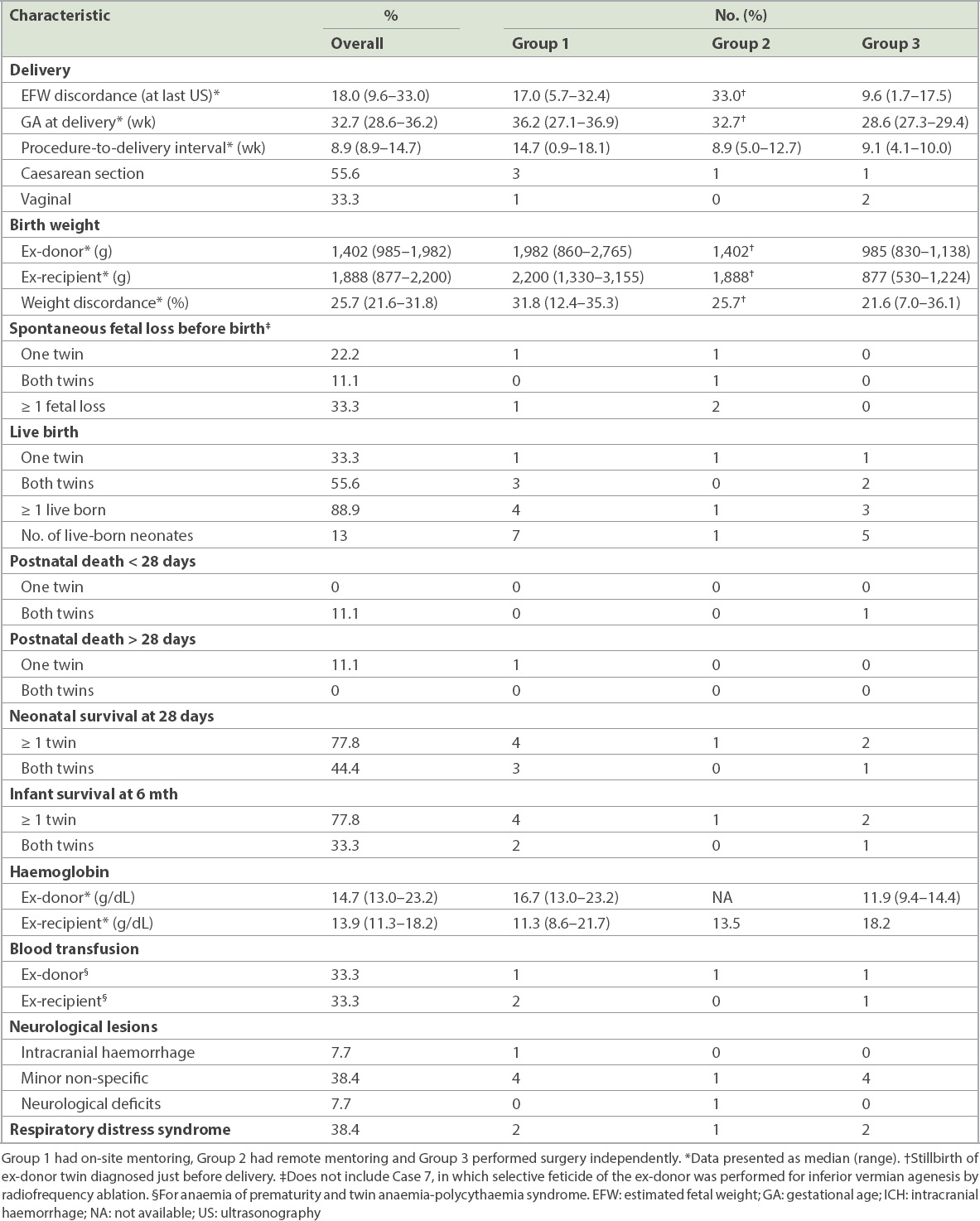
Table III
Survival characteristics.
