

Abstract
INTRODUCTION
Emerging infectious disease outbreaks, such as the present coronavirus disease 2019 (COVID-19) pandemic, often have a psychological impact on the well-being of the general population, including survivors and caregivers. Our study aimed to synthesise extant literature regarding the combined psychological responses and coping methods used by the general population in past outbreaks.
METHODS
We conducted a narrative synthesis of the published literature over the last two decades with a quality appraisal of included articles that reported both psychological responses and coping strategies within infectious disease outbreaks.
RESULTS
A total of 144 papers were identified from the search, 24 of which were included in the review. Overall, 18 studies examined the psychosocial responses of the general population towards the severe acute respiratory syndrome epidemic, four studies focused on the Ebola epidemic and two studies covered the H1N1 outbreak. Common themes in psychological responses included anxiety/fears, depression, anger, guilt, grief and loss, post-traumatic stress and stigmatisation, but also a greater sense of empowerment and compassion towards others. Coping strategies adopted included problem-focused coping (seeking alternatives, self- and other-preservation), seeking social support, avoidance, and positive appraisal of the situation.
CONCLUSION
Amid the range of psychosocial responses seen in past infectious disease outbreaks, practical considerations for the current COVID-19 pandemic need to focus on the individual in the context of the larger social environment, with an emphasis on raising awareness of the range of possible psychosocial responses, access to psychological help, self-care, empowering self-support groups and sustained engagement with updated, reliable information about the outbreak.
INTRODUCTION
The infectious disease outbreaks of recent years have had a significant impact on not only the physical health but also the psychological well-being of communities.(1) The severe acute respiratory syndrome (SARS) outbreak in 2002/2003, H1N1 influenza pandemic in 2009, Middle East respiratory syndrome (MERS) outbreak in 2012 and the current coronavirus disease 2019 (COVID-19) pandemic are all notable infectious disease outbreaks affecting multiple countries and communities.(2) As of 26 March 2020, COVID-19 has affected more than 492,000 people across 198 countries and territories; more than 22,000 people have died from the disease and over 119,000 have recovered at the time of writing.(3) Of note, the general population, including caregivers who are not infected by the disease, is not spared from the psychological consequences of such outbreaks.(4-7) This can be related to various factors including a disruption of the usual routine of life,(8) grief and loss,(9) and stigmatisation experienced during such outbreaks.(10,11) These psychological responses affect the well-being of the individual and community, and can persist long after the outbreak.(12) In the context of the present evolving COVID-19 pandemic, there is a need to synthesise the available information regarding the psychological effects and coping strategies employed during past infectious disease outbreaks in order to understand how we can better support the general public in dealing with this current pandemic.
There are several knowledge gaps to bear in mind. First, the psychosocial responses of patients, survivors, caregivers and the general population could differ from one group to another across outbreaks as the affected population may face unique concerns and experiences during each outbreak. Factors influencing these varying responses also require clarification, as variations in systems of support may be required. Second, it is important to examine different coping responses (adaptive and maladaptive) that have been adopted by the general population, which can have a bearing on overall psychological health.
In light of these knowledge gaps, our study aimed to conduct a narrative synthesis of extant data that documents both the psychological impact and coping responses in the general population (including patients, survivors and caregivers) across past infectious disease outbreaks. We then suggest practical considerations in the current COVID-19 pandemic and possible future research directions.
METHODS
We performed a systematic search of the available literature using PubMed, MEDLINE (Ovid), and Web of Science. The following search strategy was used ((psychiatric OR psychological) AND coping) AND (H5N1 OR Nipah OR Ebola OR SARS OR ‘severe acute respiratory syndrome’ OR H1N1 OR MERS OR ‘Middle East respiratory syndrome’ OR H7N9), with papers over the past two decades being considered for inclusion. Only studies in the English language and papers from peer-reviewed journals were included. Editorials, commentaries, perspectives, case studies, reviews and dissertations were excluded. Studies that explored coping or psychosocial responses in isolation without relating the two concepts were excluded.
