

Abstract
INTRODUCTION
The prevalence of hiatal hernias and para-oesophageal hernias (PEHs) is lower in Asian populations than in Western populations. Progressive herniation can result in giant PEHs, which are associated with significant morbidity. This article presents the experience of an Asian acute care tertiary hospital in the management of giant PEH and parahiatal hernia.
METHODS
Surgical records dated between January 2003 and January 2013 from the Department of Surgery, Changi General Hospital, Singapore, were retrospectively reviewed.
RESULTS
Ten patients underwent surgical repair for giant PEH or parahiatal hernia during the study period. Open surgery was performed for four patients with giant PEH who presented emergently, while elective laparoscopic repair was performed for six patients with either giant PEH or parahiatal hernia (which were preoperatively diagnosed as PEH). Anterior 180° partial fundoplication was performed in eight patients, and mesh reinforcement was used in six patients. The electively repaired patients had minimal or no symptoms during presentation. Gastric volvulus was observed in five patients. There were no cases of mortality. The median follow-up duration was 16.3 months. There were no cases of mesh erosion, complaints of dysphagia or recurrence of PEH in all patients.
CONCLUSION
Giant PEH and parahiatal hernia are underdiagnosed in Asia. Most patients with giant PEH or parahiatal hernia are asymptomatic; they often present emergently or are incidentally diagnosed. Although surgical outcomes are favourable even with a delayed diagnosis, there should be greater emphasis on early diagnosis and elective repair of these hernias.
INTRODUCTION
Asian populations have a lower prevalence of hiatal hernia (HH) compared to Western populations. Population studies conducted in Sweden, Italy and China have shown a HH prevalence of 23.9%, 43.0% and 0.7%, respectively.(1-4) It is estimated that 5% of all HHs are para-oesophageal hernias (PEHs).(5)
Large PEHs with herniation of more than half of the stomach into the chest are termed giant PEHs.(6) Giant PEHs are associated with significant morbidity due to the increased risk of volvulus, gangrene, perforation and massive bleeding.(7) To avoid serious complications, elective repair has been advocated for giant PEHs and demonstrated favourable mortality rates (< 1%) in a large case series involving a Western population.(8) However, no similar studies or randomised trials examining the utility of elective repair for giant PEHs have been conducted in Asian centres. This may be due to the low incidence of the disease. Thus, Asian literature reporting on this disease is limited to isolated case reports.(9,10)
Parahiatal hernia is an even rarer entity. It is often preoperatively misdiagnosed as PEH, as they have similar radiological findings. To date, only four cases of parahiatal hernia have been reported in Western centres and 11 cases in Asian centres.(11-17) The reported incidence is low, accounting for only 1.6% and 0.35% of all preoperatively diagnosed PEHs in Western and Asian centres, respectively.(11,13) Since the management of parahiatal hernia differs from that of PEH, it is important that these two entities are effectively differentiated.
The aim of this study was to present the experience of an Asian acute care tertiary hospital in the management of giant PEHs and parahiatal hernias, in order to enhance the understanding of these rare but important conditions. The presentation, diagnosis, and approach to emergency and elective surgical treatment of PEHs and parahiatal hernias are reviewed and discussed.
METHODS
We performed a retrospective review of endoscopic and surgical records from the Upper Gastrointestinal Surgery Service, Department of Surgery, Changi General Hospital, Singapore. Only records that were dated between January 2003 and January 2013 were reviewed.
PEHs, also known as Type II HHs, occur when a localised defect in the phreno-oesophageal membrane allows upward migration of the gastric fundus through the oesophageal hiatus while the gastro-oesophageal junction (GEJ) remains fixed to the preaortic fascia and median arcuate ligament. Progressive enlargement of the oesophageal hiatus and hernia sac may result in Type III HH. The different types of HH are presented in
Table I
Types of hiatal hernia.