There were no significant differences in postnatal outcomes between the groups. There were trends towards lower GA at delivery, shorter procedure-to-delivery intervals and lower birth weight in both twins in Group 3 compared to Group 1 (Table III). Survival of at least one twin to birth was 88.9% (n = 8), with double survival in 55.6% (n = 5) of all pregnancies treated. All were born preterm at < 37 weeks, with 44.4% delivered at < 32 weeks. The median ages at delivery were similar: 36.2 (range 27.1–36.9) weeks (Group 1), 32.7 weeks (Group 2, single survivor) and 28.6 (range 27.3–29.4) weeks (Group 3). The median procedure-to-delivery interval was 8.9 (8.9–14.7) weeks, with a trend towards shorter intervals in Groups 2 and 3 (Table III).
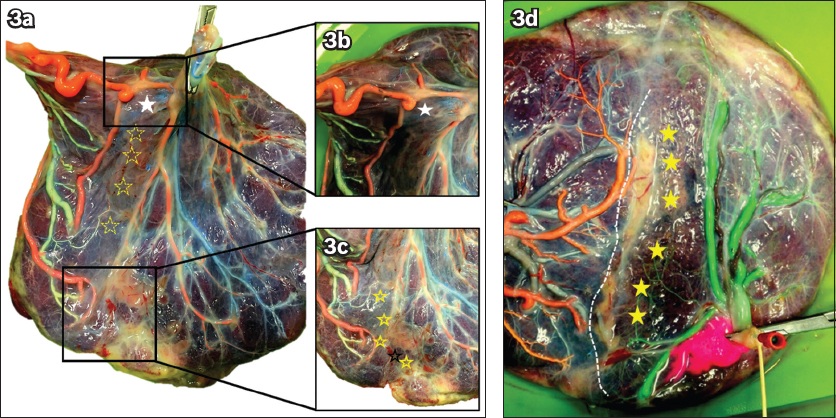
Placental dye injections were performed in every case in which patients gave consent to identify arteries and veins from donors and recipients. Six placentas were examined after birth for residual anastomoses (Figs. 3a–d), excluding Case 7 (declined consent), and Cases 6 and 9 (delivered overseas). A partially recannulated AVA between the proximately sited cords was observed in Case 5 (recurrent TTTS, white star in Fig. 3a & b), while the remaining AVAs were successfully coagulated (yellow stars in Figs. 3a & c). The other placentas showed no obvious residual anastomoses (yellow stars in Fig. 3d) and satisfactory Solomon ablation (broken line in Fig. 3d).
Fig. 3
Photographs show the results of placental dye injections performed to determine the accuracy of selective fetoscopic laser photocoagulation, identifying (a) AVAs (yellow stars); (b) recannulated AVAs, which, in this case, were the cause of recurrent twin-to-twin transfusion syndrome (white star in a & b); and in optimally completed procedures, (c & d) individually ablated AVAs (yellow stars) followed by superficial ablation of residual anastomoses (broken line in d). AVA: ablated arteriovenous anastomosis
Survival of at least one twin was observed in 77.8% of pregnancies at both 28 days and six months, and 33.3% of pregnancies had both twins surviving at six months (Table III). One twin pair and one ex-recipient died at seven days and 49 days, respectively, from prematurity-related respiratory distress syndrome. Neonatal complications included spastic cerebral palsy (7.7%, one out of 13 infants) and benign intraventricular changes (66.7%) in six infants who had normal neurological outcomes at 8–35 months of age.
DISCUSSION
This report illustrates the usefulness of a collaborative effort to introduce a new complex surgery while maintaining safety and producing satisfactory outcomes. Prior to establishing SFLP locally, patients with treatable TTTS were referred to regional centres; these arrangements, commonly self-funded, result in delayed treatment and represent an unsustainable solution, particularly when surgery is needed urgently. The conventional apprenticeship model requires resources for surgical training and a minimal case-load (25–75 procedures) to attain proficiency.(8,10) Outcomes reflect individual and institutional learning curves that are influenced by the clinical team working collectively to manage the patient.(37) While achievable in high-volume centres, successful adoption of SFLP is a real challenge in a low-volume clinic servicing a much smaller population.(13) Thus, we adapted a collaborative model utilising on-site mentoring and telementoring with model practice to achieve these goals. This review of our initial outcomes in the early part of the learning curve is important to validate the safety and efficacy of this approach.