We assessed the quality of articles included in our review using critical appraisal tools for quantitative(13) and qualitative(14) studies. The use and modification of such tools can be seen in previous studies on infectious disease outbreaks.(4) We adapted these tools to the needs of our review by inserting the term ‘survivors/patients/caregivers/general population affected by an infectious disease outbreak’ and removing the ‘intervention’ component under McMaster quantitative guidelines.(13) The McMaster University critical appraisal tool(13) was used to appraise quantitative studies, with a score of 1 or 0 given to each of the 11 components. The guidelines by Higginbotham et al(14) were used to appraise the qualitative studies, with a score of 1 or 0 given to each of the ten components.
RESULTS
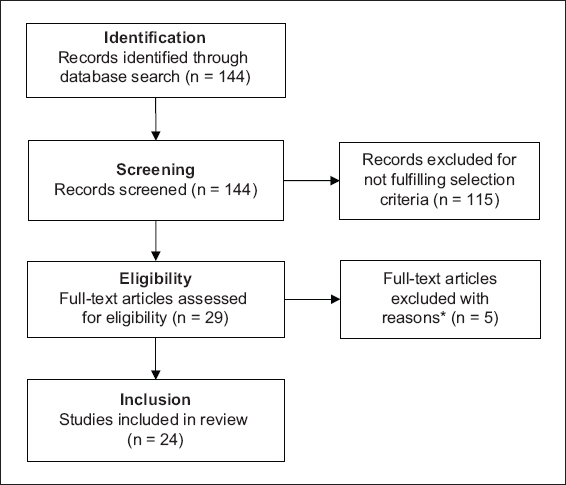
We identified 95 (PubMed) and 49 papers (Web of Science) from the database search, of which 24 papers (21 from PubMed, 3 from Web of Science) were included in the review. A PRISMA flow diagram depicting how articles were selected is presented in
Fig. 1
PRISMA flowchart shows the literature search and study selection process for psychological and coping responses towards emerging infectious disease outbreaks in patients and the general public. *Five articles looked at psychological responses or coping strategies in isolation. PRISMA: preferred reporting items for systematic reviews and meta-analyses
Quality appraisal
Of the 14 quantitative studies evaluated (12 employing only quantitative surveys and two mixed methods), all studies scored at least ten out of a maximum possible of 12 (Appendix, Supplementary Table II). Several studies failed to adequately report dropouts, exclusions or response rates.(7,15-18) Of the 12 qualitative studies evaluated (ten qualitative interviews and two mixed methods), all studies scored at least nine out of a maximum possible of ten (Appendix, Supplementary Table III). Although most of the studies mentioned how data was recorded and kept, aspects relating to data management and storage (e.g. whether data was destroyed after the study ended) were inadequately reported in some studies.
Common themes across infectious disease outbreaks
Psychological responses
Anxiety and somatic symptoms
The presence of anxiety and/or fears was a common theme, with rates varying between 3.2% and 12.6% across 11 out of 18 SARS-related studies,(6,8,19-27) both H1N1-related studies,(7,28) and two out of four Ebola-related studies.(29,30)
Anxiety levels of survivors were significantly higher than those of the general community, with 7.3% of the SARS survivors in Cheng et al’s study(20) reporting Beck Anxiety Inventory scores in the severe range. Almost 60% of the nationwide Taiwanese sample were worried about the recurrence of SARS, and 3.2% of them met the criteria for psychological distress based on Brief Symptom Rating Scale scores.(25) Higher rates were reported from a general community sample in Hong Kong, with 12.6% of them feeling ‘quite’ or ‘very’ anxious based on the State-Trait Anxiety Inventory scores.(23)
Somatic symptoms were reported in three out of 18 SARS-related studies,(20,25,31) and in one of the four Ebola-related studies.(11) SARS survivors had higher levels of somatic symptoms compared to community subjects.(20) Clinically significant levels of sleep disturbance were reported in 4.2% of a nationwide Taiwanese sample.(25) For residents living at the epicentre of the SARS outbreak, about 34% of those experiencing psychosomatic responses reported insomnia as well.(31)
Apart from the fear of another outbreak,(25) other reasons cited for increased anxiety included beliefs that one was more vulnerable to the infection,(26) uncertainty regarding the treatment process and outcomes,(8,24) the well-being of loved ones and their economic situation,(30) separation from loved ones, disruption in work life, and having to juggle multiple responsibilities as a caregiver.(8) In contrast, Joffe and Haarhoff(29) reported that although almost half of the general population sample in Britain recognised that the Ebola outbreak was a fearful disease, very few people expressed personal anxiety over the outbreak.
