Singapore Med J 2020; 61(11): 584-590 doi: https://doi.org/10.11622/smedj.2019109
Patient-centred and not disease-focused: a review of guidelines and multimorbidity
Kim Yao Ong1, Poay Sian Sabrina Lee2, PhD, Eng Sing Lee2, MBChB, FCFP
Author Information >Copyright and License information >
1Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore 2Clinical Research Unit, National Healthcare Group Polyclinics, Singapore Correspondence: Dr Lee Eng Sing, Principal Clinician Researcher, Clinical Research Unit, National Healthcare Group Polyclinics, 3 Fusionopolis Link, Nexus@one-north, South Lobby, #05-10, Singapore 138543. eng_sing_lee@nhgp.com.sg
Single-disease clinical practice guidelines (CPGs) are not designed to consider patients with multiple chronic conditions, or multimorbidity. Applying multiple CPGs to a single patient may create an overwhelming treatment burden resulting in poor adherence and clinical outcomes. No studies on the cumulative treatment burden from multiple CPGs have been done in Singapore. We described the treatment burden on a hypothetical patient with six chronic conditions when multiple CPGs were applied, and appraised each CPG with respect to the patient-centred care of older adults with multimorbidity.
METHODS
A treatment plan was developed for a hypothetical 72-year-old woman with asthma, depression, diabetes mellitus, dyslipidaemia, hypertension and osteoarthritis according to the latest CPG recommendations. Treatment burden was quantified in terms of time spent, cost, and the number of appointments and medications. Each CPG was appraised with respect to the care of older adults, patients with multimorbidity and patient-centred care.
RESULTS
Following the CPGs strictly, an average of about two hours was spent daily taking 14 different medications and following 21 non-pharmacological recommendations. Her out-of-pocket payment was SGD 104.42 monthly despite a near 90% subsidy on healthcare bills. Patient-centred care of older adults with multimorbidity was inadequately addressed in all six CPGs.
CONCLUSION
When six CPGs were cumulatively followed, the treatment burden was time-consuming, costly and disruptive. Patients’ goals and preferences must guide prioritisation of care such that treatment burden remains minimally disruptive to their lives. Developing future CPGs to deliver patient-centred rather than disease-focused care will be crucial to the management of multimorbidity.
Keywords: chronic disease, comorbidity, multimorbidity, practice guidelines, primary care
INTRODUCTION
Multimorbidity is the co-occurrence of two or more chronic conditions in an individual.(1,2) It is associated with increasing age and is most prevalent among older adults.(3) Managing multimorbidity is challenging, as current healthcare systems are predominantly guided by single-disease pathways.(4) For example, most clinical practice guidelines (CPGs) have a single-disease focus.(5) They inadequately address patients with multimorbidity(5) in whom treatment burden, defined as the total healthcare workload experienced by these patients,(6) is cumulative. Consequently, these patients experience a poor quality of life, high healthcare expenditures, polypharmacy, and increased risk for adverse drug events and mortality(7) in a healthcare system with poor coordination and integration.(8) In Singapore, where one in five Singaporeans will be aged 65 years or older by 2030,(9) it is imperative to optimise management of multimorbidity. Following multiple single-disease CPGs may create an overwhelming treatment burden that leads to poor adherence, wasted resources and poor clinical outcomes.(10) While previous studies examining international guidelines have found that treatment burden greatly increases with an increasing number of chronic conditions,(11-13) no similar studies have been conducted in Singapore.
We aimed to identify gaps in current CPGs that run contrary to the goal of patient-centred care, which is for treatment burden to be minimally disruptive to patients’ lives. The primary study objective was to describe the treatment burden of a hypothetical patient with six common chronic conditions in the primary care setting when multiple single-disease CPGs are applied. The secondary objective was to appraise the extent to which CPGs address older adults, multimorbidity and patient-centred care.
METHODS
A treatment plan was developed for our hypothetical patient Mdm Wong, a 72-year-old widow with asthma, depression, diabetes mellitus, dyslipidaemia, hypertension and osteoarthritis, all moderate in severity, based on the latest CPG recommendations (Appendix 1). Mdm Wong lives alone and receives a monthly annuity of SGD 650 from her Central Provident Fund account, the mandatory national savings scheme in Singapore,(14) and visits the nearest polyclinic for her multimorbidity. For the purpose of this study, generic medications with the least frequent dosing regimen and combined recommendations applicable to multiple CPGs were chosen whenever possible.
From the 20 chronic conditions that are under the Ministry of Health (MOH) Chronic Disease Management Programme and therefore eligible for subsidies (Appendix 2),(15) six conditions commonly managed in the primary care setting were selected, including a chronic pain condition (osteoarthritis) and a mental health condition (depression), to reflect the full breadth of multimorbidity. MOH CPGs produced within the last ten years were selected, as they are most appropriately matched to local practice. As the MOH CPGs for asthma and osteoarthritis had not been updated in the past ten years, international guidelines that are most often used locally (Appendix 2) were selected,(16-21) namely the Global Strategy for Asthma Management and Prevention guidelines from the Global Initiative for Asthma and the Osteoarthritis: Care and Management in Adults guidelines from the National Institute for Health and Care Excellence (NICE). CPGs were evaluated based on criteria selected from similar studies examining the applicability of guideline recommendations to older adults, patients with multimorbidity and patient-centred care.(11,13)
Treatment burden concerning time spent, cost, and the number of appointments and medications was quantified. Estimates of time spent on various health-related activities (HRAs) were obtained from the published literature(22,23) and operational data from the National Healthcare Group Polyclinics (NHGP) (Appendix 3). Both subsidised and unsubsidised costs of treatment in the primary care setting were calculated. The unsubsidised costs included the national goods and services tax (GST) at the prevailing rate of 7% to reflect the true cost to the healthcare system. The out-of-pocket payment by Mdm Wong after MOH subsidy with GST absorbed, and additional coverage from the Pioneer Generation Package (PGP), which entitles patients to an additional 50% off their subsidised healthcare bill,(24) and the Community Health Assist Scheme (CHAS), which enables patients to make claims up to SGD 135 per visit and SGD 54 per year from their Medisave account,(25) were also reported. This was expressed as a percentage of her monthly annuity. Treatment for acute exacerbations of chronic diseases was not considered.
