

His mother took Tom, a one-year-old boy, to your clinic for a repeat consultation for persistent fever. Two days ago, he had presented with a three-day history of high fever and conjunctivitis. His mother mentioned that he had started attending a neighbourhood childcare centre one month before, and his teachers had said that a few of his classmates were down with flu. At that time, you prescribed antipyretics for viral fever and advised his mother to return if the fever persisted beyond Day 5 of the illness. During the repeat consultation, Tom’s mother reported that he had developed a rash two days ago, but it had mostly faded. She showed you a photo she had taken with her mobile phone of a generalised maculopapular rash. Tom was extremely fretful and refused to lie down on the couch, but you managed to examine him on his mother’s lap. On examination, his neck was supple, and a detailed head-to-toe examination revealed bilateral non-suppurative conjunctivitis, mild red lips and Bacille Calmette-Guérin vaccine site erythema. You were concerned that Tom had features of Kawasaki disease and referred him to a paediatric tertiary hospital for further evaluation.
WHAT IS KAWASAKI DISEASE?
Kawasaki disease (KD) is an acute, self-limiting febrile illness that predominantly affects young children below five years of age.(1) It is one of the most common vasculitis disorders of childhood and, if left untreated, is associated with development of coronary artery aneurysms (CAA). It is now the most common cause of acquired heart disease in children in developed countries.(2) The aetiology of KD remains unknown. A variety of infectious agents such as retrovirus, Epstein-Barr virus, coronavirus, staphylococcal and streptococcal superantigens, and unidentified virus particles have been postulated to trigger an immune activation, driving the inflammatory process.(3,4) To date, no single agent has been consistently identified.
HOW RELEVANT IS THIS TO MY PRACTICE?
Primary care physicians play a crucial role in the early diagnosis of KD, as they are often the first contact for patients. Many patients with KD initially present to primary care clinics for acute undifferentiated fever, and the attending doctor has the duty of diagnosing KD. Very often, the diagnosis is missed due to the mindset that KD is ‘rare’ and will not be seen in general practice. In reality, the incidence of KD is increasing, and the prevalence is higher among Asian populations. The incidence of KD in Singapore, estimated at 51.4 per 10,000 children aged below five years, is one of the highest outside Japan and very similar to that in Hong Kong and Taiwan.(5) KD results in CAA in up to one-third of untreated patients, and persistent aneurysms in 3%–5% of patients who receive treatment,(6,7) putting them at lifelong risk of thrombosis and myocardial ischaemia. Patients aged below six months or above five years are at increased risk for CAA. A recent study by Tulloh et al in the United Kingdom (UK) found that children with KD treated after Day 7 of illness were at significantly increased risk of serious heart damage, and this risk rose proportionately with further treatment delay.(8) Similarly, the American Academy of Paediatrics suggested that treatment should ideally be administered within the first seven days of illness and by Day 10 (as defined by the first day of fever) at the latest.(9) The American Heart Association (AHA) recommended that intravenous immunoglobulin (IVIG) should be instituted as early as possible, within the first ten days of illness of the onset of fever, as soon as the diagnosis can be established.(10) This further highlights the pivotal role of primary care providers in early diagnosis to ensure that patients receive prompt treatment for KD.
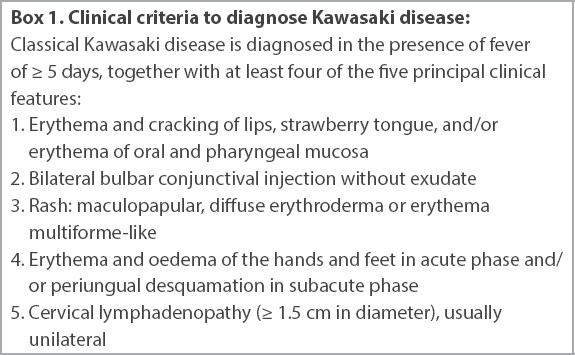
There is no single diagnostic test for KD. Clinical criteria recommended by the AHA are used to diagnose KD (
Box 1
Clinical criteria to diagnose Kawasaki disease:
Since April 2020, there have also been reports of COVID-19 infection with multi-systemic inflammatory syndrome that shares many characteristics with KD. This syndrome is now known as multi-system inflammatory syndrome in children (MIS-C). It was first reported by Riphagen et al in the UK in late April, with an unprecedented cluster of eight children with hyperinflammatory shock, showing features similar to KD.(12) By mid-May, the New York City Health Department detected 89 paediatric patients with symptoms consistent with MIS-C.(13) Locally, there have been no reported cases of MIS-C or KD linked to COVID-19 so far. The Ministry of Health in Singapore has urged for increased vigilance and referral of potential cases that present with clinical features suggestive of KD to tertiary paediatric hospitals for evaluation.
A high index of suspicion is required for the diagnosis of incomplete KD. Incomplete KD should be considered in any infant or child with prolonged unexplained fever and fewer than four of the principal clinical findings. In these cases, further laboratory investigations and echocardiography may be required to support the diagnosis of incomplete KD.
