

Abstract
INTRODUCTION
Trampolining is a popular activity. However, to our knowledge, no studies on paediatric trampoline-related injuries (TRIs) have been conducted in Asia. We aimed to provide an Asian perspective on paediatric TRIs and evaluate current safety measures.
METHODS
Patients aged under 16 years who presented to the emergency department at KK Women’s and Children’s Hospital, Singapore, from March 2012 to June 2016 with a TRI were identified from the National Trauma Registry. Data was collated retrospectively focusing on age, location of the trampoline, mechanism and location of injury, treatment, disposition, and follow-up treatment.
RESULTS
137 children were seen for a TRI during this period. There was even representation across age groups (< 6 years, 6–11 years and 11–16 years). 60.6% of these injuries occurred in a public trampoline park, and a smaller proportion involved home and school trampolines. 61.3% of injuries occurred on the trampoline and 25.5% involved a fall off it, while the remaining were incurred by hitting the trampoline frame. The most common injury was soft tissue injury, followed by fractures and dislocations, of which 16.7% required surgical intervention. Most patients were discharged to an outpatient clinic. 14.6% of all patients required admission and 9.5% eventually required surgical intervention. There were three stable head injuries and no cervical spine injuries or deaths.
CONCLUSION
The existence of trampoline parks has contributed to a rise in TRIs. We recommend measures such as general education, changes in the setup around the trampoline, increasing the age limit for trampolining, adult supervision and discouraging double bouncing.
INTRODUCTION
Trampolining is a popular activity today; what started off as a competitive sport has become a well-received recreational activity among children and adults. Within the last five years, Singapore has seen more than five recreational trampoline parks open throughout the island. Most of these trampoline parks consist of a number of interconnected trampolines, surrounded by protective nets along its periphery. Other features of the trampoline park include foam pits, a parkour wall and a slam dunk zone. These parks also hold beginners’ trampoline classes for novice children. Trampoline parks have also become a popular location to hold events for children.(1-3)
Multiple studies have described an increase in the number of injuries among children as a result of trampoline-related activities. The National Electronic Injury Surveillance System sample described multiple cases of spinal cord injuries as well as a traumatic brain injury and two deaths at trampoline parks.(4-6) Several other studies also pointed out trampoline-related injuries (TRIs) as a significant cause of cervical spine injury, which can subsequently cause long-term neurological sequelae.(5,7-11)
The American Academy of Pediatrics published a study in 1977 recommending a ban on trampoline activities as part of physical education programmes in schools and that trampolining should be abolished as a competitive sport, only to review and soften their stance in the 1980s.(12-14) In response, the American Academy of Orthopaedic Surgeons recommended some safety measures that should be put in place when using the trampoline.(15)
This study aimed to provide an Asian perspective of paediatric TRIs by retrospectively reviewing the data of patients (aged 0–16 years) who presented to the emergency department (ED) in KK Women’s and Children’s Hospital (KKH), the largest children’s hospital in Singapore, for a TRI between 2012 and 2016. We focused on the types and mechanisms of injury, treatment required, and the morbidities and mortalities of the injury. In doing so, we aimed to evaluate the effectiveness of the safety measures in place and recommend further measures that should be reinforced.
METHODS
A single-centre retrospective study was conducted on all children under the age of 16 years who had presented to the ED of KKH for a TRI between March 2012 and June 2016. Approval was granted by the SingHealth Centralised Institutional Review Board. All data was obtained from the National Trauma Registry and all subjects who met the inclusion criteria were selected from the registry, regardless of whether they were on the trampoline for recreational or competitive purposes. Patients who presented with any other pre-existing comorbid condition (in addition to the TRI) that might affect their eventual disposition were excluded.
Data was collated focusing on these features: age group, whether the trampoline was part of a public trampoline park or a privately owned trampoline, the exact day and date of the injury, time of accident and presentation, cause of fall, mechanism of injury, part of body injured, type of injury, treatment in the ED, disposition, and follow-up treatment. All fractures were correlated with radiological findings.
Data was interpreted by a statistician using IBM SPSS Statistics version 23.0 (IBM Corp, Armonk, NY, USA). Descriptive data for categorical variables was presented as number of cases and percentages, while differences across groups were expressed using chi-square test or Fisher’s exact test, as appropriate. A p-value < 0.05 was considered statistically significant.
RESULTS
During the study period from March 2012 to June 2016, a total of 137 children presented to KKH for TRIs. Of these, 73 (53.3%) were female and 64 (46.7%) were male. 52 (38.0%), 49 (35.8%) and 36 (26.3%) of the patients were in the 6–11 years, 11–16 years and < 6 years age groups, respectively. 60.6% had injured themselves in a public trampoline park, 24.8% were injured through trampoline use in school and 14.6% had fallen while using a trampoline at home. The demographic profile of the patients is summarised in
Table I
Demographics of the patients (n = 137).