Depressive symptoms
Depressive symptoms with rates ranging from 3.0% to 73.1% were specifically observed in six out of 18 studies pertaining to SARS(15,21,24,25,27,31) and two studies on the Ebola epidemic.(11,30) The presence of helplessness or hopelessness, which are cognitive features of depression, were also seen in three SARS-related studies(18,21,24) and both Ebola-related studies.(11,30) In a nationwide Taiwanese sample, 3.0% met the criteria for psychological distress due to depression,(25) and 73.1% of Hong Kong residents staying at the epicentre of the outbreak reported more than two weeks of low mood following the outbreak.(31)
Reasons associated with depressive symptoms include an inability to return to their usual routine of life,(30) the contagiousness of the disease, lack of information regarding its route of transmission, stigma, and proximity to the epicentre of the outbreak.(31) In particular, the extreme role change experienced by healthcare workers who later became patients after contracting SARS was associated with a sense of helplessness.(24) Survivors of Ebola and their family members also viewed the disease and subsequent death as inescapable, which conveyed a sense of hopelessness.(11)
Feelings of anger and irritability with rates ranging from 2.3% to 56.7% were reported in five SARS-related studies.(22,24,25,27,31) Of note, 2.3% and 2.9% of a nationwide Taiwanese sample had clinically significant levels of hostility and inferiority respectively.(25) Younger and middle-aged adults appeared to experience higher levels of anger as compared to older adults.(27) Anger and frustration was attributed to lack of and conflicting information regarding the disease,(22,31) as well as feelings of isolation and stigmatisation that persisted even after discharge.(24,31)
Grief and loss experienced at multiple levels featured more prominently in studies of Ebola and were reported in two studies.(9,30) This was a result of not only the death of loved ones(9,30) but also a loss of one’s cultural identity, rituals(9) and material possessions.(30) Loss as experienced by those affected during the SARS and H1N1 outbreaks was often related to a loss of one’s usual way of life. In a sample of residents living at the epicentre of the SARS outbreak in Hong Kong, 88.1% felt that the outbreak had severely affected their daily life.(31) Healthcare workers who later became infected felt the loss in the occupational sphere of life as they transitioned from the role of a healthcare provider to that of a patient.(24) Patients also reported experiencing a loss of control due to the lack of information available regarding the disease and treatment process.(24)
In terms of longitudinal changes, negative cognitions and emotional responses tended to decline over time.(18) In particular, older adults experienced a greater decline in sadness about two months after the outbreak as compared to younger adults.(27) The nature of concerns reported by respondents also changed over time. Possible factors included one’s geographical distance from the outbreak(18) and use of coping strategies.(27) Situation-specific coping strategies (personal hygiene practices and avoidance of crowds) were more predictive of changes in anxiety levels as compared to lifestyle habits or information-seeking behaviour.(19)
Post-traumatic stress symptoms
Post-traumatic stress symptoms (25.8%) were reported in one SARS-related(6) and two Ebola-related studies.(11,30) Survivors of Ebola and their caregivers reported lingering feelings of fear and low mood after the outbreak and re-experienced them during subsequent disease outbreaks.(11) Many Ebola survivors also reported flashbacks, particularly those involving images of corpses.(30) In a sample of the general population in Singapore, 25.8% of the respondents experienced post-traumatic morbidity following a SARS outbreak as well.(6)
Stigmatisation, abandonment and isolation
Experiences of stigmatisation, abandonment and isolation (rates of 9.7%–48.7%) were noted in seven SARS-related studies,(22,24-26,31,32) one H1N1-related study(28) and all four Ebola-related studies.