We worked closely with two regionally based fetal surgeon mentors who were able to travel quickly and teleconference easily across negligible time differences. The primary team acquired basic fetoscopy skills through model training, as no local surgeon had undergone a full fetoscopy apprenticeship.(19) These arrangements proved particularly helpful in the first cases that presented technical challenges (i.e. anterior placentas, large vessels), which were overcome with much greater efficiency under direct supervision of the mentor,(7) and in post-SFLP management for recurrent TTTS and TAPS.(19) There were greater procedural delays for Group 1, as travel arrangements had to be made for the overseas mentor, and these first cases predictably took the primary team longer to organise. The duration of surgery was the longest for Group 2, as these cases were complicated by anterior placentae and significant intrauterine bleeding. Placental dye injections enabled reflection and continuous learning from the unsuccessful cases.
Survival rates in our preliminary series are comparable to those in the published literature, including survival rates for pregnancies with at least one live birth (88.9% vs. 70%–88%),(4,14) two survivors (55.6% vs. 35%–74%) and no survivors (11.1% vs. 9.5%–27%),(1,38) respectively. Rates of PPROM, perinatal survival and neonatal death in our cohort were similar to published outcomes.(1,38) Incidences of recurrent TTTS (22.2%) and TAPS (33.3%) were higher than the reported rates of 0%–16% and 2%–13%, respectively.(5,39) This data reflects the primary team’s inexperience in identifying and ablating smaller or more peripheral anastomoses, and in dealing with large AVAs, as well as the small patient numbers in this series.
The approach we used illustrates the prerequisites for a mentoring system to work effectively: the primary team operating efficiently as a single unit (performing all cases together to improve operating efficacy), with each member fulfilling specified functions,(7,16,19) immediate feedback from the mentor, and specific skills reinforced by model practice.(19,40) The proximity of regional centres allowed us to coordinate the entire team, including the overseas mentor, within days. The main limitation to the timely growth of a new fetal therapy centre is a caseload that is insufficient to attain and maintain proficiency in the traditional sense.(41) As our centre services a small population with a low birth-rate, it will not easily meet the conventional numeric requirements for institutional competence in uncommon procedures.(42) This solution gives the primary team the confidence to proceed with service provision without compromising patients’ rapid access to SFLP within the existing healthcare system, and can be adapted to provide accessible advanced therapies at similar low-volume centres.
While surgical apprenticeship is the accepted practice,(11) it is inadequate in itself to meet the increasing demand for SFLP at low-volume centres.(43,44) Skills acquisition as a surgical team and effective mentor-mentee communication were the critical factors in the success of the collaborative model driven by patient and institutional needs and can be applied to other complex surgical therapies.(13,45) Mentoring beyond the apprenticeship period provides continued benefit,(18,46) resulting in fewer clinical errors, complications and mortality.(47,48) We acknowledge that although this is a promising approach to skills acquisition for new techniques, our numbers are small and hence, further studies with larger numbers are required to reinforce our conclusions.
ACKNOWLEDGEMENTS
We would like to thank Zhenzhi Chen, Pei-Huang Kuan, Sister Li Li Tan, Cecille Arquillo Laureano, Maylene Tan Zipagan and the residents of the Department of Obstetrics and Gynaecology, National University Hospital, Singapore. This work was supported by funding from the Department of Obstetrics and Gynaecology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore.
