

INTRODUCTION
The conventional pelvic radiograph remains the primary imaging modality for the assessment of osseous structures related to the pelvic girdle and hips in both adult and paediatric populations. Other more dedicated pelvic radiograph projections are often only performed for problem solving and usually requested by specialist orthopaedic surgeons. The overlapping and complex configuration of pelvic anatomic structures form the bases of the lines, arcs and stripes concept in assessment of pelvic radiographs. This pictorial essay reviews pertinent reference guides that are utilised for reporting plain radiographs of the pelvis and demonstrates various pathologies that distort their appearance.
Some of the reference guides are used for age-specific populations, some for symptom-specific scenarios and some for problem solving. For example, when assessing for the presence of a fracture in an elderly patient, one should not reference the line of Klein, which is used for evaluating the presence of slipped upper femoral epiphysis (SUFE) on a pelvic radiograph. By correctly utilising these reference guides, very subtle abnormalities may be detected and further appropriate imaging and treatment can be initiated. This may aid in early detection of potentially debilitating abnormalities, particularly in relation to paediatric hip pathology, and help prevent long-term adverse sequelae. Understanding pelvic anatomy and utilising the pelvic reference lines, arcs and stripes are therefore useful and can translate to better patient care.
ANATOMY
The bony pelvis consists of the sacrum, coccyx and a pair of innominate bones. The innominate bones are formed from three separate bones – the pubis, ilium and ischium. In childhood, they are joined by the triradiate cartilage that unites at puberty to compose the acetabulum, which articulates with the proximal femur at the hip joint.
There are four articulations within the pelvis, excluding the hips: the bilateral sacroiliac joints, which join the ilia and sacrum; the pubic symphysis, which joins the two pubic bones; and the sacrococcygeal joint or symphysis, between the sacrum and coccyx.
LINES, ARCS AND STRIPES
Numerous lines, arcs and stripes make up the pelvic radiograph (Figs.
Fig. 1
Pelvic radiograph shows the iliopectineal line (thick black dashed line); ilioischial line (thick white dashed line); sacral arcuate lines (three thick black curves); Shenton arc (arrowheads); line of Klein (thin straight white line); gluteal fat stripe (white asterisks); acetabular roof (thin white curve); medial acetabular wall (black asterisks); anterior acetabular wall (black dots); posterior acetabular wall (white dots); and femoral head line (thin black curve).
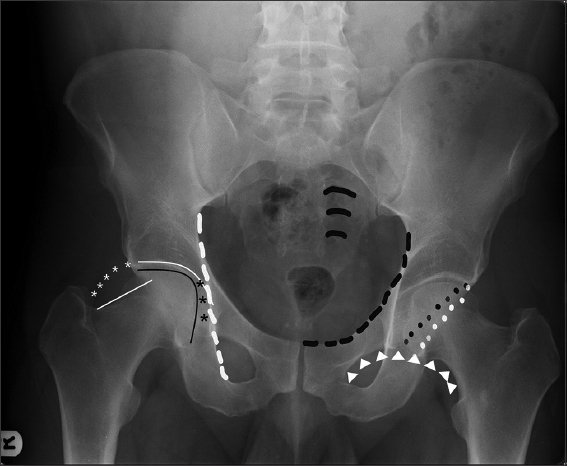
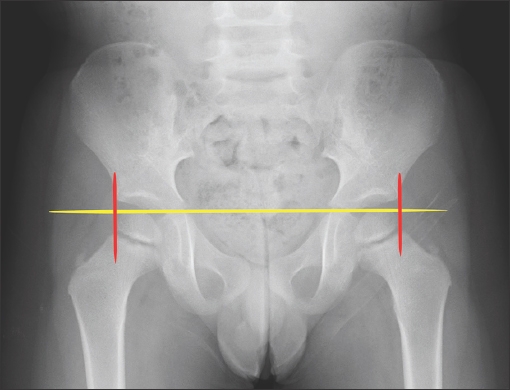
Fig. 2
Pelvic radiograph shows Hilgenreiner’s line (horizontal line) and Perkin’s line (vertical lines). The upper femoral epiphysis should be below Hilgenreiner’s line and medial to Perkin’s line in the inferomedial quadrant.
