Singapore Med J 2021; 62(9): 454-457 doi: 10.11622/smedj.2021146
Paediatric traumatic brain injury: an approach in primary care
Haresh Singaraju1, MBBS, Adriel Zhijie Leong2, MRCS, MPH, Yang Chern Lim3, MRCPCH, FAMS, Vincent Nga2, MRCSE, FRCSE, Lee Gan Goh1, MMed, FCFP
Author Information >Copyright and License information >
1Division of Family Medicine, National University Hospital, Singapore 2Division of Neurosurgery, Department of Surgery, National University Hospital, Singapore 3Division of Children’s Emergency, Department of Paediatric Medicine, National University Hospital, Singapore Correspondence: Dr Haresh Singaraju, Chief Resident, Division of Family Medicine, National University Hospital, National University Health System, 1E Kent Ridge Road, Level 9, Singapore 119228. haresh_singaraju@nuhs.edu.sg
Sam, a nine-month-old infant with no significant past medical history, was brought into your clinic by his mother. She had heard a loud thud in the room and found Sam lying prone on the floor and crying. He had likely rolled off the bed, which was 0.7-m high. She attended to him immediately and brought him to your clinic. She appeared extremely worried. No loss of consciousness or seizure-like activity was noted.
WHAT IS TRAUMATIC BRAIN INJURY?
Traumatic brain injury (TBI) is defined as a disruption in the normal function of the brain that can be caused by a bump, blow, jolt to the head or penetrating head injury.(1)
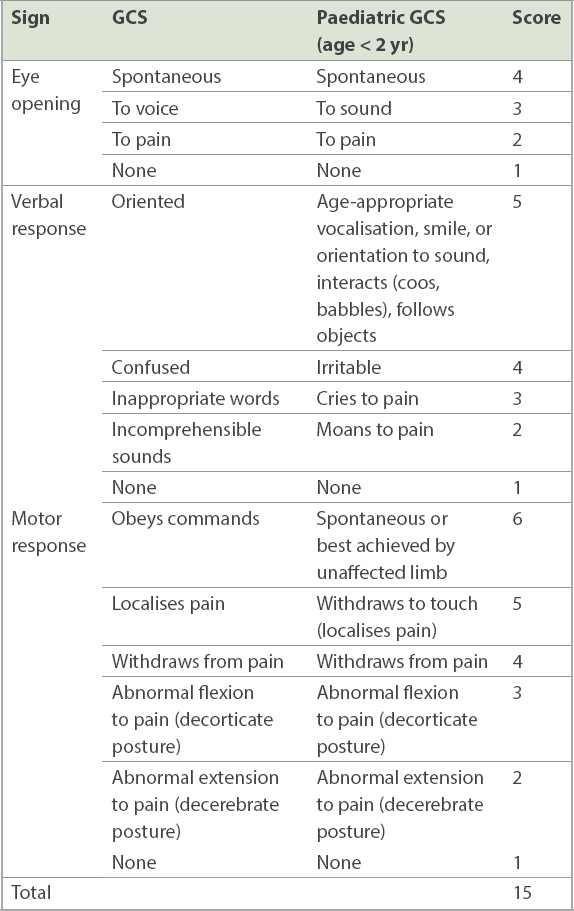
Mild TBI is defined as a Glasgow Coma Scale (GCS) (Table I) score of 13–15, measured at approximately 30 minutes after the injury or, if longer than 30 minutes, at initial presentation.(2,3) Concussion is a subtype of TBI that is caused by a direct blow to the head, face, neck or elsewhere on the body with an impulsive force transmitted to the head, resulting in the rapid onset of short-lived impairment of neurologic function that resolves spontaneously.(4) Impairment of neurologic function may manifest as loss of consciousness, amnesia, confusion or cognitive slowness.(5)
TBI is the most common cause of death or disability in the paediatric population (age 0–16 years).(6) As pivotal brain growth occurs in this population, complications that impede this growth may result in long-term physical, cognitive, socioemotional and financial implications. The disability sustained also has chronic consequences for the family and the community.(7) Fortunately, the majority of TBIs are mild, and disabilities are either absent or transient. As primary care physicians may encounter children with TBI, it is key that they have a clear clinical approach to triaging and managing them.