In a general population sample of Taiwanese residents, 9.7% reported that they, their family or their friends had experienced SARS-related discrimination because they had been quarantined or had family members who were healthcare workers.(25) Residents living at the epicentre of the outbreak in Hong Kong experienced more severe stigmatisation, with 40.6% being rejected for dining with friends, 48.7% experiencing workplace discrimination from employers, and 47.8% from colleagues.(31)
Stigmatisation resulted not only from one’s identity as a survivor or relationship to a survivor,(11,25,30,33) but also one’s nationality,(28,29) place of residency(31) and health status prior to the outbreak.(26) Those having chronic illnesses prior to the outbreak were identified as being particularly vulnerable to SARS, resulting in discriminatory attitudes towards them.(26) Latinos were stigmatised as Mexico was determined to be the epicentre of the H1N1 outbreak.(28) Attitudes of the general population were particularly influenced by media portrayals.(26,29)
Feelings of abandonment and isolation often result from experiences of stigma and discrimination. Survivors reported feeling abandoned when they were turned away from healthcare services,(9) ostracised by their community(9,30) and distanced from healthcare workers due to the use of personal protective equipment (PPE).(9,22)
Feelings of isolation often arose as a result of having to be quarantined.(30) Despite most patients understanding the need for quarantine measures, being quarantined evoked feelings of abandonment that sometimes lasted beyond discharge.(24) These quarantine measures also affected those who were not exposed to the virus, such as new mothers who had to be separated from their infant.(22) Immigrants were particularly worried about how quarantine measures would affect their community and result in further isolation.(28)
Positive changes and cognitive restructuring
Positive changes and post-traumatic growth as a result of the outbreak were seen in four SARS-related studies(21,24,32,33) and one Ebola-related study.(30) Some survivors gained self-empowerment through the ordeal, transcending victimhood.(11,33) This took the form of having increased compassion, being present for others despite the fear, showing empathy even to those who discriminated against them,(33) and educating others about the outbreak.(30) Survivors also reported a change in perspective on life and their occupational roles. Some began to redefine their life priorities,(24) while healthcare workers who fell ill began to understand the importance of providing psychological support during times of crisis.(24,33)
Coping responses
Problem-solving
Alternatives were sought when healthcare services were not accessible or limited. Some respondents sought complementary medicine when healthcare services were not accessible or when they were refused treatment.(9) Others sought alternative measures such as qigong, recognising the limitations of biomedical treatment.(26) This coping strategy allowed them to take active steps towards self-empowerment and reduced feelings of uncertainty by providing a sense of control over their health.(26)
Respondents engaged in behaviours they believed would serve to protect themselves or others. This took the form of infection control measures(19,28) such as cleaning their homes with hygiene supplies(11,22) and changing their healthcare decision-making process.(22) Some even took care of family members, acquaintances or strangers who were infected by the disease.(9) Other measures that were adopted included increased monitoring of information pertaining to the outbreak(19,22) and self-isolation. Some chose to self-isolate when they suspected that they had contracted the disease in order to prevent its spread.(9) Others isolated themselves from healthcare workers in an act of self-preservation(9,17,19,33) or to avoid placing more burden on others during this stressful period.(8) To avoid discrimination and stigma, respondents hid their status as a survivor or their place of residency when seeking employment, and some even chose to relocate.(31)
Seeking social support
One of the common strategies adopted by respondents was seeking social support.(15,16,20,24,27,32) Such communities of support were formed when respondents sought alternative treatment(26) and when fellow patients and survivors came together for mutual support.(30,31) The presence of supportive healthcare workers was comforting to patients and survivors.(24,30) Many also found prayer and support from the religious community to be helpful.(9,11,24,28,30)
Distraction, denial or avoidance