RESULTS
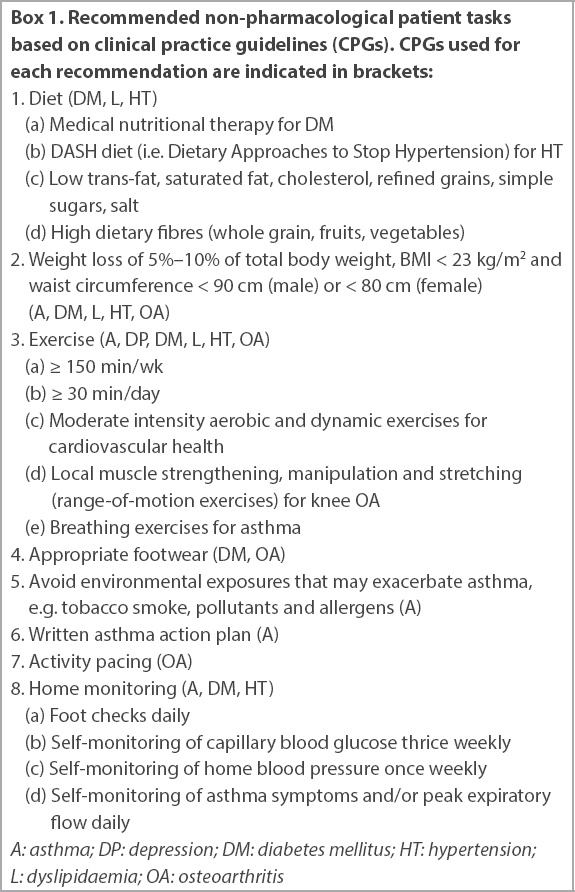
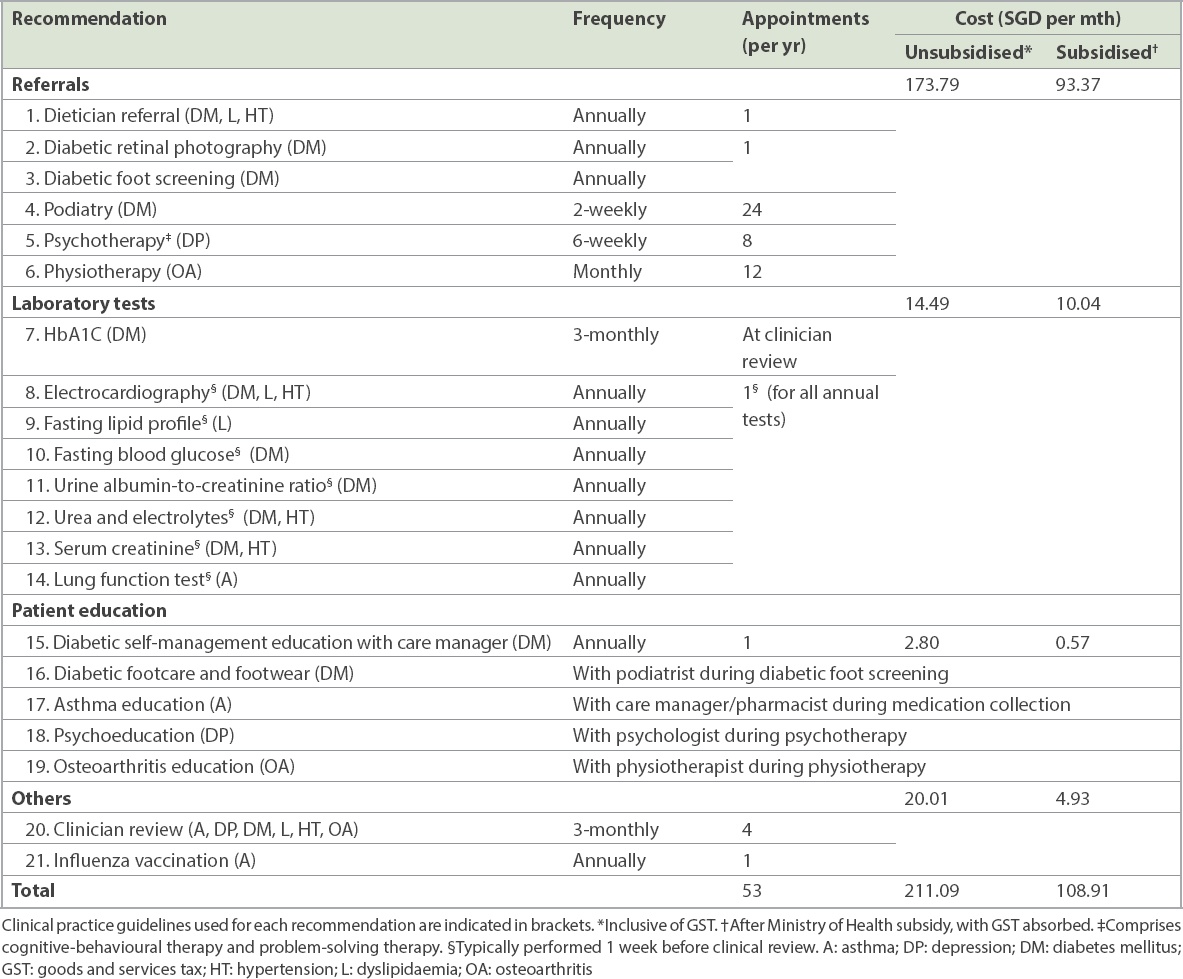
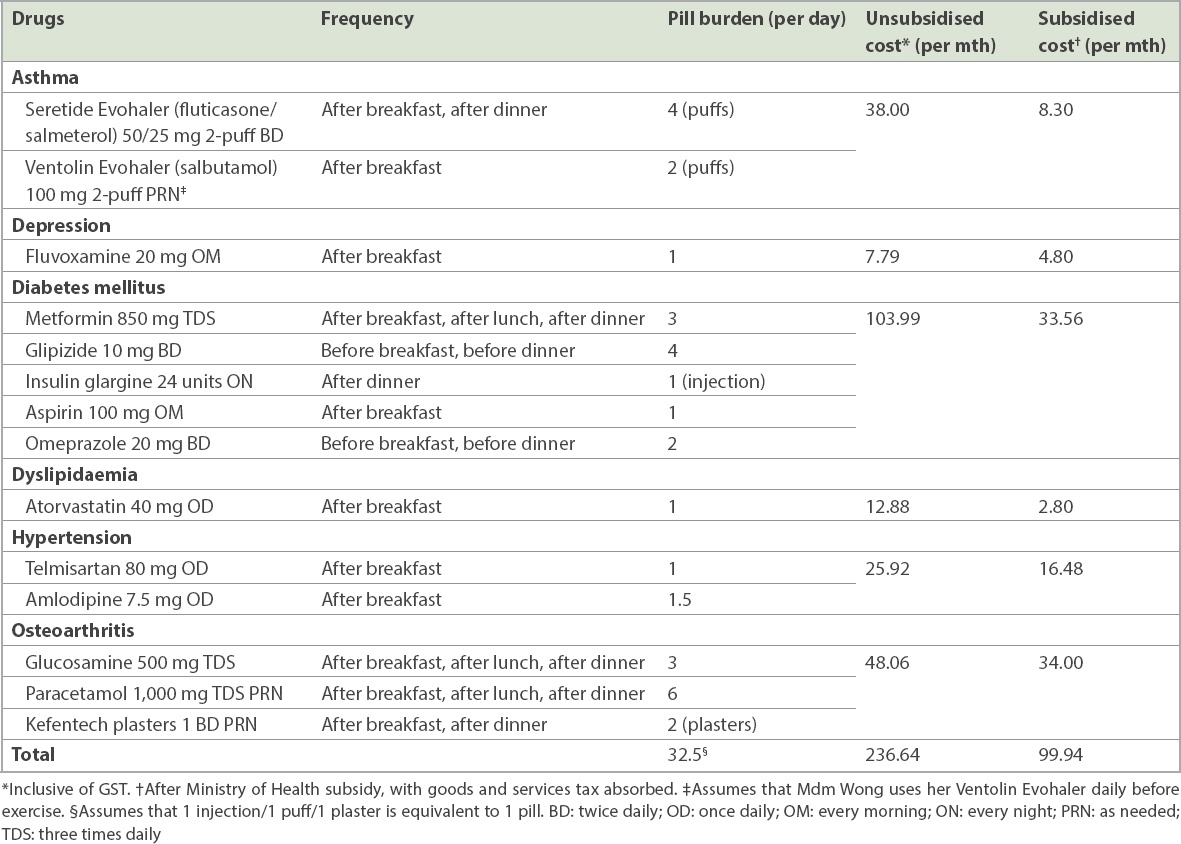
For this study, treatment burden was shown in terms of a total of 21 non-pharmacological recommendations (Box 1 & Table I). These included six referrals, eight laboratory tests and five patient-education interventions, equating to 53 polyclinic appointments annually for Mdm Wong. She would take 14 different types of medications, equivalent to 32.5 pills taken at five different times daily, assuming that ‘as needed’ salbutamol is taken once daily before exercise, paracetamol thrice daily and kefentech plasters twice daily for pain relief (Table II). In addition, she would spend up to 64.53 hr/mth (2.15 hr/day) on HRAs, including 7.87 hr/mth attending appointments, 8.67 hr/mth monitoring her diseases, 12.00 hr/mth taking medications, 16.00 hr/mth following the recommended diet and 20.00 hr/mth on exercise.
Box 1
Recommended non-pharmacological patient tasks based on clinical practice guidelines (CPGs). CPGs used for each recommendation are indicated in brackets:
Table I
Recommended non-pharmacological clinician tasks based on clinical practice guidelines.
Table II
Pharmacological recommendations from clinical practice guidelines for Mdm Wong.