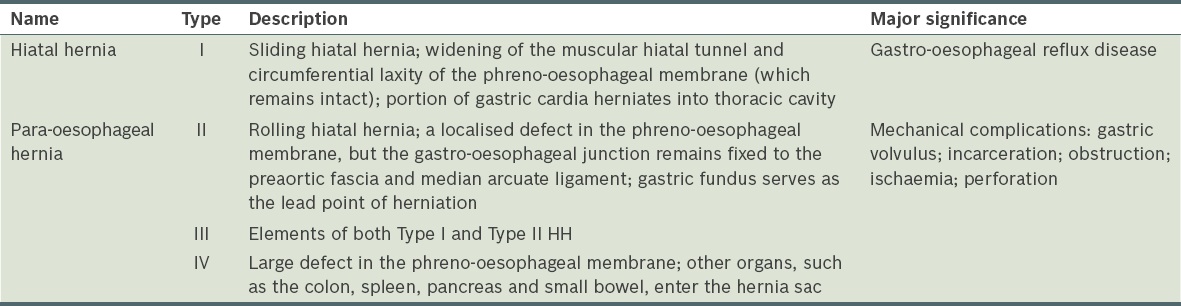
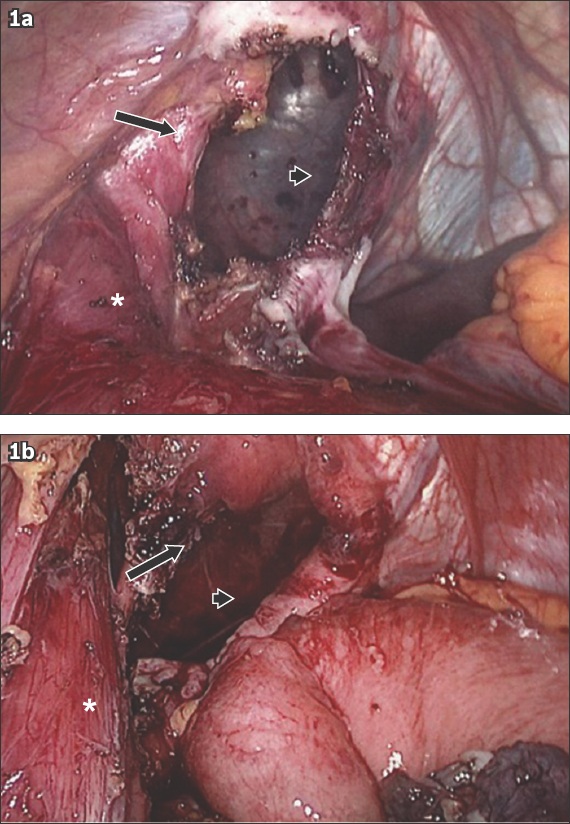
Fig. 1
Intraoperative photographs of (a) Patient A and (b) Patient B show parahiatal hernias (arrowheads) adjacent to the intact left diaphragmatic crura (arrows). The oesophagus is denoted by the asterisks (*).
PEH was diagnosed using computed tomography (CT) of the chest and abdomen in all but one case. Preoperatively, no further investigation was performed if the patient had symptoms of gastric outlet obstruction, small bowel obstruction or respiratory compromise, and required emergency surgery. Patients who were asymptomatic or had only mild pain that could be controlled using analgesics were managed electively; they underwent further preoperative evaluation with upper endoscopy and contrast studies of the upper gastrointestinal tract. The choice of surgical access was determined according to each patient’s presentation. Open procedures were performed for patients who presented emergently with obstructive symptoms or respiratory compromise, while laparoscopic surgeries were performed for elective cases where the patients were asymptomatic or had minor symptoms.
The open approach utilised an upper midline incision. Dissection of the diaphragmatic hiatus was performed to expose the crura, followed by reduction of the herniated contents into the abdominal cavity. The hernia sac was then dissected off the pleura and the thoracic oesophagus was mobilised to ensure an adequate length of abdominal oesophagus, with the GEJ brought within the abdominal cavity. When indicated, posterior gastropexy and gastrostomy were performed for fixation of the stomach to the anterior abdominal wall to prevent recurrent herniation. A non-encircling biocompatible mesh was placed when the crura could not be repaired without tension. Anti-reflux procedures were not performed in the emergency setting.
All elective patients underwent laparoscopic repair. The French position was routinely used, with the surgeon standing between the patient’s legs and an assistant standing on the patient’s right. Two 5-mm and two 12-mm ports were placed in the upper abdomen for the working instruments. The left lateral segment of the liver was retracted using a Nathanson retractor for exposure of the diaphragmatic hiatus.
