

Abstract
Most people spend a third of their lives sleeping, and thus, sleep has a major impact on all of us. As sleep is a function and not a structure, it is challenging to treat and prevent its complications. Sleep apnoea is one such complication, with serious and potentially life-threatening consequences. Local studies estimate that about 15% of Singapore’s population is afflicted with sleep apnoea. The resulting sleep fragmentation may result in poor quality of sleep, leading to daytime sleepiness. Sleep apnoea may also be the underlying cause of high blood pressure, memory loss, poor concentration and work performance, motor vehicle accidents, and marital problems. Evaluation involves a sleep study, followed by patient education, and an individualised step-wise management approach should be explored. Many patients will require follow-up for a long period of time, as management options may not offer a permanent cure; other contributory causes may arise at different phases of their lives, compounded by genetic and hormonal issues, ethnicity and the modern hazards of a fast-paced society.
You noticed that Mr George was not quite himself throughout his hypertension follow-up review. He finally shared that after an overseas golf trip, his friend had advised him to seek medical assessment for his loud snoring and ‘choking’ during sleep. He then quickly brushed the topic aside and mumbled that his friend was a light sleeper
HOW COMMON IS THIS IN MY PRACTICE?
What is sleep apnoea?
Sleep apnoea is a serious and potentially life-threatening condition where there is cessation of breathing that lasts 10 seconds or more during each session.
HOW RELEVANT IS THIS TO MY PRACTICE?
Local studies estimate that 15% of Singapore’s population are affected by sleep apnoea, and the prevalence of this condition may have increased with other health trends such as physical inactivity and obesity.(1) Sleep apnoea causes sleep fragmentation, which may result in poor quality of sleep, leading to daytime sleepiness. Sleep apnoea may also be the underlying cause of high blood pressure, memory loss, poor concentration and work performance, motor vehicle accidents and even marital problems.
WHAT CAN I DO IN MY PRACTICE?
There are at least three presentations in primary care when a thorough sleep history is useful: (a) when performing a patient’s health screening routine or examining a patient’s fitness for work; (b) when reviewing patients at high risk, including those with obesity, refractory hypertension, type 2 diabetes mellitus, congestive heart failure, atrial fibrillation and stroke; and (c) when evaluating symptoms related to sleep apnoea such as snoring or daytime sleepiness.
Asking about sleep
Most people spend a third of their lives sleeping, and thus, sleep has a major impact on all of us. As sleep is a function and not a structure, it is challenging to treat and prevent its complications. A sleep history should be taken from a patient with sleep apnoea as well as from the bed partner or roommate, and should include questions regarding snoring, witnessed instances of apnoea, gasping/choking episodes, and excessive sleepiness not explained by other factors. The patient’s sleep history should also include an assessment of sleepiness severity by the Epworth Sleepiness Scale,(2) total amount of sleep, nocturia, morning headaches, sleep fragmentation/sleep maintenance insomnia, and decreased concentration and memory. Further relevant questions may include secondary conditions precipitated by obstructive sleep apnoea (OSA), including hypertension, stroke, myocardial infarction, decreased daytime alertness and motor vehicle accidents.
Asking about snoring
Sleep apnoea is not well understood by the public and patients are less likely to bring up its symptoms, such as snoring, in the consultation room. Snoring is often regarded as a personal trait, rather than a medical condition; it may make the snorer an object of ridicule and cause the bed partner or roommate to develop sleepless nights and resentment.(1) Invitation to further elaborate on sleep behaviour and pattern may be necessary before patients voluntarily provide more information on this topic. Many in our local population can observe and describe the end part of each apnoea episode, which they often describe as ‘choking’, before the snoring restarts. It is thus important for the bed partner or roommate of a patient with sleep apnoea to observe any symptoms and to give specific lay descriptions of sleep apnoea at the patient’s follow-up consultations.
A possible symptom of OSA, snoring disturbs the sleep pattern, depriving the snorer of the appropriate rest. Snoring has also been strongly associated with many medical problems such as stroke and cerebrovascular diseases.(3) Snoring occurs in at least 10% of men aged under 30 years, and at least 60% of men aged over 60 years.(1) It also affects men twice as often as women.(1)
Physical examination
When conducting a physical examination, the clinician should document an upper airway assessment and look out for obesity, thick and short neck, receding chin, craniofacial deformities, adenotonsillar hypertrophy, deviated nasal septum, turbinate hypertrophy, crowded oropharynx and a bulky tongue.