References Simpson LL.Society for Maternal-Fetal MedicineTwin-twin transfusion syndrome.Am J Obstet Gynecol. 2013;208:3-18. Baschat A, Chmait RH, et al. WAPM Consensus Group on Twin-to-Twin TransfusionTwin-to-twin transfusion syndrome (TTTS).J Perinat Med. 2011;39:107-12. Ropacka M, Markwitz W, Blickstein I.Treatment options for the twin-twin transfusion syndrome:a review.Twin Res. 2002;5:507-14. Quintero RA, Kontopoulos E, Chmait RH.Laser treatment of twin-to-twin transfusion syndrome.Twin Res Hum Genet. 2016;19:197-206. Donepudi R, Akkermans J, Mann L, et al. Impact of cannula size on recurrent twin-twin transfusion syndrome and twin anemia-polycythemia sequence after fetoscopic laser surgery.Ultrasound Obstet Gynecol. 2018;52:744-9. Thia E, Thain S, Yeo GS.Fetoscopic laser photocoagulation in twin-to-twin transfusion syndrome:experience from a single institution.Singapore Med J. 2017;58:321-6. Gosavi A, Vijayakumar PD, Ng BS, et al. Rapid initiation of fetal therapy services with a system of learner-centred training under proctorship:the National University Hospital (Singapore) experience.Singapore Med J. 2017;58:311-20. Morris RK, Selman TJ, Harbidge A, Martin WI, Kilby MD.Fetoscopic laser coagulation for severe twin-to-twin transfusion syndrome:factors influencing perinatal outcome, learning curve of the procedure and lessons for new centres.BJOG. 2010;117:1350-7. Morris RK, Selman TJ, Kilby MD.Influences of experience, case load and stage distribution on outcome of endoscopic laser surgery for TTTS--a review. Ahmed S et al. Prenatal Diagnosis 2010.Prenat Diagn. 2010;30:808-9. author reply 810. Peeters SH, Van Zwet EW, Oepkes D, et al. Learning curve for fetoscopic laser surgery using cumulative sum analysis.Acta Obstet Gynecol Scand. 2014;93:705-11. Lubowitz JH, Provencher MT, Brand JC, Rossi MJ.The apprenticeship model for surgical training is inferior.Arthroscopy. 2015;31:1847-8. Goff BA.Changing the paradigm in surgical education.Obstet Gynecol. 2008;112:2 Pt 1328-32. Edwards AG, Teoh M, Hodges RJ, et al. Balancing patient access to fetoscopic laser photocoagulation for twin-to-twin transfusion syndrome with maintaining procedural competence:are collaborative services part of the solution?.Twin Res Hum Genet. 2016;19:276-84. Akkermans J, Peeters SH, Klumper FJ, et al. Twenty-five years of fetoscopic laser coagulation in twin-twin transfusion syndrome:a systematic review.Fetal Diagn Ther. 2015;38:241-53. Agha RA, Fowler AJ.The role and validity of surgical simulation.Int Surg. 2015;100:350-7. Stepaniak PS, Vrijland WW, de Quelerij M, de Vries G, Heij C.Working with a fixed operating room team on consecutive similar cases and the effect on case duration and turnover time.Arch Surg. 2010;145:1165-70. Snyderman CH, Gardner PA, Lanisnik B, Ravnik J.Surgical telementoring:a new model for surgical training.Laryngoscope. 2016;126:1334-8. Schubert A.Teleconferencing, distance learning, and telementoring:new technology harnessed for perioperative education.J Clin Anesth. 2000;12:250-1. Wataganara T, Gosavi A, Nawapun K, et al. Model surgical training:skills acquisition in fetoscopic laser photocoagulation of monochorionic diamniotic twin placenta using realistic simulators.J Vis Exp. 2018;133. Peeters SH, Akkermans J, Bustraan J, et al. Operator competence in fetoscopic laser surgery for twin-twin transfusion syndrome:validation of a procedure-specific evaluation tool.Ultrasound Obstet Gynecol. 2016;47:350-5. Peeters SH, Akkermans J, Westra M, et al. Identification of essential steps in laser procedure for twin-twin transfusion syndrome using the Delphi methodology:SILICONE study.Ultrasound Obstet Gynecol. 2015;45:439-46. Peeters SH, Akkermans J, Slaghekke F, et al. Simulator training in fetoscopic laser surgery for twin-twin transfusion syndrome:a pilot randomized controlled trial.Ultrasound Obstet Gynecol. 2015;46:319-26. Lenchus JD.End of the “see one, do one, teach one”era:the next generation of invasive bedside procedural instruction.J Am Osteopath Assoc. 2010;110:340-6. Curry JI.'See one, practise on a simulator, do one'- the mantra of the modern surgeon.S Afr J Surg. 2011;49:4-6. Vozenilek J, Huff JS, Reznek M, Gordon JA.See one, do one, teach one:advanced technology in medical education.Acad Emerg Med. 2004;11:1149-54. Sueters M, Middeldorp JM, Lopriore E, et al. Timely diagnosis of twin-to-twin transfusion syndrome in monochorionic twin pregnancies by biweekly sonography combined with patient instruction to report onset of symptoms.Ultrasound Obstet Gynecol. 