About half a million visits are made to the paediatric emergency departments per year in the United States for head injury complaints.(8) Locally, KK Women’s and Children’s Hospital has recorded about 5,000 such visits a year.(9) The majority of paediatric head injuries in Singapore are sustained during falls (with more than half of them occurring at home, mostly involving a high bed and sofa), followed by vehicle accidents, sports, and violence or non-accidental means.(10)
The main mechanism of paediatric TBI is dependent on age.(11) Among children aged below two years, non-accidental head injuries (NAIs) and ground-level falls are the most common, whereas falls predominate in children aged 2–4 years. From age four to teenage years, falls or road traffic accidents (RTAs) are the most common cause of TBI, while in older teenagers, RTAs are the most common cause.
WHAT CAN I DO IN MY PRACTICE?
Clinical assessment
When primary care physicians are faced with managing paediatric head injuries, tapping on their main tools – history and physical examination – is key.
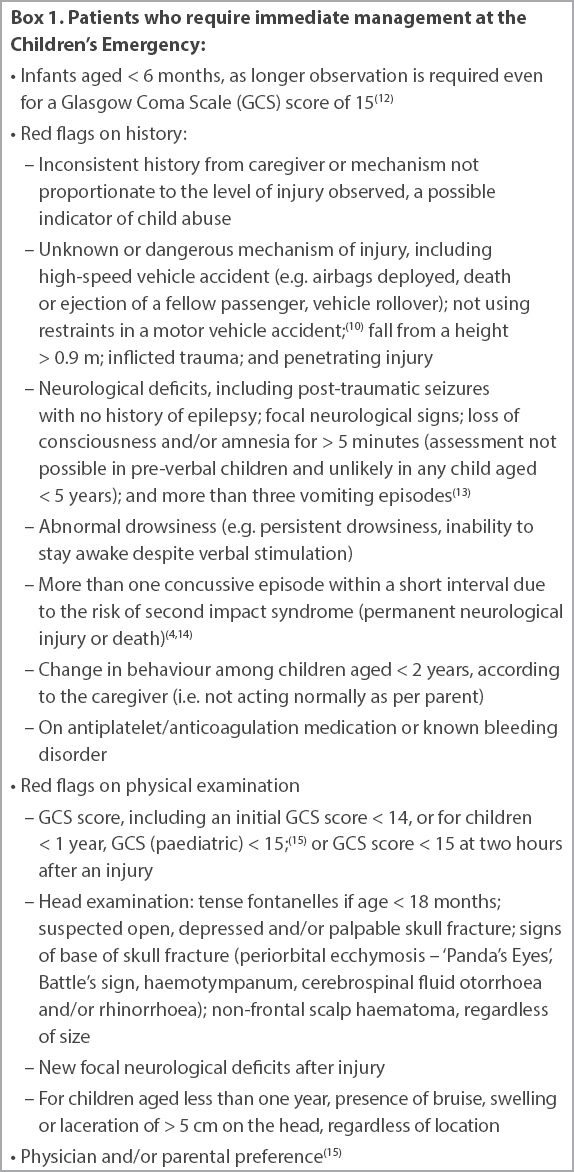
The physician should first identify those who require immediate management at the Children’s Emergency. Box 1 shows the clinical assessment sequence used to identify these patients, which is based on various clinical decision rules such as the National Institute for Health and Care Excellence guidelines and the Paediatric Emergency Care Applied Research Network (PECARN) algorithm.(12-15)
Box 1
Patients who require immediate management at the Children’s Emergency:
Clinical guideline tool
As seen in Box 1, most paediatric TBIs are mild.(11) However, 1% of these tend to be clinically important TBIs (ciTBI), which are defined as the presence of an intracranial injury on computed tomography (CT) associated with neurosurgical intervention, endotracheal intubation for the management of head injury, and hospitalisation directly related to the head injury for at least 48 hours and/or death.(15)
To safely identify children with low risk for ciTBIs who do not require neuroimaging, the PECARN algorithm(15) is a well-validated paediatric head injury clinical decision rule that primary care physicians can use. It has a sensitivity of 100.0% and 96.8% in children below two years of age and those aged two years or older, respectively. Further, it has negative predictive values of 100.00% and 99.95%, respectively. Although the PECARN algorithm has not been validated in the local context, it has been validated in various countries, all producing similar results. The algorithm can be accessed online (https://www.mdcalc.com/pecarn-pediatric-head-injury-trauma-algorithm).
Other tools such as the Canadian Assessment of Tomography for Childhood Head Injury and Children’s Head injury ALgorithm for the prediction of Important Clinical Events are widely recognised. The PECARN algorithm was selected because, in comparative studies, its algorithm had the highest sensitivity(16) in identifying patients with TBI who required CT imaging as well as validation,(17) particularly for those with minor head trauma.