In cases of giant PEH, the gastrohepatic ligament at the level of the right crus was first dissected. This dissection was carried to the left side, over the anterior surface of the oesophagus and toward the gastrosplenic ligament. Attachments to the gastric fundus were divided, and the dissection was completed with the dissection of the retro-oesophageal space to expose the right and left crura. The contents of the hernia sac would then be reduced into the abdomen. If present, the colon and small bowel were reduced before the stomach. The hernia sac was dissected off the pleura using a combination of blunt sweeping dissection and sharp dissection with a hook diathermy or harmonic scalpel aided by the pneumoperitoneum.
In all cases of giant PEH, the intrathoracic oesophagus was routinely mobilised up to the level of the inferior pulmonary vein to ensure that the intra-abdominal segment of the oesophagus was tension-free and did not retract into the thoracic cavity. Retraction of a Penrose drain or nylon tape looped around the GEJ was employed to aid this process. The diaphragmatic defect was closed without tension using interrupted sutures and mesh. Additional sutures were placed in the diaphragm anterior to the oesophagus to prevent over-angulation. The fundus of the stomach was mobilised by dividing the short gastric vessels, and anterior 180° fundoplication was routinely performed. Finally, the dissected hernia sac was interposed between the mesh and oesophagus to reduce the risk of mesh erosion.
For elective patients, a water-soluble contrast study was performed a day after surgery. If the study demonstrated a smooth flow of contrast across the hiatal repair and fundoplication, the patient was started on liquids. The patient’s diet would then be gradually adjusted over a range of consistencies, as tolerated by the patient and guided by a dietician. Most patients were on a soft diet by postoperative day 5–7 and a normal diet 1–2 weeks after the initiation of the soft diet. Emergency patients usually had the contrast study performed a few days after surgery, when they were able to get out of bed. They were progressed to a normal diet in a similar manner as the elective patients.
All patients were seen a month after discharge to evaluate their progress. Thereafter, they were seen at six-month intervals. Water-soluble contrast swallow study was performed if there was suspicion of hernia recurrence. Water-soluble contrast swallow study or CT was also performed at six months and one year after surgery to exclude asymptomatic recurrence. All patients with mesh placement were examined using upper endoscopy at one year after surgery to exclude mesh erosion.