2006;28:659-64. Linskens IH, de Mooij YM, Twisk JW, et al. Discordance in nuchal translucency measurements in monochorionic diamniotic twins as predictor of twin-to-twin transfusion syndrome.Twin Res Hum Genet. 2012;12:605-10. Kontopoulos E, Chmait RH, Quintero RA.Twin-to-twin transfusion syndrome:definition, staging, and ultrasound assessment.Twin Res Hum Genet. 2016;19:175-83. Van Mieghem T, Lewi L, Gucciardo L, et al. The fetal heart in twin-to-twin transfusion syndrome.Int J Pediatr. 2010;2010:pii:379792. Mackie FL, Hall MJ, Morris RK, Kilby MD.Early prognostic factors of outcomes in monochorionic twin pregnancy:systematic review and meta-analysis.Am J Obstet Gynecol. 2018;219:436-46. Stagnati V, Zanardini C, Fichera A, et al. Early prediction of twin-to-twin transfusion syndrome:systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2017;49:573-82. Slaghekke F, Lewi L, Middeldorp JM, et al. Residual anastomoses in twin-twin transfusion syndrome after laser:the Solomon randomized trial.Am J Obstet Gynecol. 2014;211:285.e1-7. Lopriore E, Slaghekke F, Middeldorp JM, et al. Accurate and simple evaluation of vascular anastomoses in monochorionic placenta using colored dye.J Vis Exp. 2011;55e3208. Gratacós E, Van Schoubroeck D, Carreras E, et al. Transient hydropic signs in the donor fetus after fetoscopic laser coagulation in severe twin-twin transfusion syndrome:incidence and clinical relevance.Ultrasound Obstet Gynecol. 2002;19:449-53. Gratacós E, Lewi L, Muñoz B, et al. A classification system for selective intrauterine growth restriction in monochorionic pregnancies according to umbilical artery Doppler flow in the smaller twin.Ultrasound Obstet Gynecol. 2007;30:28-34. Bebbington MW, Danzer E, Moldenhauer J, Khalek N, Johnson MP.Radiofrequency ablation vs bipolar umbilical cord coagulation in the management of complicated monochorionic pregnancies.Ultrasound Obstet Gynecol. 2012;40:319-24. Ramsay CR, Grant AM, Wallace SA, et al. Assessment of the learning curve in health technologies. A systematic review.Int J Technol Assess Health Care. 2000;16:1095-108. Chmait RH, Kontopoulos EV, Korst LM, et al. Stage-based outcomes of 682 consecutive cases of twin-twin transfusion syndrome treated with laser surgery:the USFetus experience.Am J Obstet Gynecol. 2011;204:393.e1-6. Slaghekke F, Oepkes D.Solomon technique versus selective coagulation for twin-twin transfusion syndrome.Twin Res Hum Genet. 2016;19:217-21. Peyre SE, Ashley SW.Teaching uncommon and highly complex operations:maximizing the teaching and learning.J Gastrointest Surg. 2011;15:1724-5. The Royal Australian and New Zealand College of Obstetricians and GynaecologistsManagement of monochorionic twin pregnancy. C-Obs 42. 2014;. Available at: https://www.ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27s%20Health/Statement%20and%20guidelines/Clinical-Obstetrics/Management-of-Monochorionic-Twins-(C-Obs-42)-review-July-2017.pdf?ext=.pdf. Accessed November 12, 2018. The World BankFertility rate, total (births per woman). Available at: https://data.worldbank.org/indicator/SP.DYN.TFRT.IN. Accessed December 16, 2018. Population Division, Department of Economic and Social Affairs, United NationsWorld Population Prospects:The 2017 Revision.Methodology of the United Nations Population Estimates and Projections, Working Paper No. ESA/P/WP.250. 2017;Accessed December 16, 2018New York, NY United NationsAvailable at: https://population.un.org/wpp/Publications/Files/WPP2017_Methodology.pdf. Accessed December 16, 2018. El-Sabawi B, Magee W, 3rdlastThe evolution of surgical telementoring:current applications and future directions.Ann Transl Med. 2016;4:391. Chan FY.Fetal tele-ultrasound and tele-therapy.J Telemed Telecare. 2007;13:167-71. Bruns NE, Irtan S, Rothenberg SS, et al. Trans-atlantic telementoring with pediatric surgeons:technical considerations and lessons learned.J Laparoendosc Adv Surg Tech A. 2016;26:75-8. Gilbert JH, Yan J, Hoffman SJ.A WHO report:framework for action on interprofessional education and collaborative practice.J Allied Health. 2010;39:Suppl 1196-7. Schmitt MH.Collaboration improves the quality of care:methodological challenges and evidence from US health care research.J Interprof Care. 2001;15:47-66.