Sleep study (polysomnography) and investigations
An overnight sleep study is needed for the evaluation of snoring and OSA. During the study, the patient’s electroencephalographic, electrooculographic, electromyographic and electrocardiographic activities, as well as leg movements, sleep position and respiratory efforts, are monitored via electrodes applied onto the scalp, face, chin, thorax, abdomen and legs. Sleep study can confirm the diagnosis and severity of OSA, but provides limited information on the anatomical levels or degree of upper airway obstruction. Diagnostic sleep study, continuous positive airway pressure titration study, multiple sleep latency test and maintenance wakefulness test are other specialised tests that are conducted in a sleep laboratory.
Sleep apnoea management
OSA is closely linked to the global issue of obesity, as well as problems with soft and skeletal tissues affecting the local upper airway. Thus, the challenge is to tailor each person’s treatment for OSA based on the individual’s situation and needs. Individualised evaluations such as flexible nasopharyngeal endoscopy assessment and videoendoscopic computer-assisted measurement(4,5) of the upper airway enable clinicians to better identify and quantify the sites of obstruction of the upper airway.
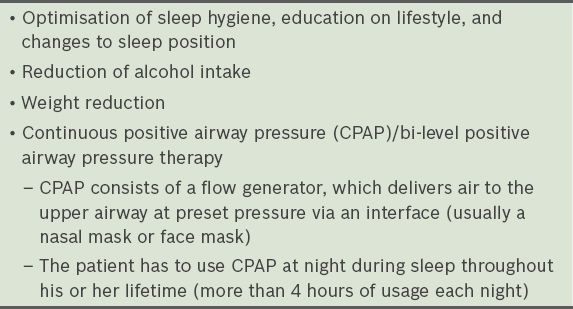
Snoring and sleep apnoea are often multifactorial conditions. Therefore, treatment varies from one patient to another, i.e. depending on the severity of their conditions, and their individual circumstances, needs and phases in life. There are many treatment options for OSA, and they are usually offered in a step-wise approach. Patient education and lifestyle changes are a combination of treatments that may sometimes be used (
Table I
Lifestyle and nonsurgical management options for sleep apnoea patients.
Many surgical interventions can help to relief upper airway obstruction, depending on the anatomical levels and degree of obstruction. These treatment options are individualised and offered after patient education, lifestyle modifications and nonsurgical management have been explored and rejected, or have failed. As sleep apnoea is often a multifactorial condition, management options that have worked well may not always lead to a permanent cure or an optimised state, as other contributory causes may arise at different phases of the patient’s life, compounded by genetic and hormonal issues, ethnicity and the modern hazards of a fast-paced society.
As some of these management options are offered by different clinical specialities and allied clinical experts, it is thus increasingly relevant and important to form integrated clinical teams to run sleep services or sleep centres. A step-wise management approach can then be seamlessly offered and tried, before tailored surgery is offered to relief physical obstruction or reconstruct the upper airway, depending on the individual’s assessment.
TAKE HOME MESSAGES
-
Sleep apnoea or obstructive sleep apnoea is estimated to affect 15% of Singapore’s population and is likely under-diagnosed.
-
Sleep apnoea has serious implications, such as sleep fragmentation and daytime sleepiness.
-
Sleep apnoea may be the underlying cause of high blood pressure, memory loss, poor concentration, poor work performance, motor vehicle accidents and even marital problems.
-
Snoring is not often brought to medical attention, as it is regarded as a personal trait and may make the snorer an object of ridicule if the issue discussed openly.
-
An overnight sleep study is required in order to confirm sleep apnoea and its severity.
-
There are many available management options for sleep apnoea, which are offered in a step-wise approach and individualised for each patient.
Mr George returned with his wife for his hypertension review. You read the memo by your ENT (Ear, Nose and Throat) Department colleague about the confirmed sleep apnoea. Mr George and his wife had attended education sessions on sleep apnoea and decided that they did not want to continue with continuous positive airway pressure therapy after their month-long trial. He was happy after his coblation procedure. His wife thanked you for helping to improve her sleep and reported that Mr George’s blood pressure had improved. You congratulated them and down-titrated Mr George’s hypertensive medications, based on readings from his home blood pressure diary