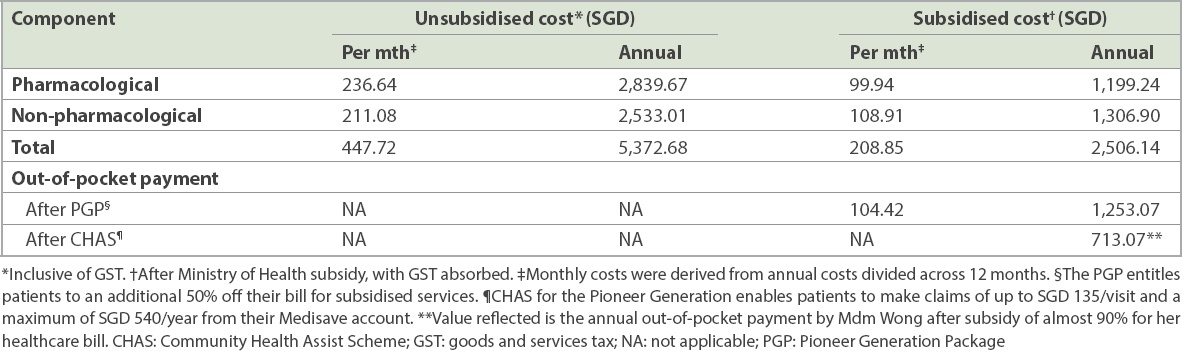
Table III shows the expected treatment costs for Mdm Wong. Without subsidies, a total of SGD 447.72 (SGD 236.64 for medications), 68.9% of her monthly annuity, would be spent monthly. After MOH and PGP subsidies, the monthly payment would decrease to SGD 104.42 monthly (SGD 49.97 for medications), 16.1% of her monthly annuity. This equates to a more than 50% reduction in her monthly payment. Unfortunately, her annual CHAS claim limit (of SGD 540 per year) would be exhausted in five months and she would have to make monthly out-of-pocket payments of SGD 104.42 for the remaining months (Table III). The treatment regimen would cost the healthcare system SGD 5,372.68 annually (SGD 2,839.67 for medications).
Table III
Out-of-pocket treatment costs for Mdm Wong.
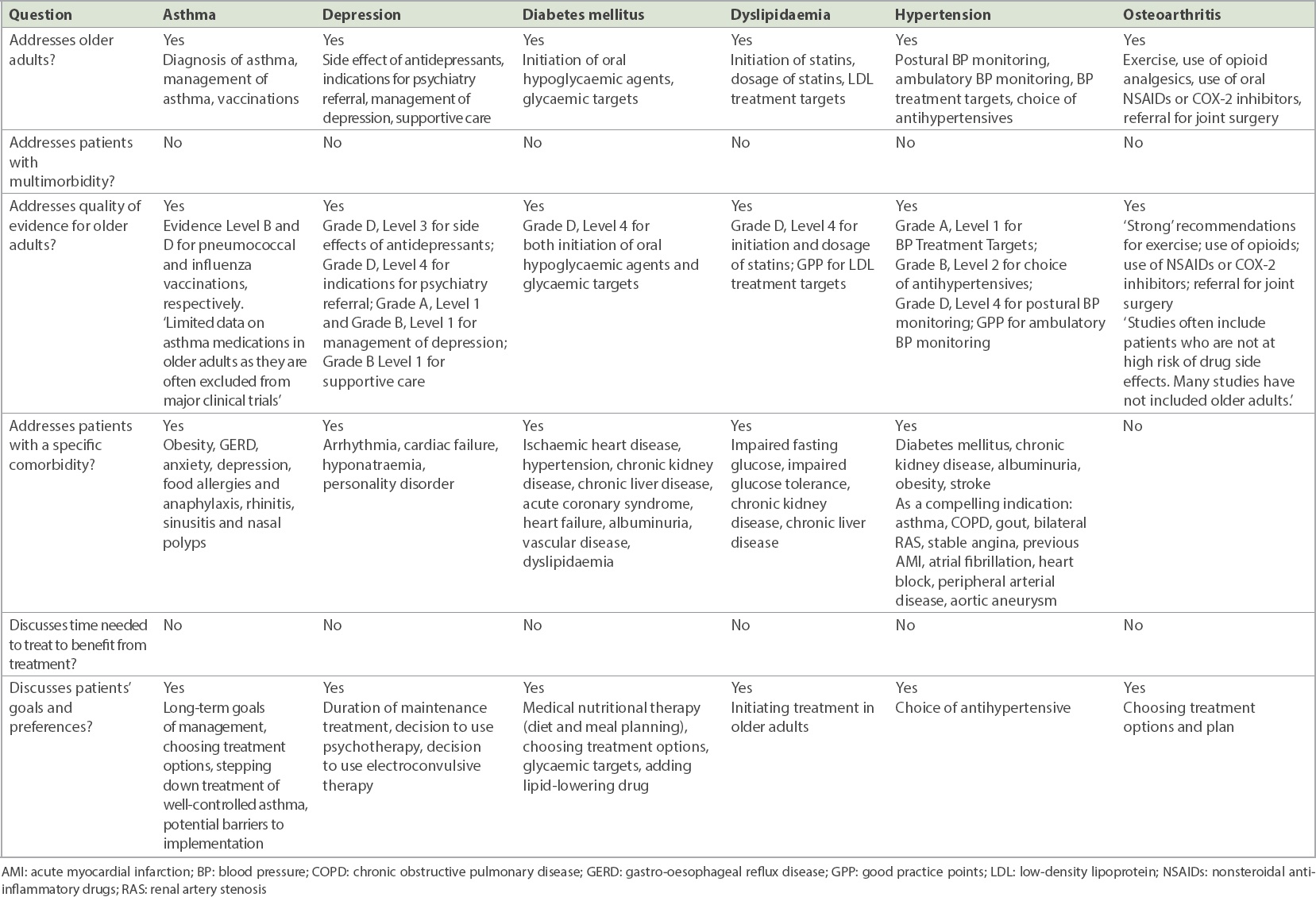
Although each individual CPG considers older adults, only four of the CPGs (asthma, depression, dyslipidaemia and hypertension) have dedicated sections with extensive information and evidence (Table IV). Across the six CPGs, recommendations range from modified treatment targets (dyslipidaemia and diabetes mellitus) to specific pharmacological recommendations (hypertension and depression). Most pertain to the increased risk of adverse effects and drug interactions in older adults. Among the recommendations for older adults, only five are based on the highest level of evidence. All except the osteoarthritis CPG mention at least one specific comorbidity (Table IV), and this is most extensive in the hypertension CPG. However, none of the CPGs address multimorbidity or multiple comorbidities. All CPGs include patients’ goals and preferences. Three CPGs (dyslipidaemia, hypertension and osteoarthritis) recommend tailoring treatment to the patient, but with no disease-specific elaboration. The other three CPGs (asthma, diabetes mellitus and depression) discuss patient preferences regarding specific treatment options or targets. None of the CPGs address the time needed to treat to benefit (Table IV).
