Singapore Med J 2017; 58(10): 580-584 doi: 10.11622/smedj.2017097
Outpatient management of knee osteoarthritis
Yiyang Liow1, MBBS, Wilson Wang2,3, MBBS, FRCS, Victor Weng Keong Loh1,2, MCFP, MHPE
Author Information >Copyright and License information >
1Division of Family Medicine, National University Health System, Singapore 2Yong Loo Lin School of Medicine, National University of Singapore, Singapore 3Department of Orthopaedic Surgery, National University Hospital, Singapore Correspondence: Dr Yiyang Liow, Resident, Family Medicine Residency Programme, Division of Family Medicine, National University Health System, 1E Kent Ridge Road, NUHS Tower Block, Level 9, Singapore 119228. yiyang_liow@nuhs.edu.sg
Osteoarthritis of the knee is a common disease that causes significant disability. Most patients can be managed conservatively in the outpatient setting. A small minority require surgery. The cornerstones of treatment are weight loss, exercise and analgesia. Walking aids, medial patellar taping, acupuncture and transcutaneous electrical nerve stimulation are useful management adjuncts. Current evidence does not support routine prescription of glucosamine and chondroitin supplements. Early consultation with an orthopaedic surgeon should be made when conservative measures fail.
Keywords: knee, osteoarthritis, treatment
Mdm Goh walked into your clinic with an antalgic gait. She complained of gradually worsening right medial knee pain for the past two years, which worsened with activity and got better with rest. Examination revealed a mild varus deformity, a small effusion and crepitus on passive range of motion. Over-the-counter paracetamol was initially effective for her, but no longer provided relief. Mdm Goh had seen advertisements in magazines promoting glucosamine joint supplements and wondered if they would help with her pain.
HOW RELEVANT IS THIS TO MY PRACTICE?
Osteoarthritis (OA) is a leading cause of disability worldwide. In 2015, the World Health Organization estimated that a total of 8,000 years had been lost to disability from OA in Singapore.(1) As a major weight-bearing joint, the knee is one of the most common sites affected. Besides the obvious direct costs, knee OA imposes substantial indirect and intangible costs on patients.(2) Recognising the increasing burden of disease in our ageing population, the Ministry of Health, Singapore, released clinical practice guidelines on the management of knee OA more than ten years ago.(3) Since then, new research and major international guidelines have emerged to guide physicians in managing this ubiquitous disease.
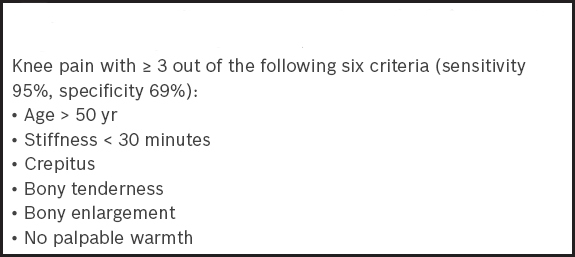
Knee OA can be diagnosed clinically. A history of gradually worsening mechanical knee pain and deformity is typical. Patients may reveal a previous traumatic knee injury, particularly meniscal tears. Pain that is worse on going down stairs is classically suggestive of patellofemoral involvement. Quadriceps wasting and mild effusion are common examination findings. Occasionally, a Baker’s cyst is palpable in the popliteal fossa. Morning stiffness lasting longer than 30 minutes with significant joint effusion and warmth should prompt consideration of an inflammatory joint disorder. Box 1 shows the criteria for diagnosis of knee OA from the American College of Rheumatology (ACR).
Box 1
American College of Rheumatology criteria for clinical diagnosis of idiopathic OA of the knee.(5)
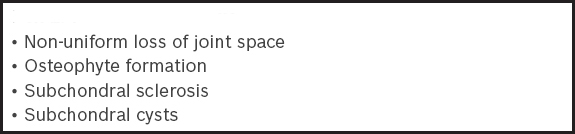
Plain radiography is not routine, but is a useful adjunct to confirm the diagnosis. Weight-bearing radiographs characteristically demonstrate a loss of joint space in conjunction with other classic changes. Skyline views are useful when suspecting patellofemoral OA. However, it is notable that knee pain can precede radiographic changes by years.(4) Box 2 shows the radiological signs of OA.