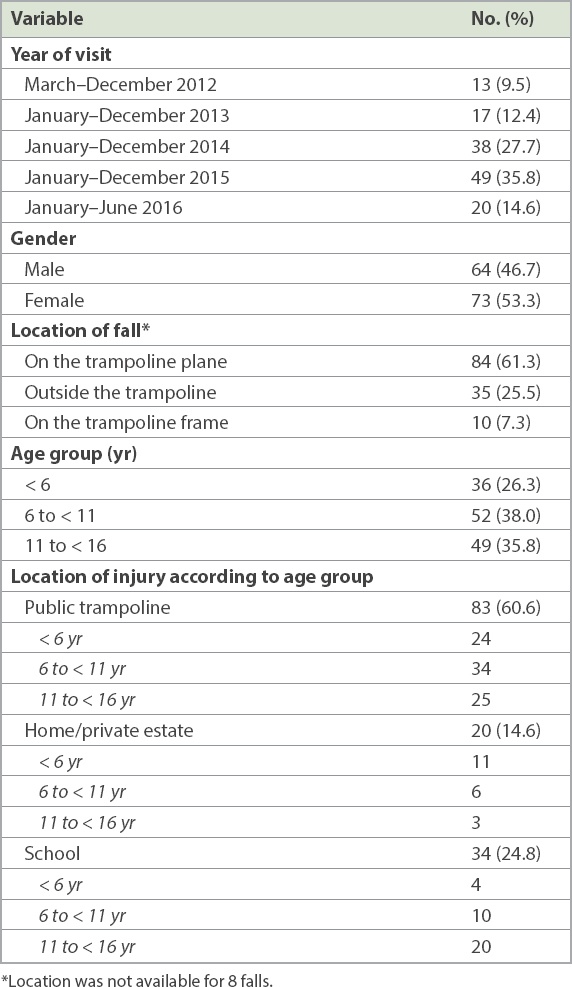
Most children had injured themselves directly through a failed landing while jumping on the trampoline, with 84 (61.3%) injuries being sustained on the trampoline plane. 35 (25.5%) injuries were sustained outside the trampoline and 10 (7.3%) by falling on the trampoline frame. Another 8 (5.8%) falls were not adequately classified. 7 (5.1%) children had accidentally collided against the trampoline frame while playing in the vicinity of the trampoline. In 10 (7.3%) of the trampoline injuries, another person was present and jumping concurrently with the child; 5 (50.0%) of these children lost balance and fell on or off the trampoline, while the other 5 (50.0%) were hit or stepped on by another person while they were jumping together.
The anatomical areas that were most commonly involved in the trampoline accidents were arms and legs, with a total of 110 (80.3%) injuries involving the limbs (
Table II
Distribution of injuries (n = 137).
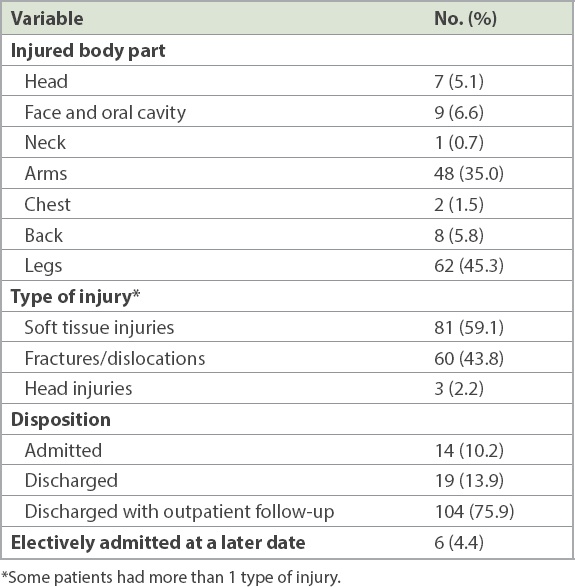
Fig. 1
Bar chart and table show the age range of the children and location of the injury.
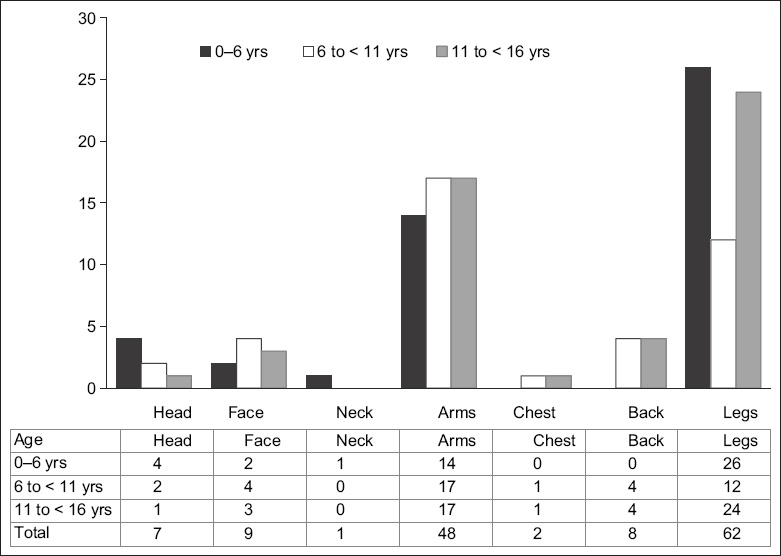
Table III
Types of injuries and their outcome according to the age of the patients.