Management
The primary care physician should be able to manage the majority of mild TBIs, since only a minority are ciTBIs. Skull radiographs should not be ordered, as they have no role in neuroimaging, except as part of the skeletal survey for non-accidental injury, which is usually conducted in a tertiary hospital.
Based on the PECARN algorithm, physicians who decide to observe their patients need to do so for 4–6 hours. As this would not be practical in the primary care setting, they could decide to either send their patient to the Children’s Emergency or back home in the presence of a reliable caregiver, where rest and observation for 24–48 hours are key.(18) If the latter is chosen, advice on red flags and future injury prevention (e.g. ensuring that younger children are not left alone on high beds or sofas and are instead placed on floor beds or cots, or wearing seat restraints in vehicles and helmets when cycling) must be provided, either in the form of pamphlets or website links (e.g. https://www.cdc.gov/headsup/index.html). These points are to be documented in clinical notes as well. In addition, a follow-up call and scheduled appointment should be arranged.(19) Learning from the COVID-19 situation, telemedicine consultations may also be adopted, as they provide further visual clinical assessment and a sense of reassurance to the physician and the caregiver.(20)
Children who sustain concussions should be advised not to return to playing sports or doing physical activity on the same day in order to avoid the risk of second impact syndrome. A strategy of gradual return to physical or cognitive activities should be adopted, whereby activities are gradually increased in a stepwise manner as long as the patient remains asymptomatic.(4,5,21) Students returning to school with residual symptoms may benefit from certain accommodations such as being offered a lighter workload and more frequent breaks, and being excused from loud places such as the canteen or assemblies.(5,22) On follow-up, if there are persistent symptoms with inability to resume normal activities within 2–4 weeks,(5) such as post-concussion syndrome (PCS), follow-up with a paediatric neurologist is recommended. Children at risk of PCS include those with a personal history of mood disorders, psychiatric illnesses or migraine.(23)
Special consideration – non-accidental injury
Suspicion of NAI must always be differentially considered by the primary care physician. This is especially so if the history from the informant or caregiver is inconsistent or does not match the degree of injury; or if physical examination reveals poor hygiene, malnutrition, growth restriction, multiple cutaneous bruises of different ages, suspicious pattern injuries, burn marks and skeletal injuries at different stages of healing(24) (although the latter cannot be clinically ascertained in the primary care setting).
If an NAI is suspected, the patient should be referred to the Children’s Emergency via ambulance or police escort. In Singapore, police notification must be done. As primary care physicians, we must ensure the safety of the child. The role of primary care physicians in child abuse is to ensure the safety of the at-risk child who cannot protect himself from abuse and to notify the police so that timely investigations can be performed and action can be taken to prevent further harm.
TAKE HOME MESSAGES
Disability from paediatric TBI can pose long-term consequences for the patient, family and society.
The severity of paediatric TBI can be identified through a good clinical approach and use of the PECARN clinical guideline tool.
NAIs should always be differentially considered, especially for younger children.
With the help of reliable caregivers and school support, primary care physicians can manage paediatric patients with mild TBI.
Sam was evaluated in the clinic and was eventually consolable. He recognised his name when called, was curious about the clinic setting, sat with a straight back without support and babbled. He had a small haematoma on the frontal scalp but no palpable skull fractures or tense fontanelles. He moved all four limbs well. No other injuries or bruises were noted. Following the PECARN algorithm, computed tomography was not recommended for Sam. This reassured his worried mother. She was given a pamphlet containing advice on red flags for head injury and fall prevention, as well as the clinic number to contact for any enquiries. During the clinical review in two days, Sam was behaving normally and his Glasgow Coma Scale score remained at 15, with no red flags identified.