REFERENCES
1. Society for Maternal-Fetal Medicine, Simpson LL. Twin-twin transfusion syndrome. Am J Obstet Gynecol 2013; 208:3-18. https://doi.org/10.1016/j.ajog.2012.10.880
PMid:23200164
2. WAPM Consensus Group on Twin-to-Twin Transfusion, Baschat A, Chmait RH, et al. Twin-to-twin transfusion syndrome (TTTS). J Perinat Med 2011; 39:107-12. https://doi.org/10.1515/jpm.2010.147
3. Ropacka M, Markwitz W, Blickstein I. Treatment options for the twin-twin transfusion syndrome: a review. Twin Res 2002; 5:507-14. https://doi.org/10.1375/136905202762341964
PMid:12573181
4. Quintero RA, Kontopoulos E, Chmait RH. Laser treatment of twin-to-twin transfusion syndrome. Twin Res Hum Genet 2016; 19:197-206. https://doi.org/10.1017/thg.2016.28
PMid:27203606
5. Donepudi R, Akkermans J, Mann L, et al. Impact of cannula size on recurrent twin-twin transfusion syndrome and twin anemia-polycythemia sequence after fetoscopic laser surgery. Ultrasound Obstet Gynecol 2018; 52:744-9. https://doi.org/10.1002/uog.18904
PMid:28925589
6. Thia E, Thain S, Yeo GS. Fetoscopic laser photocoagulation in twin-to-twin transfusion syndrome: experience from a single institution. Singapore Med J 2017; 58:321-6. https://doi.org/10.11622/smedj.2016067
PMid:27056209 PMCid:PMC5474527
7. Gosavi A, Vijayakumar PD, Ng BS, et al. Rapid initiation of fetal therapy services with a system of learner-centred training under proctorship: the National University Hospital (Singapore) experience. Singapore Med J 2017; 58:311-20. https://doi.org/10.11622/smedj.2016127
PMid:27439783 PMCid:PMC5474526
8. Morris RK, Selman TJ, Harbidge A, Martin WI, Kilby MD. Fetoscopic laser coagulation for severe twin-to-twin transfusion syndrome: factors influencing perinatal outcome, learning curve of the procedure and lessons for new centres. BJOG 2010; 117:1350-7. https://doi.org/10.1111/j.1471-0528.2010.02680.x
PMid:20670301
9. Morris RK, Selman TJ, Kilby MD. Influences of experience, case load and stage distribution on outcome of endoscopic laser surgery for TTTS--a review. Ahmed S et al. Prenat Diagn 2010; 30:808-9; author reply 810. https://doi.org/10.1002/pd.2549
PMid:20661894
10. Peeters SH, Van Zwet EW, Oepkes D, et al. Learning curve for fetoscopic laser surgery using cumulative sum analysis. Acta Obstet Gynecol Scand 2014; 93:705-11. https://doi.org/10.1111/aogs.12402
PMid:24773155
11. Lubowitz JH, Provencher MT, Brand JC, Rossi MJ. The apprenticeship model for surgical training is inferior. Arthroscopy 2015; 31:1847-8. https://doi.org/10.1016/j.arthro.2015.07.014
PMid:26433232
13. Edwards AG, Teoh M, Hodges RJ, et al. Balancing patient access to fetoscopic laser photocoagulation for twin-to-twin transfusion syndrome with maintaining procedural competence: are collaborative services part of the solution? Twin Res Hum Genet 2016; 19:276-84. https://doi.org/10.1017/thg.2016.24
PMid:27087260
14. Akkermans J, Peeters SH, Klumper FJ, et al. Twenty-five years of fetoscopic laser coagulation in twin-twin transfusion syndrome: a systematic review. Fetal Diagn Ther 2015; 38:241-53. https://doi.org/10.1159/000437053
PMid:26278319
16. Stepaniak PS, Vrijland WW, de Quelerij M, de Vries G, Heij C. Working with a fixed operating room team on consecutive similar cases and the effect on case duration and turnover time. Arch Surg 2010; 145:1165-70. https://doi.org/10.1001/archsurg.2010.255
PMid:21173290
17. Snyderman CH, Gardner PA, Lanisnik B, Ravnik J. Surgical telementoring: a new model for surgical training. Laryngoscope 2016; 126:1334-8. https://doi.org/10.1002/lary.25753