WHAT CAN I DO IN MY PRACTICE?
Acute undifferentiated fever in children is one of the most frequent presenting complaints in primary care. The common diagnosis is infection, with viral infections being more common than bacterial infections. The younger the child is, the higher the probability of serious bacterial infection. Febrile neonates and infants below three months of age are considered a separate high-risk group due to the risk of late-onset Group B streptococcal infection and should be referred to a tertiary paediatric hospital for further management. In a non-verbal child, it is important to conduct a head-to-toe physical examination, actively looking out for ‘hidden’ sources of infection such as meningitis, otitis media, pharyngitis, septic arthritis, osteomyelitis and urinary tract infection.
Other causes of acute fever include inflammatory or autoimmune causes such as KD and vaccine-related fever. However, vaccine-related fevers usually last less than 48 hours, and there should be a history of recent vaccination. Most benign, self-limiting viral infections do not cause a fever longer than 5–7 days. Fever of longer than five days’ duration should be investigated for bacterial infection or other diagnosis such as KD. Primary care physicians can form a ‘safety net’ to ensure that the diagnosis of KD is not missed by giving appropriate return advice to parents, such as in the event of persistent fever or clinical features suggestive of KD.
HOW DO I DIAGNOSE KAWASAKI DISEASE?
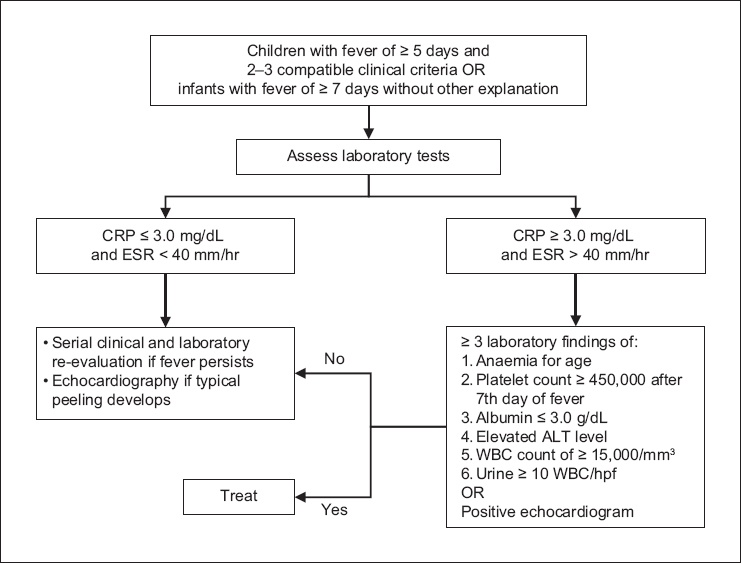
Patients with principal clinical findings that meet the case definition by the AHA are said to have classical or complete KD (
Fig. 1
Flowchart shows evaluation for suspected incomplete Kawasaki disease based on the American Heart Association Guidelines 2017. ALT: alanine aminotransferase; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; HPF: high-power field; WBC: white blood cell count
Some patients can also present with atypical clinical features such as renal impairment, neuritis, testicular swelling, pulmonary infiltrates and pleural effusions, diarrhoea, vomiting and abdominal pain, acute surgical abdomen, and haemophagocytic syndrome, which are not commonly seen in KD.
The course of KD can be described in three clinical phases: acute, subacute and convalescent. The acute phase lasts for 7–14 days and is characterised by fever and principal features of KD (
KD is a clinical diagnosis. Taking a detailed history and performing a detailed physical examination with index of suspicion is key in the evaluation of KD. It is also not uncommon for a child to have concomitant infection, such as KD and concurrent upper respiratory tract infection or urinary tract infection. The presence of a differential diagnosis such as infectious mononucleosis or scarlet fever is, very often, then used as evidence to exclude KD as a diagnosis. However, there has been increasing evidence that these infectious agents can act as a trigger for KD.(3,4) Therefore, it is important to bear in mind that the presence of an infectious agent does not exclude the diagnosis of KD.
Obtain history of fever and associated signs and symptoms
Fever of ≥ 3 days with at least three features of classical or complete KD, such as rash, conjunctival injection and lymphadenopathy, is sufficient to raise concerns of evolving KD. Signs and symptoms of KD can be transient, and a careful history may reveal that several principal features were present during the illness but resolved by the time of presentation. Not all clinical features present simultaneously. KD features may only start to appear after Day 5 of illness. Similarly, some of the features of KD may be present after fever has lysed without treatment. These groups of patients may still benefit from treatment if there are still signs of ongoing inflammation clinically or serologically. Thus, the presence of any of the five clinical features of KD at any time during the course of the illness should be documented and taken into consideration.
Examination findings
Specific signs to look for during an examination include: (1) polymorphous, non-vesicular, non-bullous rash; (2) bilateral painless, non-suppurative, limbic-sparing conjunctivitis; (3) erythema and cracking of lips, strawberry tongue, diffuse injection of oral and pharyngeal mucosa with no discrete lesions or ulceration; (4) significant cervical lymphadenopathy (> 1.5 cm) that is usually unilateral but can be bilateral; and (5) erythema and oedema of hands and feet (Figs.