Other notable features
The acetabular roof is the superior weight-bearing area of the acetabulum, which includes a portion of both the anterior and posterior columns. Flattening of the acetabular roof occurs in achondroplasia.
The medial acetabular wall is normally lateral to the ilioischial line. The anterior acetabular wall is the anterior acetabulum rim, which runs medial in relation to the posterior acetabular wall. The posterior acetabular wall is the posterior acetabular rim, which runs lateral to the anterior wall. These two lines should never cross.
The femoral head line should be round and smooth, other than for the smooth divet, which represents the fovea.
SPECTRUM OF DISEASES
Trauma
Injuries to the pelvis and hip detected by radiography are either fractures or dislocations. The aforementioned lines can be utilised to ascertain the anatomic bony structures that are affected in pelvic injuries.
Pelvic fractures
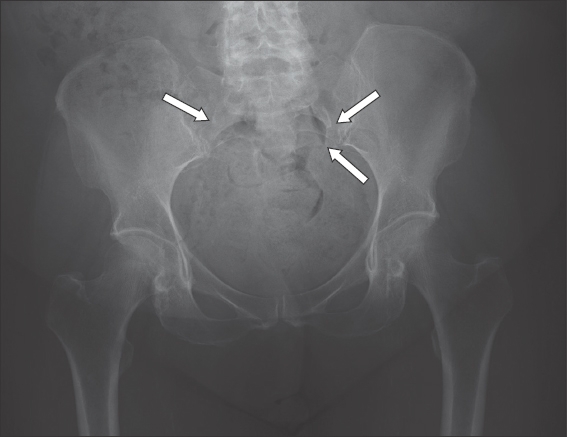
Pelvic fractures can be simple or complex, and involve any part of the bony pelvis. Unstable fractures of the pelvis in high-energy trauma are classified based on the mechanism of injury: lateral compression (
Fig. 3
Pelvic radiograph shows lateral compression injuries. A laterally directed force causes inward rotation of the left hemipelvis with left superior and inferior pubic rami fractures (white arrows). Posteriorly, an impaction fracture of the ipsilateral sacral ala can be seen, with disruption of the sacral arcuate lines (black arrows). The asterisk (*) indicates that there is an abnormality on the radiograph, which is part of the red dot system or radiographer abnormality detection system in our institution.
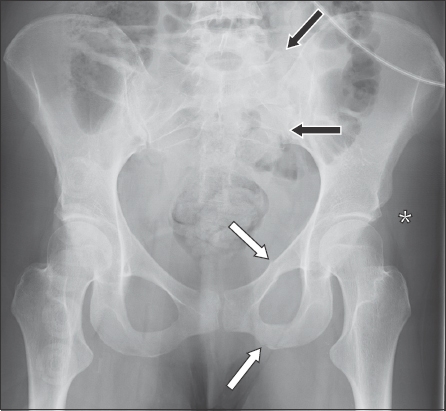
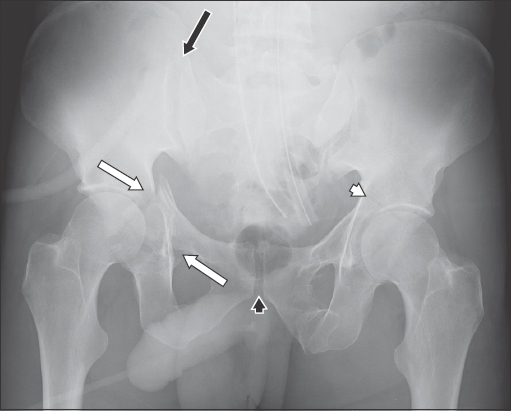
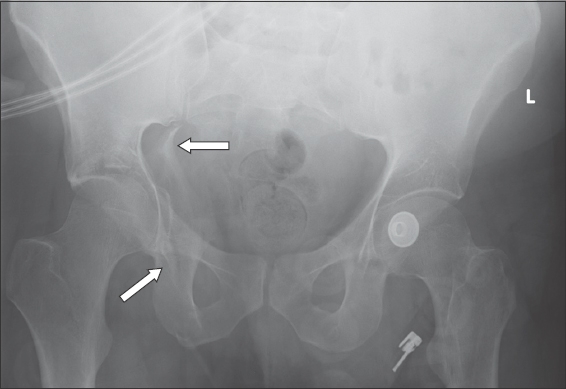
Fig. 4
Pelvic radiograph shows complex pelvic fractures with posterior and anterior columns fractures of the right acetabulum, and disruption of the right ilioischial and iliopectineal lines (white arrows); and anterior left acetabular column fracture with discontinuity of the left iliopectineal line (white arrowhead). There is widening of the right sacroiliac joint (black arrow) and minor widening of the pubic symphysis (black arrowhead).