Some respondents found ways to distract themselves from the situation by performing external actions, while some others resorted to mental avoidance.(6,8,9,15,17,24,27,28,30,32) Some Ebola patients ran away from their town,(9) while others kept themselves busy looking for jobs or reading.(30) Caregivers distracted themselves by going out to buy the patients’ favourite food.(8) Some survivors mentally disengaged from the traumatising situation in the treatment unit and experienced a sense of numbness,(30) while members of the general public denied the significance of the pandemic after being overwhelmed by information(28) or expressed wishful thinking.(17) Nurses who were eventually diagnosed with SARS tended to reject the possibility of the diagnosis even when they started feeling unwell.(24)
Positive appraisals
Respondents tried adopting a positive attitude in the face of the crisis.(6,11,15,27,32) For example, some chose to seek alternative treatment and prevention methods,(26) which reflected an internal locus of control.(7,26) The confidence that respondents placed in their government’s ability to manage the situation(25) or their healthcare system(23,29) also reflected a positive appraisal of the situation. Some attempted to reappraise the situation through a culturally relevant lens, using stories from past outbreaks in their cultural community to understand what to anticipate and reduce distress.(28)
Correlations between variables
Demographic factors, perception of risk and psychological distress
Demographic factors were correlated with psychiatric distress as well. Survivors who were healthcare workers,(20,21) had a chronic illness(26) or had lost family members were significantly more likely to experience high distress.(30) Older adults were more likely to experience psychological distress, according to a study by Peng et al,(25) although Main et al(15) found a negative correlation between age and disease-related stressors. Those with a higher level of education had better mental health (p < 0.01)(16) and less negative emotions (p < 0.05).(18)
Perception of risk was positively correlated with psychological symptoms (r = 0.12, p ≤ 0.01).(15) Specifically, the fear of a recurrent outbreak was predictive of psychological distress (odds ratio [OR] 1.48, 95% confidence interval [CI] 1.02 to 2.16),(25) as were concerns about losing control of the spread of SARS, contracting SARS and the health of one’s family.(6) On the other hand, post-traumatic morbidity was not associated with these concerns.(6) Appraisals of the perceived impact of the epidemic,(21) particularly the level of threat (r = 0.59, p < 0.01), self- and other-control regarding the virus(7) and one’s coping efficacy,(16,21) were predictive of anxiety,(7) depression,(21) and overall mental health and functioning.(16)
Perceived general health (r = −0.46, p ≤ 0.001) and life satisfaction (r = −0.31, p ≤ 0.001) were negatively correlated with psychological symptoms.(15)
Demographic factors, risk appraisal and coping strategies
Age was negatively correlated with active coping (r = −0.14, p ≤ 0.05) and seeking social support (r = −0.12, p ≤ 0.05).(15) A mediating factor may be the phase of the outbreak, as younger adults reported using more emotion-focused coping at the acute phase of the outbreak, while older adults used more emotion-focused coping several months after the outbreak.(27)
Appraisals of threat(17) and personal vulnerability predicted the adoption of active coping strategies(26) such as infection control measures (OR 1.50, 95% CI 1.07–2.09).(23) Appraisals of self- and other-control during the outbreak were negatively correlated with the use of emotion-focused strategies (p < 0.01 and p < 0.05, respectively) and positively correlated with the use of problem-focused strategies (both p < 0.01).(7) Respondents who perceived the negative effects of the outbreak to be more severe had lower levels of defensiveness or denial.(32) Active coping was positively related to perceived general health (r = 0.12, p ≤ 0.05) and life satisfaction (r = 0.17, p ≤ 0.001).(15) Seeking social support was positively correlated with life satisfaction (r = 0.11, p ≤ 0.05), while rumination and worry resulted in less problem-focused coping (r = −0.34, p < 0.001).(15)
DISCUSSION
Our study aimed to explore the psychosocial responses in survivors, caregivers and the general population during an infectious disease outbreak. We identified several common themes in psychological responses across the outbreaks, including anxiety/fears, depression, anger, guilt, grief and loss, post-traumatic stress, and stigmatisation but also positive changes and cognitive restructuring. Common coping strategies included problem-focused coping (seeking alternatives, self- and other-preservation), seeking social support, avoidance and positive appraisal of the situation.