PMid:27010229
18. Schubert A. Teleconferencing, distance learning, and telementoring: new technology harnessed for perioperative education. J Clin Anesth 2000; 12:250-1. https://doi.org/10.1016/S0952-8180(00)00141-0
19. Wataganara T, Gosavi A, Nawapun K, et al. Model surgical training: skills acquisition in fetoscopic laser photocoagulation of monochorionic diamniotic twin placenta using realistic simulators. J Vis Exp 2018; (133). https://doi.org/10.3791/57328
PMid:29630059 PMCid:PMC5933233
20. Peeters SH, Akkermans J, Bustraan J, et al. Operator competence in fetoscopic laser surgery for twin-twin transfusion syndrome: validation of a procedure-specific evaluation tool. Ultrasound Obstet Gynecol 2016; 47:350-5. https://doi.org/10.1002/uog.15734
PMid:26307171
21. Peeters SH, Akkermans J, Westra M, et al. Identification of essential steps in laser procedure for twin-twin transfusion syndrome using the Delphi methodology: SILICONE study. Ultrasound Obstet Gynecol 2015; 45:439-46. https://doi.org/10.1002/uog.14761
PMid:25504904
22. Peeters SH, Akkermans J, Slaghekke F, et al. Simulator training in fetoscopic laser surgery for twin-twin transfusion syndrome: a pilot randomized controlled trial. Ultrasound Obstet Gynecol 2015; 46:319-26. https://doi.org/10.1002/uog.14916
PMid:26036333
23. Lenchus JD. End of the "see one, do one, teach one" era: the next generation of invasive bedside procedural instruction. J Am Osteopath Assoc 2010; 110:340-6.
24. Curry JI. 'See one, practise on a simulator, do one' - the mantra of the modern surgeon. S Afr J Surg 2011; 49:4-6.
25. Vozenilek J, Huff JS, Reznek M, Gordon JA. See one, do one, teach one: advanced technology in medical education. Acad Emerg Med 2004; 11:1149-54. https://doi.org/10.1197/j.aem.2004.08.003
PMid:15528578
26. Sueters M, Middeldorp JM, Lopriore E, et al. Timely diagnosis of twin-totwin transfusion syndrome in monochorionic twin pregnancies by biweekly sonography combined with patient instruction to report onset of symptoms. Ultrasound Obstet Gynecol 2006; 28:659-64. https://doi.org/10.1002/uog.3819
PMid:16969785
27. Linskens IH, de Mooij YM, Twisk JW, et al. Discordance in nuchal translucency measurements in monochorionic diamniotic twins as predictor of twin-to-twin transfusion syndrome. Twin Res Hum Genet 2012; 12:605-10. https://doi.org/10.1375/twin.12.6.605
PMid:19943724
28. Kontopoulos E, Chmait RH, Quintero RA. Twin-to-twin transfusion syndrome: definition, staging, and ultrasound assessment. Twin Res Hum Genet 2016; 19:175-83. https://doi.org/10.1017/thg.2016.34
PMid:27203605
29. Van Mieghem T, Lewi L, Gucciardo L, et al. The fetal heart in twin-to-twin transfusion syndrome. Int J Pediatr 2010; 2010. pii: 379792. https://doi.org/10.1155/2010/379792
PMid:20811613 PMCid:PMC2929591
30. Mackie FL, Hall MJ, Morris RK, Kilby MD. Early prognostic factors of outcomes in monochorionic twin pregnancy: systematic review and meta-analysis. Am J Obstet Gynecol 2018; 219:436-46. https://doi.org/10.1016/j.ajog.2018.05.008
PMid:29763608
31. Stagnati V, Zanardini C, Fichera A, et al. Early prediction of twin-to-twin transfusion syndrome: systematic review and meta-analysis. Ultrasound Obstet Gynecol 2017; 49:573-82. https://doi.org/10.1002/uog.15989
PMid:27270878
32. Slaghekke F, Lewi L, Middeldorp JM, et al. Residual anastomoses in twin-twin transfusion syndrome after laser: the Solomon randomized trial. Am J Obstet Gynecol 2014; 211:285.e1-7. https://doi.org/10.1016/j.ajog.2014.05.012
PMid:24813598