Laboratory testing is performed if there are concerns about inflammation or other causes of joint disease. Erythrocyte sedimentation rate and C-reactive protein are serum inflammatory markers that may be mildly raised, but significant elevation is not expected in knee OA. Rheumatoid factor and anti-cyclic citrullinated peptide are frequently used to screen for rheumatoid arthritis, while raised serum uric acid levels may be consistent with gouty arthritis.
WHAT CAN I DO IN MY PRACTICE?
Weight loss and exercise
For overweight patients, weight loss reduces the load imposed on the knees and has been shown to improve symptoms and function. This positive effect has been described following weight loss of more than 5% over a five-month period.(7) Combining caloric restriction with exercise appears to be the most effective strategy to achieve weight loss and symptomatic improvement.(8)
Exercise has also been shown to significantly reduce pain and improve quality of life.(9) Both the 2013 American Academy of Orthopedic Surgeons (AAOS) and the 2012 ACR recommendations on exercise for knee OA concur on this, strongly recommending muscle strengthening and low-impact aerobic exercises.(10,11) Additionally, the ACR also recommends aquatic exercises.(11) Exercises commonly suggested to patients include brisk walking, swimming, cycling and tai-chi. Ideally, the activity should be one that patients will continue to enjoy doing after the treatment period is over.
Instructional handouts are available on the Internet to guide patients in performing lower limb muscle-strengthening exercises on their own.(12) Referral to a physiotherapist should be considered for those who are deconditioned and require a personalised and structured exercise programme. Due to fear of pain or progression of disease, some patients may limit or stop exercise altogether. As this can lead to a vicious cycle of inactivity, muscle weakness, weight gain, more pain and functional impairment, it is critical to identify and address these concerns early on.
Analgesia
Pain control is the cornerstone of pharmacological treatment of knee OA. The 2012 ACR guidelines for the management of OA conditionally recommend the use of paracetamol, oral or topical nonsteroidal anti-inflammatory drugs (NSAIDs) and tramadol for pharmacological management of knee OA.(11)
When prescribing the full dosage of paracetamol of 4,000 mg per day (i.e. eight 500-mg tablets), physicians should advise patients to avoid other paracetamol-containing products such as over-the-counter cold remedies. However, NSAIDs should be avoided in patients with significant gastrointestinal bleeding, renal impairment or cardiovascular disease. Proton-pump inhibitors should be prescribed for their gastroprotective effects when NSAIDs are used for chronic pain management for knee OA.(13,14) If pain control is still not achieved, tramadol is added.
Glucosamine and chondroitin
Glucosamine and chondroitin are commercially available oral supplements that have long been marketed as providing joint cartilage support, with the purported benefits of pain relief and slowing disease progression. Both products, alone or in combination, have been extensively studied, but there has been no convincing evidence of benefit to date.(15-18) Neither the AAOS nor ACR guidelines support their routine use in the treatment of knee OA.(10,11)
Despite the lack of evidence, these supplements are still commonly prescribed by physicians, probably owing to their reputation for being ‘harmless’. Although major adverse events are rare, gastrointestinal effects such as heartburn and dyspepsia are common. If prescribed, they should be taken with meals to minimise such symptoms.
Intra-articular injections
Often described as a simple process of wear and tear, OA actually has a complex disease mechanism driven by inflammatory mediators within the affected joint.(19) Intra-articular corticosteroid injections have traditionally been used to reduce local inflammation in the hope of improving pain and function. Current evidence suggests that intra-articular corticosteroid injections may provide short-term reduction in pain for up to six weeks.(20,21) The ACR guidelines support their conditional use, but the AAOS workgroup interpreted the evidence to be inconclusive and was unable to make a recommendation for or against their use.(10,11)