Table IV
Applicability of clinical practice guidelines to older adults with multimorbidity and patient-centred care.
DISCUSSION
Similar to Mdm Wong, about one in ten older adults in Singapore has six or more chronic conditions (unpublished data from NHGP). The cumulative treatment plan from six CPGs has created a treatment burden that is time-consuming, costly and disruptive to her daily living. The CPGs also inadequately address the issues of older adults with multimorbidity and patient-centred care. Our results highlight the various shortcomings of single-disease CPGs when managing patients with multimorbidity in Singapore, a finding that is consistent with previous studies from other countries.(11,13,26)
Compared with a 2015 study in which patients with six conditions required up to 18 different medications,(12) Mdm Wong was prescribed 14 medications for her six conditions. This was due to differences in the selection of conditions and disease severity defined.(13) In addition, the cumbersome pharmacological regimen involving a high pill burden and the complexity associated with preparing a large number of medications every day adds to the treatment burden. Therefore, polypharmacy is associated with increased medication errors, adverse drug events, drug interactions and hospital admissions.(27) The 21 non-pharmacological recommendations for six conditions are comparable to those of previous studies,(11,13) with differences due to the varying number of chronic conditions and the disease severity defined.
Russell et al and Yen et al have conducted studies to examine the time spent on HRAs in the American and Australian setting, respectively.(22,28) In Singapore, ready-to-eat food and groceries are readily accessible close to residential areas, which may be different for patients residing in America and Australia. Therefore, in our study, Mdm Wong spends an average of 65 hours a month on HRAs, significantly lower than the 81 hours reported for six conditions by Buffel et al.(12) Furthermore, for polyclinic appointments, the median time estimates for waiting time and time spent receiving healthcare are ten minutes and 15–25 minutes, respectively. These operational values obtained from the NHGP are conservative compared to the mean values of 47 minutes and 72 minutes, respectively, in the American Time Use Survey.(28) Lastly, our patient had the option of bundled appointments. Compared to the average of seven appointments a month from Buffel et al,(12) Mdm Wong only requires an average of four appointments per month. In Singapore, the polyclinics providing public primary healthcare make multiple healthcare services available at a single site, thereby allowing patients to make minimal trips and save time travelling to each appointment. Nevertheless, the allied health services that are available vary between polyclinics, and most polyclinics do not house all services on-site. Hence, while it is theoretically possible to attend multiple appointments in a single sitting (e.g. psychologist, physiotherapist and podiatrist on the same day), our study has not reflected that.
We estimated that the annual out-of-pocket payment by Mdm Wong would be SGD 713.07 despite the heavy subsidies of almost 90% of her healthcare bill. Without subsidies, Mdm Wong would have to spend almost 70% of her annuity each month and SGD 5,372.68 annually on healthcare alone, excluding travel expenses and other indirect costs. The annual economic burden borne by the healthcare system is estimated to be SGD 15,148 per patient with multimorbidity in Singapore, with healthcare costs and social care costs increasing by SGD 2,265 and SGD 3,177, respectively, with each additional chronic condition.(29) Significant increases in healthcare utilisation and costs among patients with multimorbidity have been consistently demonstrated. According to a systematic review by Lehnert et al in 2011, total healthcare expenditures rose almost exponentially with the number of chronic conditions in several studies.(2) Healthcare costs were up to 5.5 times higher in patients with multimorbidity compared to those with none or only one chronic condition, and each additional chronic condition was associated with increased costs of USD 2,382 per year.(1)
Chronic conditions represent a lifetime burden that impact not only health services, but also patients and their caregivers who work to incorporate the increasingly complex treatment regimens into their daily lives.(10) Patients are significantly affected when they have to constantly juggle the demands of managing chronic conditions with other family, social and personal demands.(30) The healthcare workload is balanced against the patient’s capacity to manage their own health.(31) When the healthcare workload exceeds the patient’s capacity, they become overwhelmed by both the illness and treatment burden. Poor adherence, wasted resources and poor clinical outcomes ensue.(10) A patient-centred approach focuses on achieving patients’ targets for life and health while imposing the minimal potential treatment burden on their lives(32) with an empathic and feasible treatment plan.(33) Clinicians must continuously consider whether what is ‘asked of’ patients is achieving their goals or those of the health system.(34)