Acetabular fractures
The Judet and Letournel classification is a commonly used classification system for acetabular fractures. It describes the five elementary patterns of acetabular fractures as: anterior wall, anterior column (which commonly disrupts the iliopectineal line, as seen in Figs.
Fig. 5
Pelvic radiograph shows disrupted iliopectineal lines on both sides, indicating anterior column fractures of the bilateral acetabula (arrows).
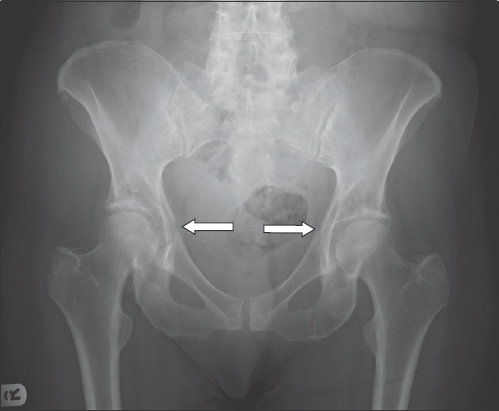
Fig. 6
Pelvic radiograph shows discontinuity of the right ilioischial line (arrows) suggestive of posterior acetabular fracture.
Femoral neck fractures
Femoral neck fractures are common injuries sustained by older patients from falls or younger patients from significant trauma.
Radiographic features for femoral neck fracture include disruption of the Shenton line (
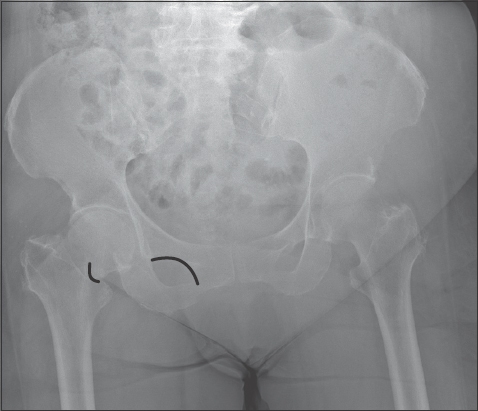
Fig. 7
Pelvic radiograph shows a right femoral neck fracture with disruption (black lines) of the Shenton arc or line.
Avulsion injuries
An avulsion injury of the pelvis occurs when an osseous fragment is pulled from its donor bone by forceful contraction of a tendon. This injury is more common in younger individuals.