Hyaluronic acid is a naturally occurring component of joint cartilage matrix and synovial fluid. It lubricates joint movements and acts as a shock absorber. Intra-articular injections of hyaluronic acid are thought to restore such viscoelastic properties. Published meta-analyses have generally shown positive results, but controversy regarding its efficacy remains.(22-25) There are also additional concerns about cost-effectiveness, and studies evaluating its efficacy reflect a high percentage of industry authorship.(26) The AAOS does not recommend the use of hyaluronic acid injections in knee OA treatment, while the ACR guidelines make no recommendations.(10,11)
Orthoses and patellar taping
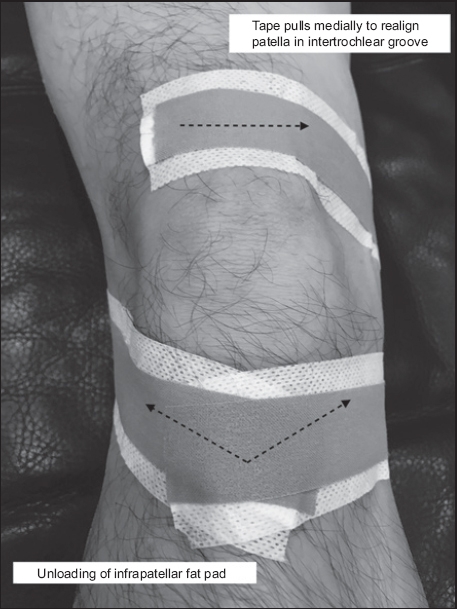
Lateral wedge insoles and valgus-directed braces have been prescribed for patients with medial compartment knee OA. However, the evidence generally does not support their use.(27-29) Conversely, medial patellar taping has been shown to be useful for patients with patellofemoral OA.(30-33) This simple intervention exerts a medially directed force to realign the patella in the intertrochlear groove, thereby reducing pain. During application, the patient should be lying down with the knee extended and thigh muscles relaxed. Tape is applied to the superior aspect of the patella, pulled medially and fixed to the medial side of the knee. Additionally, a second and third tape is applied to the tibial tubercle and pulled to the medial and lateral joint lines, respectively (Fig. 1). This unloads the infrapatellar fat pad, which can be aggravated by stretching of tissue.(34) A commercially available adhesive, non-stretch sports tape is typically used. A hypoallergenic underlay tape can be applied in combination.
Fig. 1
Photograph shows the application of medial patellar taping on the right knee.
Taping can be performed regularly by a physiotherapist, but self-taping is recommended, as it empowers patients to care for their own knees.
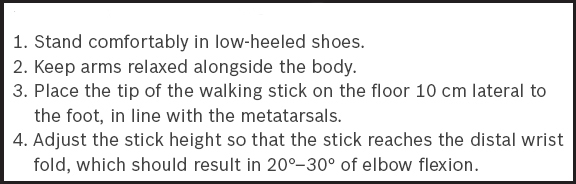
Walking aids
Walking aids decrease the load transmitted through the knees and thereby reduce pain and improve function.(35) Patients with unilateral or asymmetrical OA should use a walking stick on the contralateral side. The tip of the stick should be placed on the ground at the same time that the foot of the symptomatic knee lands on the ground.(36) The stick should also be appropriately customised for the patient. Those with bilateral or more symmetrical disease can consider the use of a walking frame. Box 3 shows the steps to take when customising a walking stick.
Acupuncture and transcutaneous electrical nerve stimulation
Traditional Chinese acupuncture has long been used as an alternative therapy in the treatment of knee OA. A recent meta-analysis of ten randomised controlled trials published through March 2015 investigated the effect of acupuncture on chronic knee pain. It concluded that acupuncture improves short- and long-term function, but provides only short-term pain relief.(37) Transcutaneous electrical nerve stimulation (TENS) involves transcutaneously applied electric currents to modulate nociceptive receptors and reduce pain. Studies have largely suggested that it can be a useful adjunct to reduce pain in knee OA patients.(38-40)
The ACR guidelines conditionally recommend both treatment modalities for patients who have at least moderate knee OA but are unable or unwilling to undergo total knee replacement.(11) Conversely, the AAOS does not recommend acupuncture, based on a lack of efficacy in the studies it analysed, and was inconclusive on electrotherapeutic modalities.(10)
Referral for surgery
Early consultation with an orthopaedic surgeon should be undertaken when adequate conservative treatment has failed to provide the patient satisfactory pain relief, stability or functional improvement.
TAKE HOME MESSAGES
Knee OA is a major cause of disability worldwide.
The burden of disease is expected to increase locally as our population ages.
A clinical diagnosis is sufficient to identify knee OA, but plain radiography and laboratory tests are useful adjuncts.
Weight loss of more than 5% over a five-month period can improve pain and function for overweight patients.
Low-impact aerobic exercises have significant benefits and should be encouraged.
Referral to a physiotherapist is indicated for deconditioned patients or those who will benefit from a structured exercise programme.
Adequate analgesia is paramount to prevent a vicious cycle of pain, activity limitation and weakness or weight gain. Paracetamol, NSAIDs and tramadol are recommended agents.
Beneficial management adjuncts include walking aids, medial patellar taping, acupuncture and TENS.