RESULTS
In our retrospective review, we identified 1,001 patients with an endoscopic diagnosis of hiatal hernia. Of these patients, eight had a diagnosis of giant PEH and two had a diagnosis of parahiatal hernia. These ten patients, whose median age was 54.4 (range 38.0–79.0) years, underwent surgical repair between January 2003 and January 2013. Six of them presented acutely – four required emergency surgery and two were managed conservatively before undergoing semi-elective surgery a week after presentation. The clinical presentation, intraoperative findings and postoperative outcomes of the four patients who underwent emergency surgery are presented in
Table II
Details of the patients who underwent emergency surgery (n = 4).
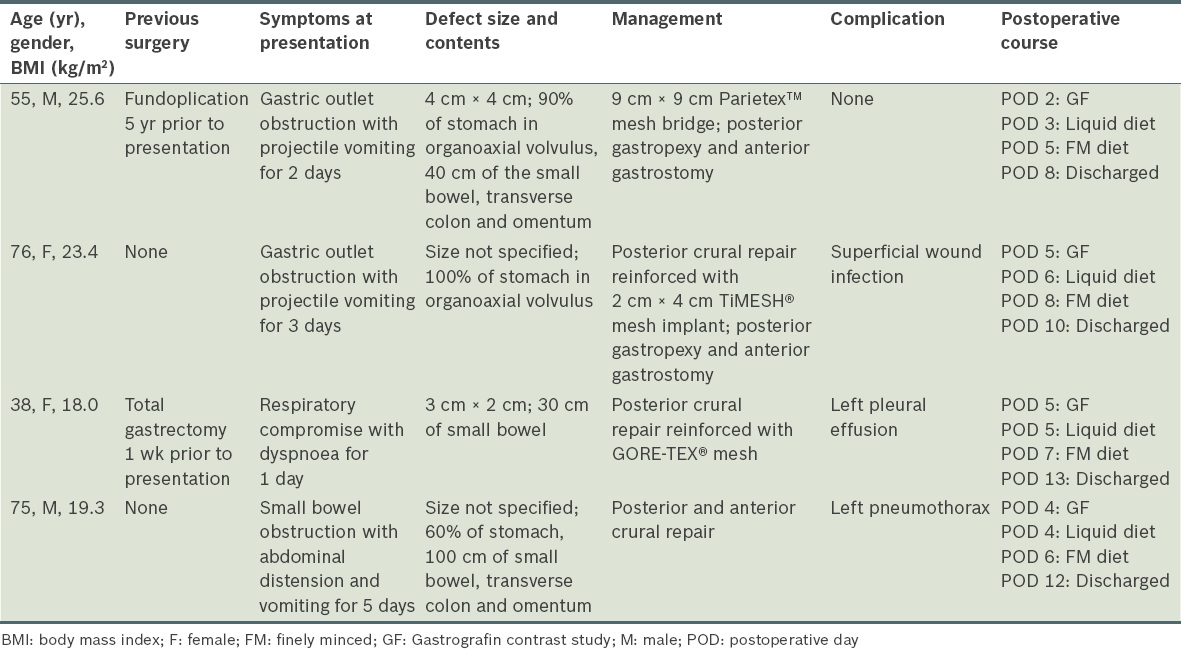
All four emergency surgeries were performed via midline laparotomy. In two cases, complete reduction of the hernia contents was only possible after the constriction was widened via an incision in the crura. The small bowel and transverse colon were usually reduced before reduction of the stomach. Two of the four patients with symptoms of gastric outlet obstruction had constriction of the pylorus at the level of the diaphragmatic hiatus, due to complete or almost complete herniation of the stomach with associated organoaxial gastric volvulus. These two patients required posterior gastropexy and anterior gastrostomy to reduce the risk of recurrent herniation and gastric volvulus. Three of the four patients underwent mesh repair – one received mesh repair because the defect was too large to be closed primarily without tension and the mesh had to be used to bridge the defect, while the other two patients had mesh reinforcement of the primary posterior crural repair. As there was no gastric or bowel ischaemia, bowel resection was not necessary in these three cases.
Elective repair was carried out in the remaining six patients who had minor or no symptoms. The procedure of choice for such patients was laparoscopic repair. The presentation, type and size of hernia defects, management, and postoperative course of these six patients are presented in
Table III
Details of the patients who underwent elective surgery (n = 6).
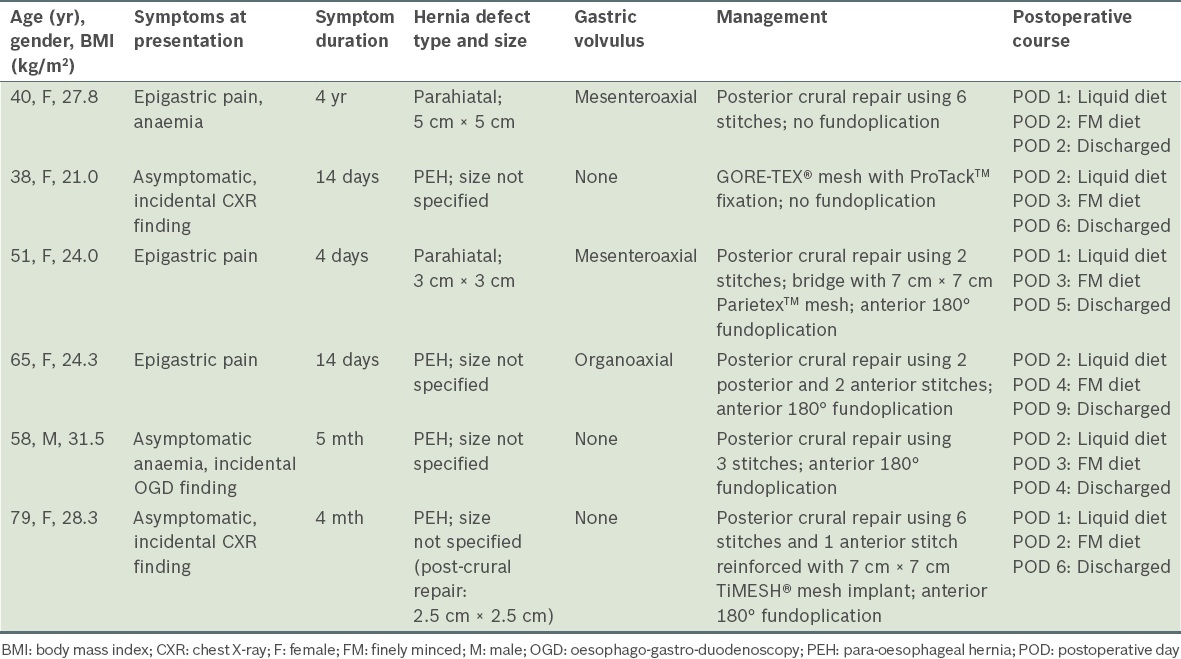
Among the six patients who underwent elective surgery, four had anterior 180° fundoplication and three had hiatal plasty with prosthetic mesh. Of the three patients who had hiatal plasty with prosthetic mesh, two had defects that could not be closed primarily without tension and meshes were used to bridge the defects, while one had a tear in the diaphragm after primary repair, which was reinforced with a TiMESH® mesh implant.