References Centers for Disease Control and PreventionTBI:Get the Facts. Available at: https://www.cdc.gov/traumaticbraininjury/get_the_facts.html. Accessed November 1, 2020. Carroll LJ, Cassidy JD, Holm L, et al. Methodological issues and research recommendations for mild traumatic brain injury:the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury.J Rehabil Med. 2004;43 Suppl113-25. Marcin JP, Pollack MM.Triage scoring systems, severity of illness measures, and mortality prediction models in paediatric trauma.Crit Care Med. 2002;30:11 SupplS457-67. McCrory P, Meeuwisse W, DvoÅák J, et al. Consensus statement on concussion in sport--the 5th international conference on concussion in sport held in Berlin, October 2016.Br J Sports Med. 2017;51:838-47. Silverberg ND, Iaccarino MA, Panenka WJ, et al. Management of concussion and mild traumatic brain injury:a synthesis of practice guidelines.Arch Phys Med Rehabil. 2020;101:382-93. Araki T, Yokota H, Morita A.Pediatric traumatic brain injury:characteristic features, diagnosis, and management.Neurol Med Chir (Tokyo). 2017;57:82-93. Bray L.Parents'experiences of hope following a child's brain injury.Nurs Child Young People. 2015;27:22-6. Centers for Disease Control and Preventiontitle>Traumatic Brain Injury in the United States:Emergency Department Visits, Hospitalizations and Deaths 2002–2006. Available at: https://www.cdc.gov/traumaticbraininjury/tbi_ed.html. Accessed January 12, 2021. Lai L.Protect kids from severe injaes.Straits Times. 2017;Jun27. Available at: https://www.straitstimes.com/singapore/protect-kids-from-severe-injaes. Accessed January 12, 2021. Chong S, Chew SY, Feng JXY, et al. A prospective surveillance of paediatric head injaes in Singapore:a dual-centre study.BMJ Open. 2016;6:e010618. Kay A, Rodrigues D, Sharp M, Solanki GA.Special considerations in paediatric head and spinal trauma. In:Kirollos R, Helmy A, Thomson S, Hutchinson P, eds.Oxford Textbook of Neurosurgery. 2019;Oxford, UK Oxford University Press999-1008. National University Hospital, SingaporeApproach to apparently minor blunt head trauma in the children's emergency. 2020;July. National Clinical Guideline Centre (UK)Head injury:Triage, Assessment, Investigation and Early Management of Head Injury in Children, Young People and Adults.NICE Clinical Guidelines No. 176. 2014;London, UK National Institute for Health and Care Excellence. Halstead ME, Walter KD, Moffatt K.Council on Sports Medicine and FitnessSport-related concussion in children and adolescents.Paediatrics. 2018;142:e20183074. Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injaes after head trauma:a prospective cohort study.Lancet. 2009;374:1160-70. Babl FE, Borland ML, Phillips N, et al. Accuracy of PECARN, CATCH, and CHALICE head injury decision rules in children:a prospective cohort study.Lancet. 2017;389:2393-402. Mastrangelo M, Midulla F.Minor head trauma in the pediatric emergency department:decision making nodes.Curr Pediatr Rev. 2017;13:92-9. Lumba-Brown A, Yeates KO, Sarmiento K, et al. Centers for Disease Control and Prevention guideline on the diagnosis and management of mild traumatic brain injury among children.JAMA Pediatr. 2018;172:e182853. Davis GA, Purcell L, Schneider KJ, et al. The Child Sport Concussion Assessment Tool 5th Edition (Child SCAT5):background and rationale.Br J Sports Med. 2017;51:859-61. Greenhalgh T, Koh GCH, Car J.Covid-19:a remote assessment in primary care.BMJ. 2020;368:m1182. Almeida AA, Lorincz MT, Hashikawa AN.Recent advances in pediatric concussion and mild traumatic brain injury.Pediatr Clin North Am. 2018;65:1151-66. Iverson GL, Gioia GA.Returning to school following sport-related concussion.Phys Med Rehabil Clin North Am. 2016;27:429-36. Morgan CD, Zuckerman SL, Lee YM, et al. Predictors of postconcussion syndrome after sports-related concussion in young athletes:a matched case-control study.J Neurosurg Pediatr. 2015;15:589-98. Kempe CH, Silverman FN, Steele BF, et al. The battered-child syndrome.JAMA. 1962;181:17-24. Holmes JF, Palchak MJ, MacFarlane T, Kuppermann N.Performance of the pediatric Glasgow coma scale in children with blunt head trauma.Acad Emerg Med. 2005;12:814.