Interventions for knee OA that do not show clear evidence of benefit are glucosamine, chondroitin, intra-articular hyaluronic injections, lateral sole wedges and valgus-directed braces.
Early consultation with an orthopaedic surgeon is warranted when an adequate trial of conservative management has failed.
Mdm Goh returned to your clinic in six weeks and was happy to report improvements in pain control. She had lost 1.5 kg by modifying her diet and taking 30-minute brisk walks every morning. After mulling over your advice during the last consultation, she had decided not to take glucosamine supplements. Naproxen gave adequate relief when the pain arose and had not caused any gastric troubles. You applauded her efforts and reiterated the far-reaching benefits of her lifestyle changes.
References World Health OrganizationGlobal Health Estimates 2015:Burden of disease by Cause, Age, Sex, by Country and by Region. 2000-2015;. Available at: http://www.who.int/healthinfo/global_burden_disease/estimates/en/index2.html. Accessed September 14 2017. Xie F, Thumboo J, Fong KY, et al. A study on indirect and intangible costs for patients with knee osteoarthritis in Singapore.Value Health. 2008;11:Suppl 1S84-90. Ministry of Health SingaporeClinical Practice Guidelines:Osteoarthritis of the Knees. 2007;May. Available at: https://www.moh.gov.sg/content/dam/moh_web/HPP/Doctors/cpg_medical/current/2007/CPG_OA%20Kness_Booklet.pdf. Accessed September 14 2017. Thorstensson CA, Andersson ML, Jönsson H, Saxne T, Petersson IF.Natural course of knee osteoarthritis in middle-aged subjects with knee pain:12-year follow-up using clinical and radiographic criteria.Ann Rheum Dis. 2009;68:1890-3. Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association.Arthritis Rheum. 1986;29:1039-49. Swagerty DL, JrHellinger D.Radiographic assessment of osteoarthritis.Am Fam Physician. 2001;64:279-86. Christensen R, Bartels EM, Astrup A, Bliddal H.Effect of weight reduction in obese patients diagnosed with knee osteoarthritis:a systematic review and meta-analysis.Ann Rheum Dis. 2007;66:433-9. Messier SP, Mihalko SL, Legault C, et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis:the IDEA randomized clinical trial.JAMA. 2013;310:1263-73. Fransen M, McConnell S, Harmer AR, et al. Exercise for osteoarthritis of the knee:a Cochrane systematic review.Br J Sports Med. 2015;49:1554-7. Jevsevar DS.Treatment of osteoarthritis of the knee:evidence-based guideline, 2nd edition.J Am Acad Orthop Surg. 2013;21:571-6. Hochberg MC, Altman RD, April KT, et al. American College of RheumatologyAmerican College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee.Arthritis Care Res (Hoboken). 2012;64:465-74. Tan Tock Seng HospitalProtect Your Joints with these Strengthening Workouts. Available at: https://www.ttsh.com.sg/articles/protect-your-joints/. Accessed September 14 2017. Scheiman JM.The use of proton pump inhibitors in treating and preventing NSAID-induced mucosal damage.Arthritis Res Ther. 2013;15:Suppl 3S5. Latimer N, Lord J, Grant RL, et al. National Institute for Health and Clinical Excellence Osteoarthritis Guideline Development GroupCost effectiveness of COX 2 selective inhibitors and traditional NSAIDs alone or in combination with a proton pump inhibitor for people with osteoarthritis.BMJ. 2009;339:b2538. Wandel S, Jüni P, Tendal B, et al. Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee:network meta-analysis.BMJ. 2010;341:c4675. Reichenbach S, Sterchi R, Scherer M, et al. Meta-analysis:chondroitin for osteoarthritis of the knee or hip.Ann Intern Med. 2007;146:580-90. Singh JA, Noorbaloochi S, MacDonald R, Maxwell LJ.Chondroitin for osteoarthritis.Cochrane Database Syst Rev. 2015;1:CD005614. Vasiliadis HS, Tsikopoulos K.Glucosamine and chondroitin for the treatment of osteoarthritis.World J Orthop. 