Comparison across outbreaks
Psychological distress
Fears, anxieties and depression were common psychological symptoms reported across outbreaks. Underlying reasons cited for these symptoms included disruptions in daily routine, the uncertainty involving one’s job and financial security, their loved ones’ well-being, the treatment process, and information pertaining to the disease. Post-traumatic stress symptoms, on the other hand, differed more significantly across outbreaks. Studies exploring the impact of the Ebola epidemic, in particular, often featured post-traumatic stress symptoms as a main theme. This could possibly be explained by the higher mortality rate for the Ebola outbreak (50%) compared with SARS (15%)(34,35) and H1N1 (0.02%),(36) and the disparity in quality and accessibility of healthcare services in affected regions. Ebola-related studies in our review were concentrated in West Africa, where the quality and accessibility of healthcare services are often lacking as compared to developed nations where the SARS and H1N1 outbreaks occurred. This resulted in poor handling of bodies postmortem and a situation in which survivors had to spend an extended period of time in the same treatment unit as those who had already passed away.(9,30) This contributed to post-traumatic stress symptoms such as flashbacks involving images of corpses.(30) Issues with the healthcare system and implementation of infection control measures also meant that the mortality rate and likelihood of transmitting the virus within families and communities were higher for Ebola virus outbreaks. Hence, respondents were more likely to have experienced grief and loss from the death of a loved one.(9,11,30) Whereas the nature of loss as experienced by respondents involved in the Ebola outbreak were largely focused on the physical (i.e. people and possessions),(30) those affected in the SARS and H1N1 outbreaks often reported losses involving aspects of daily life, such as a disruption in their daily routine or social support.(22)
Despite the possible differences in culture, education levels and healthcare services available, stigma and abandonment were reported across various outbreaks. One plausible explanation for this is that the various communities lacked information or experience on these emerging infectious diseases at the start and ways to handle the situation. Large-scale infectious disease outbreaks of high severity were still uncommon to most countries. This resulted in issues regarding the dissemination of health information in an appropriate and accurate manner.(8,24,26,28,29) Media portrayals, in particular, appeared to have a strong influence on discriminatory attitudes directed towards selected groups of people, such as the chronically ill(26) and those of a certain nationality.(28,29)
Coping strategies
The use of different coping methods (e.g. problem-solving, seeking social support, distraction/denial/avoidance and positive thinking)(37) in reducing psychological distress differed across studies. Problem-solving reduced sadness in a study by Yeung and Fung,(27) but was unrelated to(7) or contributed to an increase in anxiety levels in other studies.(19) Conflicting results could be explained in relation to one’s appraisal of the situation. Lazarus and Folkman(38) suggested that a ‘goodness of fit’ had to be achieved between one’s appraisal of the situation and the selected coping strategy to maximise its effectiveness. The use of problem-focused strategies such as problem-solving should predict better adjustment in controllable situations, while emotion-focused strategies such as avoidance and denial would be favoured in uncontrollable situations.(38) Notably, attempts at problem-solving resulted in a decline in sadness only for the older adult group in Yeung and Fung’s(27) study. This could indicate that older adults who may have had more experience dealing with health issues and previous encounters with infectious disease outbreaks appraised the situation as being controllable, more so than the younger and middle-aged adults. Across studies, survivors found solace in religious practices, the presence of empathetic healthcare workers throughout their treatment and discharge, and the support of fellow survivors.(9,11,24,30) Attempts to cope through positive thinking and appraisals were reflected across studies, with the general population putting their confidence in alternative treatments, the government or the healthcare system.(23,25,29)
Practical considerations in the current COVID-19 pandemic