33. Lopriore E, Slaghekke F, Middeldorp JM, et al. Accurate and simple evaluation of vascular anastomoses in monochorionic placenta using colored dye. J Vis Exp 2011; (55):e3208. https://doi.org/10.3791/3208
PMid:21912373 PMCid:PMC3230184
34. Gratacós E, Van Schoubroeck D, Carreras E, et al. Transient hydropic signs in the donor fetus after fetoscopic laser coagulation in severe twin-twin transfusion syndrome: incidence and clinical relevance. Ultrasound Obstet Gynecol 2002; 19:449-53. https://doi.org/10.1046/j.1469-0705.2002.00642.x
PMid:11982976
35. Gratacós E, Lewi L, Muñoz B, et al. A classification system for selective intrauterine growth restriction in monochorionic pregnancies according to umbilical artery Doppler flow in the smaller twin. Ultrasound Obstet Gynecol 2007; 30:28-34. https://doi.org/10.1002/uog.4046
PMid:17542039
36. Bebbington MW, Danzer E, Moldenhauer J, Khalek N, Johnson MP. Radiofrequency ablation vs bipolar umbilical cord coagulation in the management of complicated monochorionic pregnancies. Ultrasound Obstet Gynecol 2012; 40:319-24. https://doi.org/10.1002/uog.11122
PMid:22302774
37. Ramsay CR, Grant AM, Wallace SA, et al. Assessment of the learning curve in health technologies. A systematic review. Int J Technol Assess Health Care 2000; 16:1095-108. https://doi.org/10.1017/S0266462300103149
PMid:11155830
38. Chmait RH, Kontopoulos EV, Korst LM, et al. Stage-based outcomes of 682 consecutive cases of twin-twin transfusion syndrome treated with laser surgery: the USFetus experience. Am J Obstet Gynecol 2011; 204:393.e1-6. https://doi.org/10.1016/j.ajog.2011.02.001
PMid:21411051
39. Slaghekke F, Oepkes D. Solomon technique versus selective coagulation for twin-twin transfusion syndrome. Twin Res Hum Genet 2016; 19:217-21. https://doi.org/10.1017/thg.2016.25
PMid:27203607
40. Peyre SE, Ashley SW. Teaching uncommon and highly complex operations: maximizing the teaching and learning. J Gastrointest Surg 2011; 15:1724-5. https://doi.org/10.1007/s11605-011-1570-2
PMid:21630103
41. The Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Management of monochorionic twin pregnancy. C-Obs 42. 2014. Available at: https://www.ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27s%20...(C-Obs-42)-reviewJuly-2017.pdf?ext=.pdf. Accessed November 12, 2018.
43. Population Division, Department of Economic and Social Affairs, United Nations. World Population Prospects: The 2017 Revision. Methodology of the United Nations Population Estimates and Projections, Working Paper No. ESA/P/WP.250. New York, NY: United Nations, 2017. Available at: https://population.un.org/wpp/Publications/Files/WPP2017_Methodology.pdf. Accessed December 16, 2018.
44. El-Sabawi B, Magee W 3rd. The evolution of surgical telementoring: current applications and future directions. Ann Transl Med 2016; 4:391. https://doi.org/10.21037/atm.2016.10.04
PMid:27867943 PMCid:PMC5107399
46. Bruns NE, Irtan S, Rothenberg SS, et al. Trans-atlantic telementoring with pediatric surgeons: technical considerations and lessons learned. J Laparoendosc Adv Surg Tech A 2016; 26:75-8. https://doi.org/10.1089/lap.2015.0131
PMid:26698191
47. Gilbert JH, Yan J, Hoffman SJ. A WHO report: framework for action on interprofessional education and collaborative practice. J Allied Health 2010; 39 Suppl 1:196-7.
48. Schmitt MH. Collaboration improves the quality of care: methodological challenges and evidence from US health care research. J Interprof Care 2001; 15:47-66. https://doi.org/10.1080/13561820020022873
PMid:11705070