2017;8:1-11. Ayhan E, Kesmezacar H, Akgun I.Intraarticular injections (corticosteroid, hyaluronic acid, platelet rich plasma) for the knee osteoarthritis.World J Orthop. 2014;5:351-61. Bellamy N, Campbell J, Robinson V, et al. Intraarticular corticosteroid for treatment of osteoarthritis of the knee.Cochrane Database Syst Rev. 2006;2CD005328. Jüni P, Hari R, Rutjes AW, et al. Intra-articular corticosteroid for knee osteoarthritis.Cochrane Database Syst Rev. 2015;10CD005328. Lo GH, LaValley M, McAlindon T, Felson DT.Intra-articular hyaluronic acid in treatment of knee osteoarthritis:a meta-analysis.JAMA. 2003;290:3115-21. Bellamy N, Campbell J, Robinson V, et al. Viscosupplementation for the treatment of osteoarthritis of the knee.Cochrane Database Syst Rev. 2006;2CD005321. Campbell KA, Erickson BJ, Saltzman BM, et al. Is local viscosupplementation injection clinically superior to other therapies in the treatment of osteoarthritis of the knee:a systematic review of overlapping meta-analyses.Arthroscopy. 2015;31:2036-45.e14. Arrich J, Piribauer F, Mad P, et al. Intra-articular hyaluronic acid for the treatment of osteoarthritis of the knee:systematic review and meta-analysis.CMAJ. 2005;172:1039-43. Printz JO, Lee JJ, Knesek M, Urquhart AG.Conflict of interest in the assessment of hyaluronic acid injections for osteoarthritis of the knee:an updated systematic review.J Arthroplasty. 2013;28:30-33.e1. Duivenvoorden T, Brouwer RW, van Raaij TM.Braces and orthoses for treating osteoarthritis of the knee.Cochrane Database Syst Rev. 2015;3CD004020. Parkes MJ, Maricar N, Lunt M, et al. Lateral wedge insoles as a conservative treatment for pain in patients with medial knee osteoarthritis:a meta-analysis.JAMA. 2013;310:722-30. Bennell KL, Bowels KA, Payne C, et al. Lateral wedge insoles for medial knee osteoarthritis:12 month randomised controlled trial.BMJ. 2011;342:d2912. Hinman RS, Crossley KM, McConnell J, Bennell KL.Efficacy of knee tape in the management of osteoarthritis of the knee:blinded randomised controlled trial.BMJ. 2003;327:135. Cushnaghan J, McCarthy C, Dieppe P.Taping the patella medially:a new treatment for osteoarthritis of the knee joint?.BMJ. 1994;308:753-5. Warden SJ, Hinman RS, Watson MA, Jret al. Patellar taping and bracing for the treatment of chronic knee pain:a systematic review and meta-analysis.Arthritis Rheum. 2008;59:73-83. Crossley KM, Marino GP, Macilquham MD, Schache AG, Hinman RS.Can patellar tape reduce the patellar malalignment and pain associated with patellofemoral osteoarthritis?.Arthritis Rheum. 2009;61:1719-25. Handbook of Non Drug Intervention (HANDI) Project TeamTaping for knee osteoarthritis.Aust Fam Physician. 2013;42:725-6. Jones A, Silva PG, Silva AC, et al. Impact of cane use on pain, function, general health and energy expenditure dang gait in patients with knee osteoarthritis:a randomised controlled trial.Ann Rheum Dis. 2012;71:172-9. HANDI Project teamAccessed September 14 2017Walking cane knee osteoarthritishttp://www.racgp.org.au/download/Documents/HANDI/walking-cane-knee-osteoarthritis.pdf. Accessed September 14 2017. Lin X, Huang K, Zhu G, et al. The effects of acupuncture on chronic knee pain due to osteoarthritis:a meta-analysis.J Bone Joint Surg Am. 2016;98:1578-85. Osiri M, Welch V, Brosseau L, et al. Transcutaneous electrical nerve stimulation for knee osteoarthritis.Cochrane Database Syst Rev. 2000;4CD002823. Cherian JJ, Harrison PE, Benjamin SA, et al. Do the effects of transcutaneous electrical nerve stimulation on knee osteoarthritis pain and function last?.J Knee Surg. 2016;29:497-501. Chen LX, Zhou ZR, et al. Transcutaneous electrical nerve stimulation in patients with knee osteoarthritis:evidence from randomized-controlled trials.Clin J Pain. 2016;32:146-54.