Radiographic features include the presence of an avulsed bony fragment immediately adjacent to the donor bone in anatomically predictable locations that allude to the tendon attachment responsible for the injury, such as a pubic crest avulsion at the rectus abdominis-aponeurosis attachment disrupting the iliopectineal line (
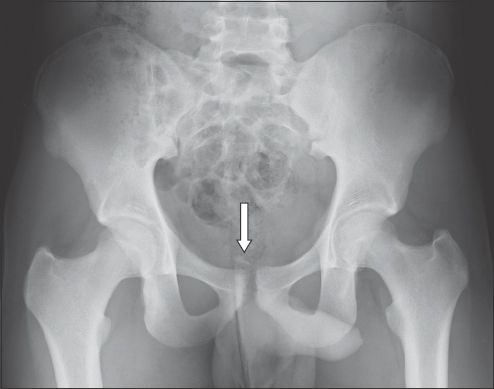
Fig. 8
Pelvic radiograph shows an avulsion fracture of the right pubic crest (arrow), the insertion site of the rectus abdominis muscles, which shows disruption of the iliopectineal line.
Insufficiency fractures
Insufficiency fractures are caused by normal stresses on abnormal bone. Common locations in the pelvis are the sacrum and pubic rami. The radiographic features are vertical fractures through the sacral ala (
Fig. 9
Pelvic radiograph shows bilateral sacral insufficiency fractures with disruption of bilateral sacral arcuate lines (arrows) in the absence of significant injury.
Slipped upper femoral epiphysis
SUFE represents a Type 1 Salter-Harris fracture, resulting in posteromedial slippage of the femoral head. It is most common in adolescents, and boys are more commonly affected.(7) Risk factors include obesity and endocrine disorders such as hypothyroidism, hyperparathyroidism and renal osteodystrophy.
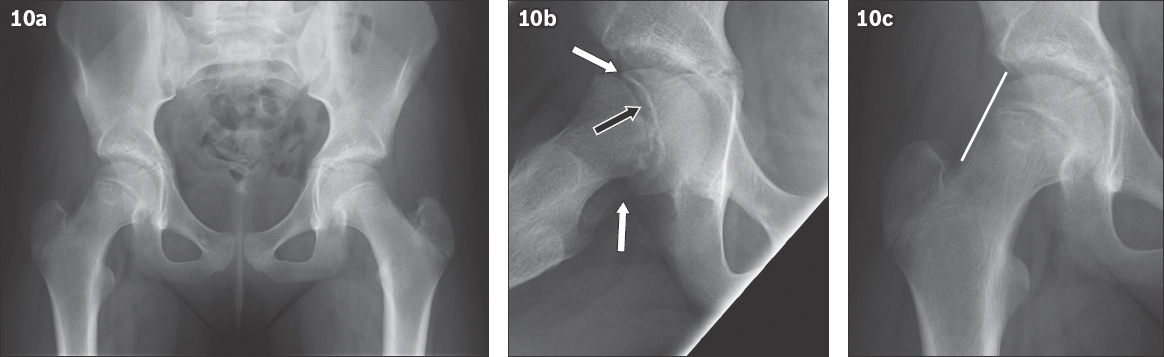
SUFE can be evaluated on the anteroposterior view of the pelvis (
Fig. 10
(a) Anteroposterior pelvic radiograph shows slipped upper femoral epiphysis on the right. (b) Frog-leg lateral radiograph confirms slipped upper femoral epiphysis with widening of the physis (black arrow), with the direction of the slippage shown (white arrows). (c) Radiograph shows that the line of Klein (white line) running along the lateral margin of the femoral neck does not cross the femoral head epiphysis.
Congenital/inherited
Developmental dysplasia of the hip
This aberrant development of the hip joint is typically diagnosed in the neonatal period by clinical examination and then usually confirmed with ultrasonography. Radiography can be used for assessment after substantial ossification has occurred.
Radiographic features include delay in ossification, the upper femoral epiphysis being displaced from the inferomedial quadrant (based on Hilgenreiner and Perkin’s lines;
Fig. 11
Pelvic radiograph shows developmental dysplasia of the hip on the left where the femoral epiphysis (white asterisk) lies in the superolateral quadrant (lateral to Perkin’s line, black; and above Hilgenreiner’s line, white). It should normally be in the inferomedial quadrant (black asterisk).