In our study, all six CPGs include patients’ goals and preferences. While many have advocated for personalised care, there is limited evidence on the best practices to achieve this.(11) One obvious barrier is the lack of information to aid clinical decisions, such as comparable information about the relative risks and benefits of different treatments. Future CPGs would need to incorporate the risks and benefits of prioritisation of care for each patient, while clinicians are trained to apply these principles.(35) One approach to personalise recommendations is to report a ‘payoff time’, the time over which patients must comply with treatment to achieve the proposed benefit.(36) For example, for a patient with diabetes mellitus and limited life expectancy who has difficulty achieving glycaemic targets on oral hypoglycaemic agents, the payoff time for preventing long-term complications using insulin should be balanced against the risk of hypoglycaemia and burden of regular blood glucose monitoring.(37) This helps to identify patients who may not benefit from recommendations that have immediate risks and delayed benefits.(36) If the payoff time is longer than the patient’s life expectancy, a shared decision to remove a prescribed treatment can decrease treatment burden and improve patient-centred care.(37)
In our study, we found that there were a limited number of recommendations for older adults based on the highest level of evidence, and no recommendations for patients with multimorbidity. Currently, there is insufficient published evidence to guide clinicians in managing older adults with multimorbidity or supporting their preferences, as older adults are systematically excluded from clinical trials(38) despite having the highest prevalence of multimorbidity. In future trials, older adults should be included and shared decision-making between patients and clinicians investigated in order to close this gap.(39)
We found that although most CPGs address the increased risk of drug interactions and adverse effects in older adults, none elaborated further on common or high-risk interactions. Furthermore, although the hypertension CPG has an extensive list of comorbidities, most are suggested as ‘compelling indications’ for specific medications, with no elaboration. While elaborating in CPGs to address all situations is unrealistic, their generalisability can be improved. CPGs should be cross-referenced explicitly to identify and demonstrate how to streamline synergistic recommendations and reconcile contradictory ones.(13) Most importantly, future CPGs should move from a single-disease focus to a patient-centred approach. For example, the United Kingdom (UK) NICE guideline for multimorbidity explicitly recommends establishing the disease and treatment burden alongside patient preferences.(40)
Our study has several strengths. First, we identified local CPGs and used available time and cost data norms whenever possible to contextualise the treatment burden in a local setting. Secondly, we used median time norms to calculate time spent, which is more meaningful for data that is not normally distributed, compared to the use of mean values in previous studies.(12)
The present study also has some limitations. The full range of treatment burdens was not considered. Our hypothetical patient did not present with any disease exacerbations or acute intercurrent illnesses. Furthermore, we excluded recommendations that were not found in the six CPGs we adopted, such as age-appropriate cancer screening or vaccinations as well as the psychosocial aspects of her disease and treatment burden experienced. Therefore, the treatment burden we tabulated would not be realistic if Mdm Wong were to exist in real life.
In conclusion, current single-disease CPGs inadequately address the patient-centred care approach for older adults with multimorbidity. When applied cumulatively, they create an overwhelming treatment burden. Therefore, patients’ goals and preferences must guide prioritisation of care such that treatment burden remains minimally disruptive to their lives. Developing future CPGs to deliver patient-centred rather than disease-focused care will be crucial to the management of multimorbidity.
ACKNOWLEDGEMENTS
This research was supported by the Singapore Ministry of Health’s National Medical Research Council under the Centre Grant Programme (reference no. CGAug16C019).
References Bähler C, Huber CA, Brüngger B, Reich O.Multimorbidity, health care utilization and costs in an elderly community-dwelling population:a claims data based observational study.BMC Health Serv Res. 2015;15:23. Lehnert T, Heider D, Leicht H, et al. Review:health care utilization and costs of elderly persons with multiple chronic conditions.Med Care Res Rev. 2011;68:387-420. Salisbury C, Johnson L, Purdy S, Valderas JM, Montgomery AA.Epidemiology and impact of multimorbidity in primary care:a retrospective cohort study.Br J Gen Pract. 2011;61:e12-21. Mercer SW, Salisbury C, Fortin M. ABC of Multimorbidity (ABC Series). 2014;1st edUK John Wiley & Sons Ltd. Guthrie B, Payne K, Alderson P, McMurdo ME, Mercer SW.Adapting clinical guidelines to take account of multimorbidity.BMJ. 2012;345:e6341. Gallacher K, May CR, Montori VM, Mair FS.Understanding patients'experiences of treatment burden in chronic heart failure using normalization process theory.Ann Fam Med. 2011;9:235-43. Gijsen R, Hoeymans N, Schellevis FG, et al. Causes and consequences of comorbidity:a review.J Clin Epidemiol. 2001;54:661-74. Wolff JL, Starfield B, Anderson G.Prevalence, expenditures, and complications of multiple chronic conditions in the elderly.Arch Intern Med. 2002;162:2269-76. Ministry of Health SingaporeAgeing in Place in Singapore. Available at: http://www.gs.org.sg/sg50conference/pdf/s4-1.pdf. Accessed August 26 2019. May C, Montori VM, Mair FS.We need minimally disruptive medicine.BMJ. 2009;339:b2803. Boyd CM, Darer J, Boult C, et al. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases:implications for pay for performance.JAMA. 2005;294:716-24. Buffel du Vaure C, Ravaud P, Baron G, et al. Potential workload in applying clinical practice guidelines for patients with chronic conditions and multimorbidity: a systematic analysis.BMJ Open. 2016;6:e010119. Hughes LD, McMurdo ME, Guthrie B.Guidelines for people not for diseases:the challenges of applying UK clinical guidelines to people with multimorbidity.Age Ageing. 2013;42:62-9. CPF Advisory Panel, Central Provident Fund, Singapore. Chapter 2: The Retirement Payouts and Sums. Available at: https://services.mom.gov.sg/cpfpanel/media/recommendations/part1/Chapter%202_The%20Retirement%20Payouts%20and%20Sums.pdf. Accessed August 25, 2018. Ministry of Health, Singapore. Chronic Disease Management Programme. Handbook for Healthcare Professionals 2018. Available at: https://www. primarycarepages.sg/Documents/Practice%20Management/CDMP%20Handbook%20for%20Healthcare%20Professionals%202018.pdf. Accessed August 25, 2018. Ministry of Health, Singapore. MOH Clinical Practice Guidelines on Diabetes Mellitus. 2014;. Available at: https://www.moh.gov.sg/hpp/doctors/guidelines/GuidelineDetails/cpgmed_diabetes_mellitus. Accessed August 30, 2018. Ministry of Health, Singapore. MOH Clinical Practice Guidelines on Lipids. 2016;. Available at: https://www.moh.gov.sg/hpp/doctors/guidelines/GuidelineDetails/cpgmed_lipids. Accessed August 30, 2018. Ministry of Health, Singapore. MOH Clinical Practice Guidelines on Hypertension. 2017;. Available at: https://www.moh.gov.sg/hpp/doctors/guidelines/GuidelineDetails/cpgmed_hypertension. Accessed August 30, 2018. 2018 GINA Report, Global Strategy for Asthma Management and PreventionGlobal Initiative for Asthma [online]. Available at: https://ginasthma.org/gina-reports/. Accessed August 30, 2018. Ministry of Health, Singapore. MOH Clinical Practice Guidelines on Depression. 2012;. Available at: https://www.moh.gov.sg/docs/librariesprovider4/guidelines/depression-cpg_r14_final.pdf. Accessed August 30, 2018. National Clinical Guideline Centre (UK)Osteoarthritis: Care and Management in Adults. 2014;London National Institute for Health and Care Excellence (UK). Yen LE, McRae IS, Jowsey T, Bagheri N.Time spent on health related activity by older Australians with diabetes.J Diabetes Metab Disord. 2013;12:33. Safford MM, Russell L, Suh DC, Roman S, Pogach L.How much time do patients with diabetes spend on self-care?.J Am Board Fam Pract. 2005;18:262-70. Ministry of Finance, Singapore. Overview: Pioneer Generation Package. Available at: https://www.pioneers.sg/en-sg/Pages/Overview.aspx. Accessed September 15, 2018. Community Health Assist Scheme, Singapore. CHAS Subsidies. Available at: https://www.chas.sg/content.aspx?id=636. Accessed September 15, 2018. Mutasingwa DR, Ge H, Upshur RE.How applicable are clinical practice guidelines to elderly patients with comorbidities?.Can Fam Physician. 2011;57:e253-62. Maher RL, Hanlon J, Hajjar ER.Clinical consequences of polypharmacy in elderly.Expert Opin Drug Saf. 2014;13:57-65. Russell LB, Ibuka Y, Carr D.How much time do patients spend on outpatient visits?:the American time use survey.Patient. 2008;1:211-22. Picco L, Achilla E, Abdin E, et al. Economic burden of multimorbidity among older adults:impact on healthcare and societal costs.BMC Health Serv Res. 2016;16:173. Jeon YH, Jowsey T, Yen L, et al. Achieving a balanced life in the face of chronic illness.Aust J Prim Health. 2010;16:66-74. Shippee ND, Shah ND, May CR, Mair FS, Montori VM.Cumulative complexity:a functional, patient-centered model of patient complexity can improve research and practice.J Clin Epidemiol. 2012;65:1041-51. Leppin AL, Montori VM, Gionfriddo MR.Minimally disruptive medicine:a pragmatically comprehensive model for delivering care to patients with multiple chronic conditions.Healthcare (Basel). 2015;3:50-63. Boehmer KR, Gionfriddo MR, Rodriguez-Gutierrez R, et al. Patient capacity and constraints in the experience of chronic disease:a qualitative systematic review and thematic synthesis.BMC Fam Pract. 2016;17:127. Trevena L.Minimally disruptive medicine for patients with complex multimorbidity.Aust J Gen Pract. 2018;47:175-9. Garber AM.Evidence-based guidelines as a foundation for performance incentives.Health Aff (Millwood). 2005;24:174-9. Braithwaite RS, Fiellin D, Justice AC.The payoff time:a flexible framework to help clinicians decide when patients with comorbid disease are not likely to benefit from practice guidelines.Med Care. 2009;47:610-7. Wyatt KD, Stuart LM, Brito JP, et al. Out of context:clinical practice guidelines and patients with multiple chronic conditions:a systematic review.Med Care. 2014;52:Suppl 3S92-S100. McMurdo ME, Witham MD, Gillespie ND.Including older people in clinical research.BMJ. 2005;331:1036-7. Elwyn G, Edwards A, Britten N.What information do patients need about medicines? “Doing prescribing”: how doctors can be more effective.BMJ. 2003;327:864-7. The National Institute for Health and Care Excellence. Multimorbidity:clinical assessment and managementNICE guideline [NG56]. 2016;. Available at: https://www.nice.org.uk/guidance/ng56. Accessed September 5 2018.
REFERENCES:
1. Bähler C, Huber CA, Brüngger B, Reich O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: a claims data based observational study. BMC Health Serv Res 2015; 15:23. https://doi.org/10.1186/s12913-015-0698-2
PMid:25609174 PMCid:PMC4307623
2. Lehnert T, Heider D, Leicht H, et al. Review: health care utilization and costs of elderly persons with multiple chronic conditions. Med Care Res Rev 2011; 68:387-420. https://doi.org/10.1177/1077558711399580
PMid:21813576
3. Salisbury C, Johnson L, Purdy S, Valderas JM, Montgomery AA. Epidemiology and impact of multimorbidity in primary care: a retrospective cohort study. Br J Gen Pract 2011; 61:e12-21. https://doi.org/10.3399/bjgp11X548929