2. Xie F, Thumboo J, Fong KY, et al. A study on indirect and intangible costs for patients with knee osteoarthritis in Singapore. Value Health 2008; 11 Suppl 1:S84-90. https://doi.org/10.1111/j.1524-4733.2008.00371.x
PMid:18387072
4. Thorstensson CA, Andersson ML, Jönsson H, Saxne T, Petersson IF. Natural course of knee osteoarthritis in middle-aged subjects with knee pain: 12-year follow-up using clinical and radiographic criteria. Ann Rheum Dis 2009; 68:1890-3. https://doi.org/10.1136/ard.2008.095158
PMid:19054828
5. Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum 1986; 29:1039-49. https://doi.org/10.1002/art.1780290816
PMid:3741515
6. Swagerty DL Jr, Hellinger D. Radiographic assessment of osteoarthritis. Am Fam Physician 2001; 64:279-86.
PMid:11476273
7. Christensen R, Bartels EM, Astrup A, Bliddal H. Effect of weight reduction in obese patients diagnosed with knee osteoarthritis: a systematic review and meta-analysis. Ann Rheum Dis 2007; 66:433-9. https://doi.org/10.1136/ard.2006.065904
PMid:17204567 PMCid:PMC1856062
8. Messier SP, Mihalko SL, Legault C, et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: the IDEA randomized clinical trial. JAMA 2013; 310:1263-73. https://doi.org/10.1001/jama.2013.277669
PMid:24065013 PMCid:PMC4450354
9. Fransen M, McConnell S, Harmer AR, et al. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med 2015; 49:1554-7. https://doi.org/10.1136/bjsports-2015-095424
PMid:26405113
10. Jevsevar DS. Treatment of osteoarthritis of the knee: evidence-based guideline, 2nd edition. J Am Acad Orthop Surg 2013; 21:571-6.
11. Hochberg MC, Altman RD, April KT, et al; American College of Rheumatology. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken) 2012; 64:465-74. https://doi.org/10.1002/acr.21596
13. Scheiman JM. The use of proton pump inhibitors in treating and preventing NSAID-induced mucosal damage. Arthritis Res Ther 2013; 15(Suppl 3):S5. https://doi.org/10.1186/ar4177
PMid:24267413 PMCid:PMC3891010
14. Latimer N, Lord J, Grant RL, et al; National Institute for Health and Clinical Excellence Osteoarthritis Guideline Development Group. Cost effectiveness of COX 2 selective inhibitors and traditional NSAIDs alone or in combination with a proton pump inhibitor for people with osteoarthritis. BMJ 2009; 339:b2538. https://doi.org/10.1136/bmj.b2538
PMid:19602530 PMCid:PMC2714674
15. Wandel S, Jüni P, Tendal B, et al. Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: network meta-analysis. BMJ 2010; 341:c4675. https://doi.org/10.1136/bmj.c4675
PMid:20847017 PMCid:PMC2941572
18. Vasiliadis HS, Tsikopoulos K. Glucosamine and chondroitin for the treatment of osteoarthritis. World J Orthop 2017; 8:1-11. https://doi.org/10.5312/wjo.v8.i1.1
PMid:28144573 PMCid:PMC5241539
19. Ayhan E, Kesmezacar H, Akgun I. Intraarticular injections (corticosteroid, hyaluronic acid, platelet rich plasma) for the knee osteoarthritis. World J Orthop 2014; 5:351-61. https://doi.org/10.5312/wjo.v5.i3.351
PMid:25035839 PMCid:PMC4095029
20. Bellamy N, Campbell J, Robinson V, et al. Intraarticular corticosteroid for treatment of osteoarthritis of the knee. Cochrane Database Syst Rev 2006; (2):CD005328. https://doi.org/10.1002/14651858.CD005328.pub2
21. Jüni P, Hari R, Rutjes AW, et al. Intra-articular corticosteroid for knee osteoarthritis. Cochrane Database Syst Rev 2015; (10):CD005328. https://doi.org/10.1002/14651858.CD005328.pub3
22. Lo GH, LaValley M, McAlindon T, Felson DT. Intra-articular hyaluronic acid in treatment of knee osteoarthritis: a meta-analysis. JAMA 2003; 290:3115-21. https://doi.org/10.1001/jama.290.23.3115
PMid:14679274
23. Bellamy N, Campbell J, Robinson V, et al. Viscosupplementation for the treatment of osteoarthritis of the knee. Cochrane Database Syst Rev 2006; (2):CD005321. https://doi.org/10.1002/14651858.CD005321.pub2