Two cases of parahiatal hernias were incidentally discovered during dissection of the hernia sac. In both cases, the hernia defect was found lateral to the left crus of an intact GEJ. In one case, the 3-cm hernia defect could not be approximated without excessive tension due to a fibrotic ring around the defect, and thus, a biocompatible mesh repair was employed. In the other case, the 5-cm hernia defect was repaired with primary suture using interrupted polypropylene.
The median time to a liquid diet was 1.5 days among patients who had elective surgery, while the time to a finely minced diet and time to discharge were three and five days, respectively. The recovery progress of the six patients who underwent elective surgery (i.e. laparoscopic repair) was faster than that of the four patients who underwent emergency surgery (i.e. open surgery performed via a midline laparotomy); we did not test the statistical significance of this finding, as the numbers of the two groups were small.
For all ten patients, the mean duration of follow-up was 16.3 (range 4.0–43.0) months. Although three of the four patients who underwent emergency surgery had minor complications, none required a repeat surgery and there were no deaths. There were no cases of mesh erosion, dysphagia, recurrence of PEH and gastric volvulus among both the patients who underwent emergency surgery and those who underwent elective surgery. At follow-up, all patients reported minimal or no symptoms.
DISCUSSION
Although HHs, gastro-oesophageal reflux disease (GERD) and oesophagitis are frequently observed to coexist, the exact nature of their relationship with one another is not completely understood.(19,20) In a large-scale study conducted in Singapore, which involved 11,934 symptomatic patients who underwent upper endoscopy, the prevalence of oesophagitis was only 3.3%.(21) Other studies that were conducted in Korea, Hong Kong and Taiwan also reported a low prevalence of GERD (5%–17%).(22-24) Based on these numbers, we can expect a similarly low prevalence rate of HH in Asian populations. Kang and Ho provided evidence for this in their study, which showed that the prevalence of HH among dyspeptic patients in Singapore was only 4% (n = 7/173) as compared to 23.6% (n = 50/212) among dyspeptic patients in England.(25) It has been hypothesised that the differences in predisposing factors (such as body mass index, oesophageal sphincter pressure and dietary habits) between Asian and Western populations may account for the difference in the prevalence of oesophagitis and HH.(26) However, little evidence exists to support this hypothesis or to account for the significant differences in prevalence of oesophagitis and HH in Asian and Western populations.
Only approximately 5% of all HHs are PEHs;(5) this could account for the paucity of PEH cases seen in Asian populations. Furthermore, Asian patients with PEH may have minimal or no symptoms, or nonspecific symptoms (ranging from mild nausea and abdominal distension to acute presentation with obstructive symptoms and dyspnoea), which make early and accurate diagnosis challenging, especially in an emergency situation.(9) The difficulty in accurately diagnosing PEH could result in the underreporting of cases in our Asian population, as patients with PEH may not be identified because they are asymptomatic, or they may be misdiagnosed as having other conditions. Thus, in the Asian context, clinicians need to have a high index of suspicion when patients present with acute upper gastrointestinal tract symptoms.