The current COVID-19 pandemic is unique in its high transmissibility; potential infectivity through mildly symptomatic individuals; severe complications in the elderly, those with medical comorbidities and even the younger population; and the absence of vaccine and proven biological therapies at the time of writing.(39) Yet, one must not lose track of the possible responses of affected individuals in the bid to contain the outbreak.(40) In view of the likely prolonged nature of the pandemic and range of psychosocial responses that can occur,(11) it is important to raise awareness among the general population and healthcare providers about its clinical manifestations.(10) Second, awareness of these psychosocial responses would allow early identification of individuals who may need further psychological assistance in the event that these responses are persistent, unusually intense, pervasive across different settings and impair daily functioning of the individual. This also highlights the need to maintain the continuity of mental health services, especially of those with pre-existing mental illness and who may be affected by the COVID-19 pandemic. Third, access to psychological help should be made available whenever needed, with sensitivity to specific arrangements in relation to the pandemic such as special work arrangements, quarantine orders, stay-home notice, leave of absence, medical leave and hospitalisation for COVID-19 treatment. Fourth, it is important to encourage adaptive coping responses(15) such as self-care,(16) which includes adequate rest, spending time with loved ones, recreational activities within official advisory limits or upskilling, which can be done online.(9) Fifth, it is useful to empower peer and community support groups to look out for one another during such times of anxiety, frustration, uncertainty, isolation and stigmatisation.(11,12,16) In view of the need to observe physical distancing, leveraging on technology and social media to facilitate responsive and real-time outreach for greater connectivity would be useful in overcoming social isolation. Encouraging such prosocial behaviours may promote more adaptive responses during a stressful period such as the current pandemic and prevent more automatic and unhelpful responses.(17) Sixth, there needs to be sustained engagement in terms of access to updated, verifiable information about the outbreak due to its likely enduring trajectory, the ubiquity of social media and subjective reporting, and evolving illness dynamics internationally.(41,42) Seventh, it is crucial to maintain a spirit of perseverance and optimism to weather the pandemic, which will pass like previous pandemics.
Implications for further research
Several areas are worth noting. First, it would be meaningful to examine the psychosocial responses of different subgroups in the population that have been affected by the outbreak across different occupations and seniority, and of those affected by control measures such as quarantine orders. This would allow us to have a more comprehensive understanding of its impact. Second, prospective studies are needed to assess changes in psychosocial responses over time and the relationship to demographic profiles, risk perception or exposure status to current pathogens in daily routines and work. Third, it would be useful to examine the impact and relationship of social media to various psychosocial responses, as these information-sharing platforms were not as prevalent during past infectious disease outbreaks. Fourth, understanding how experiences of previous outbreaks influence current psychosocial responses would allow targeted efforts to ameliorate these underlying factors.
In conclusion, this review aimed to synthesise the psychosocial responses (psychological responses and coping methods) in the general population, survivors and caregivers across previous infectious disease outbreaks. Psychological responses included anxiety, depression, loss, stigmatisation, isolation and cognitive restructuring. The extent to which each type of coping strategy was helpful for relieving psychological distress was associated with varied factors, including one’s risk appraisal, demographic factors and severity of the outbreak. Practical considerations for the current pandemic need to focus on the individual in the context of the larger social environment, with an emphasis on raising awareness of the range of possible psychosocial responses, access to psychological help, self care and sustained engagement. Further research endeavours should seek to understand the longitudinal psychological impact of disease outbreaks, differences in psychosocial responses among population subgroups, inter-relationships with social media, and the influence of past experiences with infectious disease outbreaks, in order to better prepare ourselves psychologically to face future outbreaks.