PMid:21401985 PMCid:PMC3020068
4. Mercer SW, Salisbury C, Fortin M. ABC of Multimorbidity (ABC Series). 1st ed. UK: John Wiley & Sons Ltd, 2014.
5. Guthrie B, Payne K, Alderson P, McMurdo ME, Mercer SW. Adapting clinical guidelines to take account of multimorbidity. BMJ 2012; 345:e6341. https://doi.org/10.1136/bmj.e6341
PMid:23036829
6. Gallacher K, May CR, Montori VM, Mair FS. Understanding patients' experiences of treatment burden in chronic heart failure using normalization process theory. Ann Fam Med 2011; 9:235-43. https://doi.org/10.1370/afm.1249
PMid:21555751 PMCid:PMC3090432
8. Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med 2002; 162:2269-76. https://doi.org/10.1001/archinte.162.20.2269
PMid:12418941
10. May C, Montori VM, Mair FS. We need minimally disruptive medicine. BMJ 2009; 339:b2803. https://doi.org/10.1136/bmj.b2803
PMid:19671932
11. Boyd CM, Darer J, Boult C, et al. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance. JAMA 2005; 294:716-24. https://doi.org/10.1001/jama.294.6.716
PMid:16091574
12. Buffel du Vaure C, Ravaud P, Baron G, et al. Potential workload in applying clinical practice guidelines for patients with chronic conditions and multimorbidity: a systematic analysis. BMJ Open 2016; 6:e010119. https://doi.org/10.1136/bmjopen-2015-010119
PMid:27006342 PMCid:PMC4809109
13. Hughes LD, McMurdo ME, Guthrie B. Guidelines for people not for diseases: the challenges of applying UK clinical guidelines to people with multimorbidity. Age Ageing 2013; 42:62-9. https://doi.org/10.1093/ageing/afs100
PMid:22910303
19. 2018 GINA Report, Global Strategy for Asthma Management and Prevention. In: Global Initiative for Asthma [online]. Available at: https://ginasthma.org/gina-reports/. Accessed August 30, 2018.
21. National Clinical Guideline Centre (UK). Osteoarthritis: Care and Management in Adults. London: National Institute for Health and Care Excellence (UK); 2014.
22. Yen LE, McRae IS, Jowsey T, Bagheri N. Time spent on health related activity by older Australians with diabetes. J Diabetes Metab Disord 2013; 12:33. https://doi.org/10.1186/2251-6581-12-33
PMid:23815873 PMCid:PMC3704325
23. Safford MM, Russell L, Suh DC, Roman S, Pogach L. How much time do patients with diabetes spend on self-care? J Am Board Fam Pract 2005; 18:262-70. https://doi.org/10.3122/jabfm.18.4.262
PMid:15994472
26. Mutasingwa DR, Ge H, Upshur RE. How applicable are clinical practice guidelines to elderly patients with comorbidities? Can Fam Physician 2011; 57:e253-62.
27. Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf 2014; 13:57-65. https://doi.org/10.1517/14740338.2013.827660
PMid:24073682 PMCid:PMC3864987
28. Russell LB, Ibuka Y, Carr D. How much time do patients spend on outpatient visits?: the American time use survey. Patient 2008; 1:211-22. https://doi.org/10.2165/1312067-200801030-00008
PMid:22272927
29. Picco L, Achilla E, Abdin E, et al. Economic burden of multimorbidity among older adults: impact on healthcare and societal costs. BMC Health Serv Res 2016; 16:173. https://doi.org/10.1186/s12913-016-1421-7
PMid:27160080 PMCid:PMC4862090
30. Jeon YH, Jowsey T, Yen L, et al. Achieving a balanced life in the face of chronic illness. Aust J Prim Health 2010; 16:66-74. https://doi.org/10.1071/PY09039
PMid:21133301
31. Shippee ND, Shah ND, May CR, Mair FS, Montori VM. Cumulative complexity: a functional, patient-centered model of patient complexity can improve research and practice. J Clin Epidemiol 2012; 65:1041-51. https://doi.org/10.1016/j.jclinepi.2012.05.005
PMid:22910536
32. Leppin AL, Montori VM, Gionfriddo MR. Minimally disruptive medicine: a pragmatically comprehensive model for delivering care to patients with multiple chronic conditions. Healthcare (Basel) 2015; 3:50-63. https://doi.org/10.3390/healthcare3010050
PMid:27417747 PMCid:PMC4934523
33. Boehmer KR, Gionfriddo MR, Rodriguez-Gutierrez R, et al. Patient capacity and constraints in the experience of chronic disease: a qualitative systematic review and thematic synthesis. BMC Fam Pract 2016; 17:127. https://doi.org/10.1186/s12875-016-0525-9
PMid:27585439 PMCid:PMC5009523
34. Trevena L. Minimally disruptive medicine for patients with complex multimorbidity. Aust J Gen Pract 2018; 47:175-9. https://doi.org/10.31128/AFP-10-17-4374
PMid:29621856
35. Garber AM. Evidence-based guidelines as a foundation for performance incentives. Health Aff (Millwood) 2005; 24:174-9. https://doi.org/10.1377/hlthaff.24.1.174
PMid:15647228
36. Braithwaite RS, Fiellin D, Justice AC. The payoff time: a flexible framework to help clinicians decide when patients with comorbid disease are not likely to benefit from practice guidelines. Med Care 2009; 47:610-7. https://doi.org/10.1097/MLR.0b013e31819748d5
PMid:19433991 PMCid:PMC3077952
37. Wyatt KD, Stuart LM, Brito JP, et al. Out of context: clinical practice guidelines and patients with multiple chronic conditions: a systematic review. Med Care 2014; 52 Suppl 3:S92-S100. https://doi.org/10.1097/MLR.0b013e3182a51b3d
PMid:23969592
38. McMurdo ME, Witham MD, Gillespie ND. Including older people in clinical research. BMJ 2005; 331:1036-7. https://doi.org/10.1136/bmj.331.7524.1036
PMid:16269472 PMCid:PMC1283170
39. Elwyn G, Edwards A, Britten N. What information do patients need about medicines? "Doing prescribing": how doctors can be more effective. BMJ 2003; 327:864-7. https://doi.org/10.1136/bmj.327.7419.864
PMid:14551110 PMCid:PMC214051
40. The National Institute for Health and Care Excellence. Multimorbidity: clinical assessment and management. NICE guideline [NG56]. 2016. Available at: https://www.nice.org.uk/guidance/ng56. Accessed September 5, 2018.