Mortality after emergency surgery for PEH may be as high as 40% (mean 17%).(27) Acute gastric volvulus, which is frequently associated with PEH, has a mortality rate of 30%–50%, with major sequelae such as gastric necrosis, perforation and hypovolaemic shock.(28) In the present study, although five of the ten patients with PEH or parahiatal hernia had associated gastric volvulus, there were no mortalities. Two of these five patients successfully underwent open repair, while the remaining three patients underwent laparoscopic repair with equally favourable outcomes. Although the numbers are small, this finding suggests that laparoscopic repair may be a feasible option for the treatment of PEH with associated gastric volvulus; this has been reported in other studies.(29,30) A more recent study by Teague et al also showed good results with no mortality in all of their 36 patients, five of which had chronic volvulus that were treated conservatively.(31) It is worth noting that, even though PEH is a rare condition in Asian populations and experience with PEH is limited, there were no mortalities in the present study.
Although laparoscopic repair is gaining popularity, the open approach may be safer for patients who present acutely with obstructive symptoms, haemodynamic instability or respiratory instability, or if gastric ischaemia is suspected. This is because open surgery allows for easier gastric decompression and faster reduction of the herniated stomach as compared to laparoscopic surgery. In the present study, laparoscopic repair was reserved for stable, minimally symptomatic or asymptomatic patients who were scheduled for elective surgery.
Repair of the crura and reconstitution of the hiatus is the most important part of the operation to prevent recurrence. In our hospital, primary repair of the crura posterior to the oesophagus with interrupted polypropylene sutures is preferred, as the diaphragmatic crura are stronger posteriorly. However, excessive placement of the sutures posteriorly can lead to over-angulation of the GEJ and cause postoperative dysphagia.(32) As such, some sutures had to be placed in the crura anterior to the oesophagus to prevent over-angulation of the GEJ.
In our hospital, a prosthetic mesh is not used if primary repair can be performed without tension. An exception is made if parts of the patient’s diaphragm are thinned out and may subsequently tear, leading to failure of therapy; in such cases, the mesh is used as a reinforcement of the primary repair. In cases where the hiatal defect cannot be approximated without tension, a prosthetic mesh is used as a bridge to patch the enlarged hiatus without approximating the crura while allowing the passage of the oesophagus.(33) Proponents of the mesh cite lower hernia recurrence rates, while opponents cite the occurrence of complications such as dysphagia, oesophageal stenosis and erosion of the mesh into the oesophagus.(34,35) In the present study, the dissected hernia sac was routinely used as an interposition between the mesh and oesophagus to reduce the risk of erosion; there were no cases of recurrence, mesh erosion or dysphagia among the patients who received mesh implants.
As demonstrated in the present study, parahiatal hernia is a possible alternate diagnosis for preoperatively diagnosed PEH. In a study conducted by Scheidler et al in a single Western centre, the incidence of parahiatal hernia in their cohort of laparoscopically treated HHs was 0.2% (2/917).(11) Similarly, Palanivelu et al reported a low incidence of parahiatal hernia (0.35%, 4/1,127) in their cohort of HH patients who were laparoscopically treated in a single Asian centre.(13) The unusually high proportion of parahiatal hernias in our hospital (20%, 2/10) might either indicate an underreporting of HHs (thereby leading to the smaller overall number of HHs being treated), or suggest that parahiatal hernia is an underappreciated condition that should be actively excluded in the differential diagnosis during surgical exploration of all PEHs.