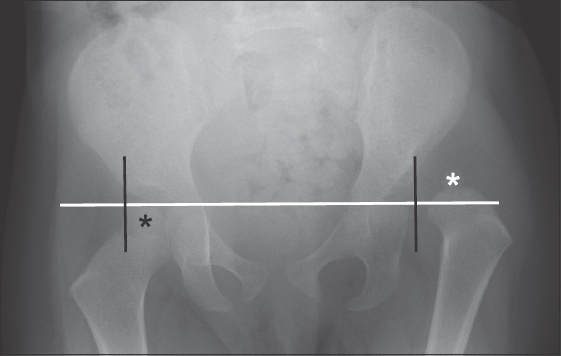
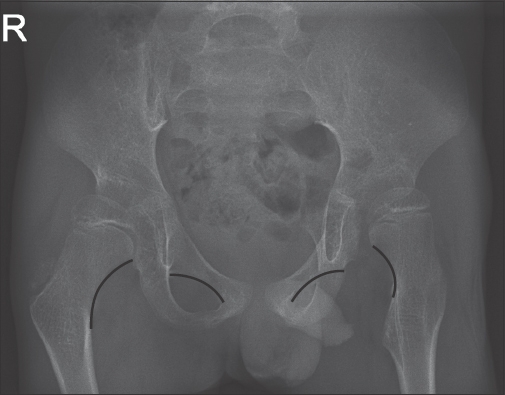
Fig. 12
Pelvic radiograph shows bilateral dysplastic hips with disruption of the Shenton arcs (black lines).
Femoroacetabular impingement
Femoroacetabular impingement occurs due to certain abnormal morphology at the femoral head-neck junction or acetabulum, resulting in impingement of the labrum or surrounding musculotendinous structures. There are two types: the ‘cam’ type, which is focal bone infilling/prominence at the anterior femoral head-neck region, giving a pistol grip deformity (
Fig. 13
Pelvic radiographs show focal bony prominence at the lateral aspect of the femoral head-neck regions compatible with cam lesions (arrows).
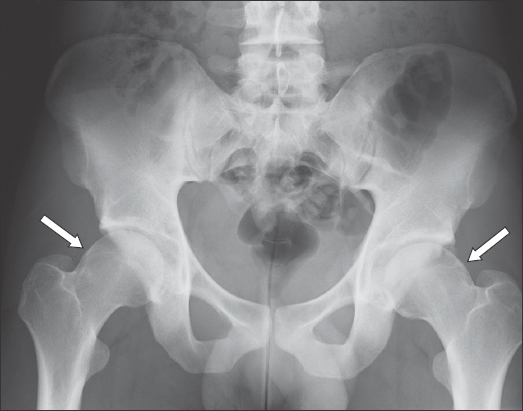
Fig. 14
(a & b) Pelvic radiographs show an example of bilateral acetabular retroversion. The crossover sign is seen in (b), where the posterior wall (black line) of the acetabulum is seen to cross over and project medial to the anterior wall (white line) of the acetabulum.