24. Campbell KA, Erickson BJ, Saltzman BM, et al. Is local viscosupplementation injection clinically superior to other therapies in the treatment of osteoarthritis of the knee: a systematic review of overlapping meta-analyses. Arthroscopy 2015; 31:2036-45.e14. https://doi.org/10.1016/j.arthro.2015.03.030
PMid:25998016
25. Arrich J, Piribauer F, Mad P, et al. Intra-articular hyaluronic acid for the treatment of osteoarthritis of the knee: systematic review and meta-analysis. CMAJ 2005; 172:1039-43. https://doi.org/10.1503/cmaj.1041203
PMid:15824412 PMCid:PMC556045
26. Printz JO, Lee JJ, Knesek M, Urquhart AG. Conflict of interest in the assessment of hyaluronic acid injections for osteoarthritis of the knee: an updated systematic review. J Arthroplasty 2013; 28:30-33.e1. https://doi.org/10.1016/j.arth.2013.05.034
PMid:23890521
27. Duivenvoorden T, Brouwer RW, van Raaij TM. Braces and orthoses for treating osteoarthritis of the knee. Cochrane Database Syst Rev 2015; (3):CD004020. https://doi.org/10.1002/14651858.CD004020.pub3
28. Parkes MJ, Maricar N, Lunt M, et al. Lateral wedge insoles as a conservative treatment for pain in patients with medial knee osteoarthritis: a meta-analysis. JAMA 2013; 310:722-30. https://doi.org/10.1001/jama.2013.243229
PMid:23989797 PMCid:PMC4458141
29. Bennell KL, Bowels KA, Payne C, et al. Lateral wedge insoles for medial knee osteoarthritis: 12 month randomised controlled trial. BMJ 2011; 342:d2912. https://doi.org/10.1136/bmj.d2912
PMid:21593096 PMCid:PMC3100910
30. Hinman RS, Crossley KM, McConnell J, Bennell KL. Efficacy of knee tape in the management of osteoarthritis of the knee: blinded randomised controlled trial. BMJ 2003; 327:135. https://doi.org/10.1136/bmj.327.7407.135
PMid:12869456 PMCid:PMC165705
31. Cushnaghan J, McCarthy C, Dieppe P. Taping the patella medially: a new treatment for osteoarthritis of the knee joint? BMJ 1994; 308:753-5. https://doi.org/10.1136/bmj.308.6931.753
PMid:8142829 PMCid:PMC2539631
32. Warden SJ, Hinman RS, Watson MA Jr, et al. Patellar taping and bracing for the treatment of chronic knee pain: a systematic review and meta-analysis. Arthritis Rheum 2008; 59:73-83. https://doi.org/10.1002/art.23242
PMid:18163413
33. Crossley KM, Marino GP, Macilquham MD, Schache AG, Hinman RS. Can patellar tape reduce the patellar malalignment and pain associated with patellofemoral osteoarthritis? Arthritis Rheum 2009; 61:1719-25. https://doi.org/10.1002/art.24872
PMid:19950307
34. Handbook of Non Drug Intervention (HANDI) Project Team. Taping for knee osteoarthritis. Aust Fam Physician 2013; 42:725-6.
PMid:24130976
35. Jones A, Silva PG, Silva AC, et al. Impact of cane use on pain, function, general health and energy expenditure during gait in patients with knee osteoarthritis: a randomised controlled trial. Ann Rheum Dis 2012; 71:172-9. https://doi.org/10.1136/ard.2010.140178
PMid:22128081
37. Lin X, Huang K, Zhu G, et al. The effects of acupuncture on chronic knee pain due to osteoarthritis: a meta-analysis. J Bone Joint Surg Am 2016; 98:1578-85. https://doi.org/10.2106/JBJS.15.00620
PMid:27655986
38. Osiri M, Welch V, Brosseau L, et al. Transcutaneous electrical nerve stimulation for knee osteoarthritis. Cochrane Database Syst Rev 2000; (4):CD002823. https://doi.org/10.1002/14651858.CD002823
39. Cherian JJ, Harrison PE, Benjamin SA, et al. Do the effects of transcutaneous electrical nerve stimulation on knee osteoarthritis pain and function last? J Knee Surg 2016; 29:497-501. https://doi.org/10.1055/s-0035-1566735
PMid:26540652
40. Chen LX, Zhou ZR et al. Transcutaneous electrical nerve stimulation in patients with knee osteoarthritis: evidence from randomized-controlled trials. Clin J Pain 2016; 32:146-54. https://doi.org/10.1097/AJP.0000000000000233
PMid:25803757