Fig. 2
Photographs show the clinical features of Kawasaki disease: (a) erythema and cracking of lips with maculopapular rash on cheeks; (b) bilateral non-suppurative conjunctivitis; (c & d) hand and feet oedema with maculopapular rash on arms and legs; (e) desquamation of the fingertips; and (f) Bacille Calmette-Guérin site inflammation.

Differential diagnoses to consider
In patients with exudative conjunctivitis, exudative pharyngitis, ulcerative intraoral lesions, bullous or vesicular rash and generalised adenopathy, the infection – including Group A streptococcal infection, scarlet fever, Ebstein-Barr virus and adenovirus infection – needs to be identified and appropriately treated. Some of these differentials such as Group A streptococcal tonsillitis and scarlet fever can be treated with antibiotics on an outpatient basis; viral infections are usually self-limiting. However, if the fever persists for more than five days or the child does not improve after antibiotic treatment, early referral to the paediatrician is warranted to facilitate further investigations. In patients who present with fever and one or two non-specific features such as rashes, it is important to advise parents to return should the fever persist beyond five days or if the parents notice more features of KD. Other conditions that present in similar ways as KD include drug-related reactions such as Stevens-Johnson syndrome and autoimmune conditions such as systemic juvenile idiopathic arthritis.
WHAT SHOULD I DO IF I SUSPECT KD?
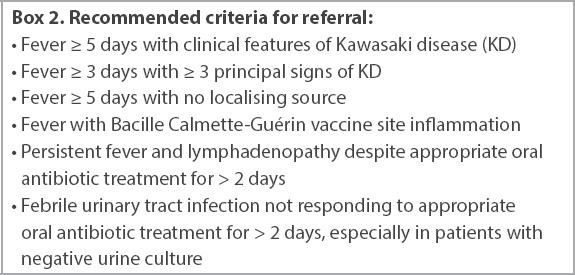
All patients with suspected KD warrant admission.
Box 2
Recommended criteria for referral:
COMMON PITFALLS
The diagnosis of KD can be easily missed if KD is not considered as a differential diagnosis, especially in patients with incomplete or atypical features. Prolonged fever and irritability may be the only clinical features of KD in an infant below six months of age. The presence of fever and pyuria in an infant or young child can be mistaken for a urinary tract infection, rash may be wrongly diagnosed as allergic rash or viral exanthem, and lymphadenopathy may be overlooked as infective lymphadenitis.
Children with recent KD
Some children may present at consultations for peeling of skin on the fingertips and toes. In such cases, provide reassurance to parents, as no treatment is necessary. Live vaccines should be delayed until at least 11 months after IVIG, as antibodies in IVIG may reduce the effectiveness of these vaccines. Additionally, up to 1%–3% of patients may have recurrence of KD after recovering from the first episode.
TAKE HOME MESSAGES
-
KD is one of the most common types of vasculitis in childhood, predominantly affecting young children aged below five years; if left untreated, it increases the risk of coronary aneurysms as sequelae.
-
KD is a clinical diagnosis made in the presence of fever of at least five days and at least four out of five clinical criteria as per the AHA’s recommendation (
Box 1). -
Patients with incomplete features should be further evaluated with blood and urine tests according to the AHA diagnostic algorithm (
Fig. 1) for incomplete KD. There should be a high index of suspicion for incomplete KD. -
BCG site inflammation and irritability, although not in the diagnostic criteria, are frequently encountered symptoms.
-
Differential diagnoses such as viral or bacterial infections, drug-related reactions and autoimmune disorders do not exclude KD. If fever persists despite adequate treatment, KD should be considered.
-
Early referral for workup for KD should be considered if any of the red flag symptoms are present (
Box 2). -
Live vaccinations should be deferred for at least 11 months following IVIG administration.
Four weeks later, Tom returned for another consultation. He was diagnosed with incomplete Kawasaki disease (KD) and was treated with intravenous immunoglobulin (IVIG) as an inpatient. He was kept on aspirin as his latest echocardiogram showed dilated coronary arteries. His mother was extremely anxious about the new-onset skin peeling on his fingertips and toes. There was no recurrence of fever. On examination, Tom appeared happy and well. You reassured his mother that peeling is a natural progression of KD and is usually self-limiting. You also took the opportunity to check Tom’s health booklet and advised his mother that he was due for his pneumococcal booster vaccine, even though his vaccine for mumps, measles and rubella should be delayed for 11 months after IVIG treatment. You also encouraged his mother to get him vaccinated with the latest influenza vaccine.
ACKNOWLEDGEMENTS
We would like to thank A/Prof Thaschawee Arkachaisri, Head and Senior Consultant, KK Women’s and Children’s Hospital, Rheumatology and Immunology Service, Singapore, for his contribution of clinical pictures and his support for this article.
SMJ-62-7.pdf