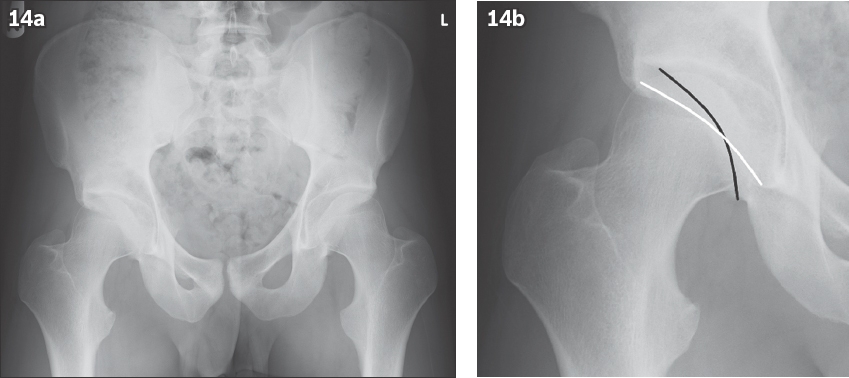
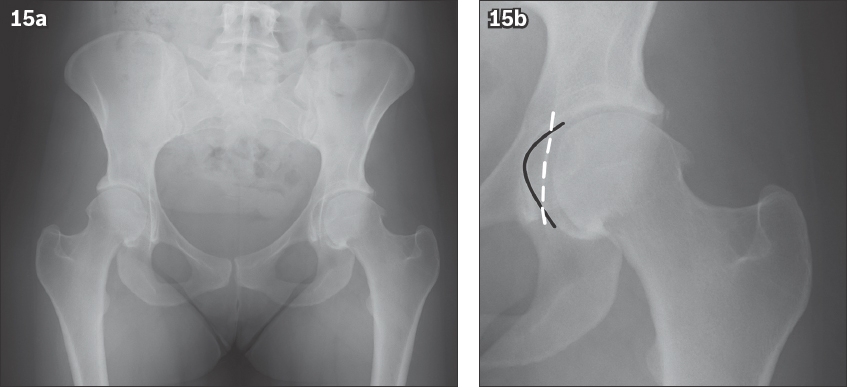
Fig. 15
(a & b) Pelvic radiographs show an example of bilateral osteoarthritic hips with coxa profunda. In (b), the medial acetabular wall (black line) projects medial to the ilioischial line (white dashed line).
Achondroplasia
Achondroplasia is the commonest form of short-limbed dwarfism, which can be inherited as an autosomal dominant or sporadic gene mutation and affects endochondral ossification.(11) Radiographic features (
Fig. 16
Pelvic radiograph shows the characteristic findings of achondroplasia: the roof of acetabula appears flat, the greater sciatic notches are small and the femoral metaphyses are widened.

Infection
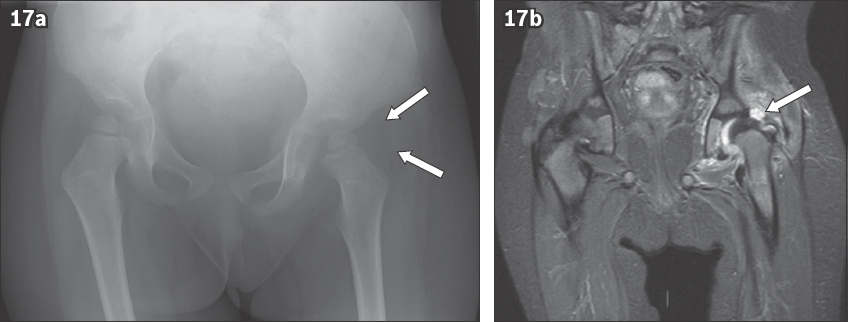
Septic arthritis is a destructive intra-articular infection, most commonly from pyogenic organisms, that usually affects the shoulder, hip and knee joints. Radiographic features include periarticular osteopenia, subchondral bone destruction and joint effusion (bulging of fat stripes) (
Fig. 17
A child with left hip joint effusion. (a) Pelvic radiograph shows the gluteal fat stripe bulging superiorly (arrows) due to the hip joint effusion. (b) Coronal MR short tau inversion recovery image of the pelvis shows the presence of the left hip effusion (arrow).