2. Carroll LJ, Cassidy JD, Holm L, et al. Methodological issues and research recommendations for mild traumatic brain injury: the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med 2004; (43 Suppl):113-25. https://doi.org/10.1080/16501960410023877
PMid:15083875
3. Marcin JP, Pollack MM. Triage scoring systems, severity of illness measures, and mortality prediction models in paediatric trauma. Crit Care Med 2002; 30(11 Suppl):S457-67. https://doi.org/10.1097/00003246-200211001-00011
PMid:12528788
4. McCrory P, Meeuwisse W, Dvořák J, et al. Consensus statement on concussion in sport--the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med 2017; 51:838-47. https://doi.org/10.1136/bjsports-2017-097878
PMid:29098980
5. Silverberg ND, Iaccarino MA, Panenka WJ, et al. Management of concussion and mild traumatic brain injury: a synthesis of practice guidelines. Arch Phys Med Rehabil 2020; 101:382-93. https://doi.org/10.1016/j.apmr.2019.10.179
PMid:31654620
6. Araki T, Yokota H, Morita A. Pediatric traumatic brain injury: characteristic features, diagnosis, and management. Neurol Med Chir (Tokyo) 2017; 57:82-93. https://doi.org/10.2176/nmc.ra.2016-0191
PMid:28111406 PMCid:PMC5341344
8. Centers for Disease Control and Prevention. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002-2006. Available at: https://www.cdc.gov/traumaticbraininjury/tbi_ed.html. Accessed January 12, 2021.
10. Chong S, Chew SY, Feng JXY, et al. A prospective surveillance of paediatric head injuries in Singapore: a dual-centre study. BMJ Open 2016; 6:e010618. https://doi.org/10.1136/bmjopen-2015-010618
PMid:26908533 PMCid:PMC4769425
11. Kay A, Rodrigues D, Sharp M, Solanki GA. Special considerations in paediatric head and spinal trauma. In: Kirollos R, Helmy A, Thomson S, Hutchinson P, eds. Oxford Textbook of Neurosurgery. Oxford, UK: Oxford University Press, 2019: 999-1008. https://doi.org/10.1093/med/9780198746706.003.0087
12. National University Hospital, Singapore. Approach to apparently minor blunt head trauma in the children's emergency. 2020 July.
13. National Clinical Guideline Centre (UK). Head injury: Triage, Assessment, Investigation and Early Management of Head Injury in Children, Young People and Adults. NICE Clinical Guidelines No. 176. London, UK: National Institute for Health and Care Excellence, 2014.
14. Halstead ME, Walter KD, Moffatt K, Council on Sports Medicine and Fitness. Sport-related concussion in children and adolescents. Paediatrics 2018; 142:e20183074. https://doi.org/10.1542/peds.2018-3074
PMid:30420472
15. Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet 2009; 374:1160-70. https://doi.org/10.1016/S0140-6736(09)61558-0
16. Babl FE, Borland ML, Phillips N, et al. Accuracy of PECARN, CATCH, and CHALICE head injury decision rules in children: a prospective cohort study. Lancet 2017; 389:2393-402. https://doi.org/10.1016/S0140-6736(17)30555-X
17. Mastrangelo M, Midulla F. Minor head trauma in the pediatric emergency department: decision making nodes. Curr Pediatr Rev 2017; 13:92-9. https://doi.org/10.2174/1573396313666170404113214
PMid:28393708
18. Lumba-Brown A, Yeates KO, Sarmiento K, et al. Centers for Disease Control and Prevention guideline on the diagnosis and management of mild traumatic brain injury among children. JAMA Pediatr 2018; 172:e182853.
19. Davis GA, Purcell L, Schneider KJ, et al. The Child Sport Concussion Assessment Tool 5th Edition (Child SCAT5): background and rationale. Br J Sports Med 2017; 51:859-61. https://doi.org/10.1136/bjsports-2017-097492
PMid:28446452
20. Greenhalgh T, Koh GCH, Car J. Covid-19: a remote assessment in primary care. BMJ 2020; 368:m1182. https://doi.org/10.1136/bmj.m1182
PMid:32213507
21. Almeida AA, Lorincz MT, Hashikawa AN. Recent advances in pediatric concussion and mild traumatic brain injury. Pediatr Clin North Am 2018; 65:1151-66. https://doi.org/10.1016/j.pcl.2018.07.006
PMid:30446054
22. Iverson GL, Gioia GA. Returning to school following sport-related concussion. Phys Med Rehabil Clin North Am 2016; 27:429-36. https://doi.org/10.1016/j.pmr.2015.12.002
PMid:27154854
23. Morgan CD, Zuckerman SL, Lee YM, et al. Predictors of postconcussion syndrome after sports-related concussion in young athletes: a matched casecontrol study. J Neurosurg Pediatr 2015; 15:589-98. https://doi.org/10.3171/2014.10.PEDS14356
PMid:25745949
25. Holmes JF, Palchak MJ, MacFarlane T, Kuppermann N. Performance of the pediatric Glasgow coma scale in children with blunt head trauma. Acad Emerg Med 2005; 12:814. https://doi.org/10.1197/j.aem.2005.04.019
PMid:16141014