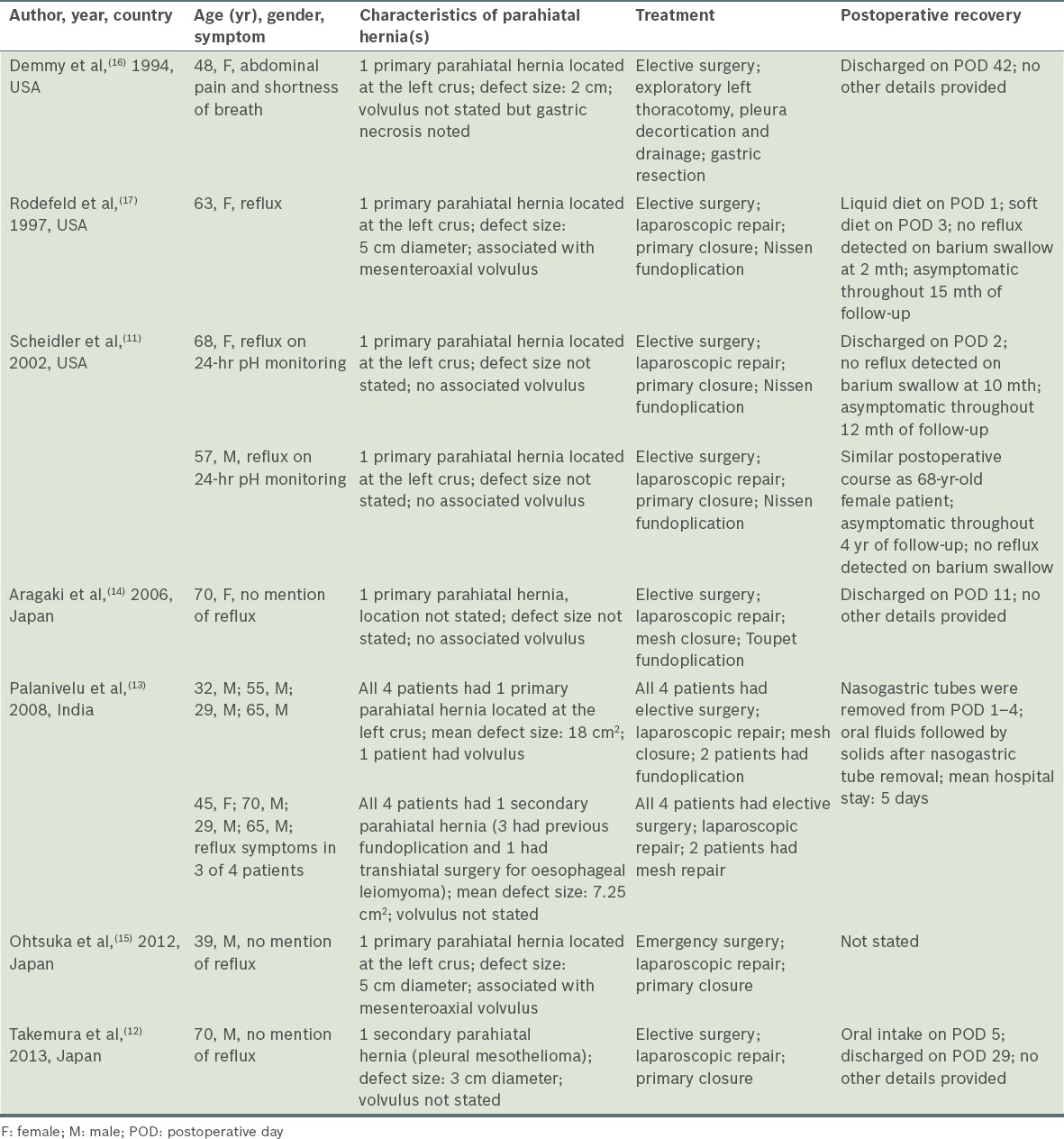
A comparison of parahiatal hernia cases is shown in
Table IV
Comparison of the clinical characteristics and surgical treatment of parahiatal hernias.
In the present study, all ten patients reported minimal or no symptoms during follow-up. Investigations were performed routinely to review the effects of the mesh implant and to exclude mesh erosion. Although it is known that anatomical recurrences can occur in up to 42% of laparoscopically repaired HH cases, these patients are rarely symptomatic and very few require repeat surgery.(36,37) There were no patients with symptomatic recurrence in our study.
In conclusion, giant PEHs and parahiatal hernias are rare conditions in the Asian context. Although most patients with either condition are asymptomatic and incidentally diagnosed, some may present emergently. A significant proportion of the patients in the present study underwent emergency surgery. Although patients who underwent emergency open surgery had good surgical outcomes, more emphasis should be directed toward early diagnosis and elective laparoscopic repair of such hernias, as laparoscopic repair may offer a faster postoperative recovery. The surgical approach to crural dissection may differ if parahiatal hernia is suspected, and this differential diagnosis should be actively excluded.