Tumour
Various malignant and benign tumours of the pelvis and proximal femur, which may present as lytic, sclerotic or mixed lytic-sclerotic lesions, can be identified on a pelvic radiograph. Careful review of the pelvic lines may aid in the detection of these lesions (
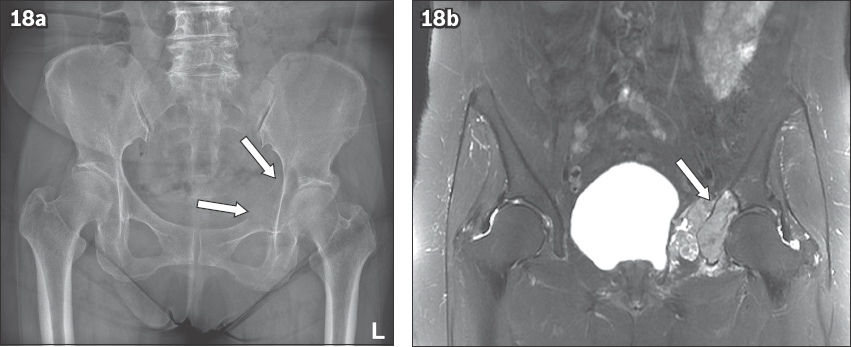
Fig. 18
(a) Pelvic radiograph shows a destructive lytic bone lesion (arrows) in the left acetabulum with discontinuity of the iliopectineal line. (b) Subsequent coronal MR short tau inversion recovery image of the pelvis shows soft tissue metastatic infiltrate causing bony destruction of the left acetabulum (arrow).
Metabolic
Legg-Calve-Perthes
Legg-Calve-Perthes disease is an idiopathic osteonecrosis of the femoral head. Osteonecrosis is the death of bone tissue caused by reduced blood flow. Radiographic appearances change with the stage of osteonecrosis. The radiographs are normal in the early stage, followed by osteopenia and patchy sclerosis. Collapse of the articular surface gradually occurs due to microfracture, with eventual bone fragmentation and degenerative change.
Legg-Calve-Perthes disease usually occurs in children aged 4–8 years, and is more common in males. Both hips are affected in 10% of cases.(13) Coxa magna, a large deformed femoral head, can be seen on radiographs in chronic cases due to overgrowth of articular cartilage (
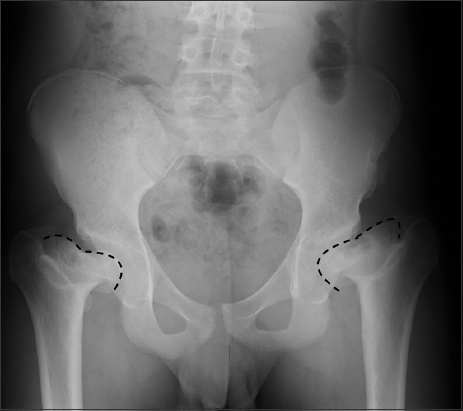
Fig. 19
Pelvic radiograph shows bilateral Legg-Calve-Perthes disease with collapse and flattening of the femoral heads (dashed black line), and widening of the femoral head and neck.
Miscellaneous
Protrusio acetabuli is characterised by deformity of the medial wall of the acetabulum with migration of the femoral head into the pelvic cavity, which sits at or medial to the ilioischial line. The centre of the femoral head is medial to the anterior and posterior walls of the acetabulum (
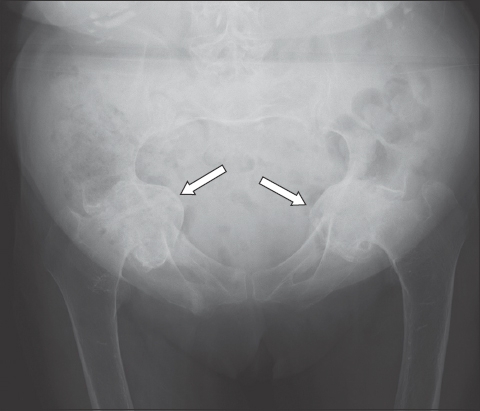
Fig. 20
Pelvic radiograph shows bilateral protrusio acetabuli (arrows) with medialisation of the medial wall of the acetabula and femoral heads lying medial to the ilioischial lines.
CONCLUSION
The pelvis has complex anatomic structures that form the basis of the lines, arcs and stripes concept in the assessment of pelvic radiographs. Having good knowledge of the pelvic anatomy and the spectrum of diseases is an important prerequisite for making an accurate diagnosis. Subtle but important findings on pelvic radiographs can be a challenge to identify. This notwithstanding, tracing the lines, arcs and stripes will be useful for detection of these imaging findings and in guiding diagnosis.
SMJ-62-340.pdf