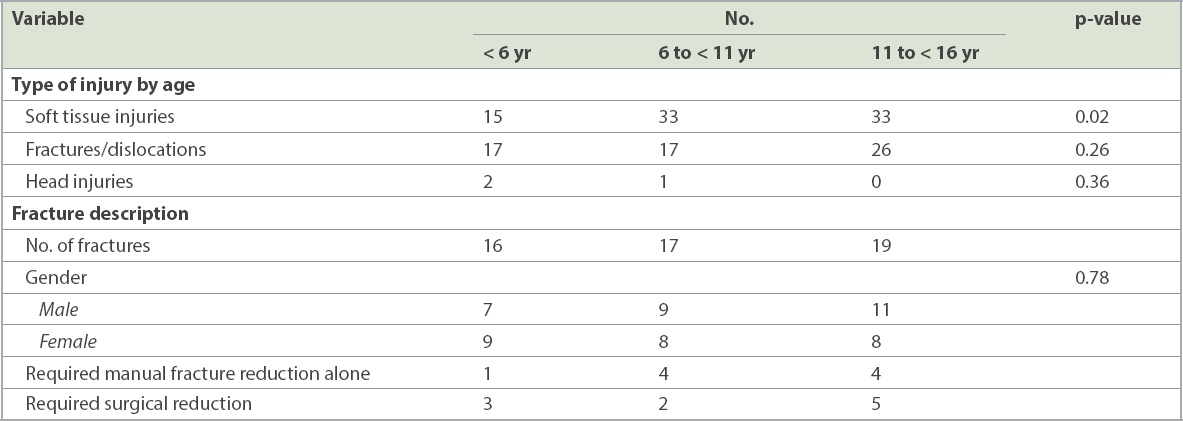
The incidence of fractures was highest in the 11–16 years age group, but this was not statistically significant (p = 0.26). The number of fractures was evenly distributed among all three age groups (
The majority of the patients (75.9%, n = 104) were discharged from the ED with outpatient follow-up, mostly to the orthopaedic surgery department. 19 (13.9%) patients did not require any form of follow-up, while 14 (10.2%) required inpatient admission for specialist care. 6 (4.4%) of the patients who were recommended for follow-up as outpatients were electively admitted for further treatment. Overall, 20 (14.6%) patients required inpatient admission and 13 (9.5%) patients eventually required surgical intervention.
DISCUSSION
Although the data only looked at ED visits over four years, there has been an apparent increase in the number of visits to the ED for TRIs, which may be related to the increase in prevalence of trampolines and trampoline parks in Singapore. Although most injuries were mild, close to 10% required surgical intervention.
The most common injuries sustained were soft tissue injuries followed by fractures, consistent with many other studies conducted.(6,7,16,17) Certain trends relating to age range and type of injury were also noted. While fractures appeared to be common across all three age groups, contusions and ligamentous strains were more common in those who were aged 6–16 years (
A significant proportion of those with fractures in our population (n = 19, 36.5%) required intervention either via manipulation and reduction in the ED or surgical reduction, while the majority were conservatively managed and discharged with no further complications. The majority of patients who had fractures requiring manual or surgical reduction were aged 11 years and above. Notably, 47.4% of those in this age range with a fracture required intervention (
While cervical spine injuries are a common cause of neurological sequelae and morbidity in TRIs in other studies,(5,8-11) only one neck injury, which was attributed to a muscular strain, presented to our ED. Of the three head injuries sustained in our population, two occurred in those below six years of age, and all three when the child fell off the trampoline: one was due to double bouncing, while the other two were unwitnessed falls. Head injuries tend to occur when a child falls off the trampoline.(19) All three patients with head injuries were admitted to the neurosurgical ward for monitoring, remained well and were discharged the following day. One of them had a concurrent uncomplicated laceration of the face requiring suturing.
This study has shown that the majority of the injuries were sustained when the child had a failed landing on the trampoline plane (n = 84) and relatively fewer injuries (n = 35) were a result of the child bouncing off the trampoline onto the ground outside the trampoline plane. Injuries that happened outside the trampoline plane tended to result in a head injury or a fall on an outstretched hand, resulting in an upper limb injury. While there were cases of children falling off the trampoline at public trampoline parks, most of these injuries occurred in a private setting – either in school, at home or in a residential estate. The data reviewed had insufficient information regarding the safety settings around the trampoline that each child was jumping on.
A significant proportion (n = 34, 24.8%) of injuries were sustained through the use of trampolines in schools. However, the greatest number of TRIs still occurred in public trampoline parks (n = 83, 60.6%), suggesting that the increase in popularity and accessibility to public trampoline parks in Singapore may indeed contribute to an increase in TRIs. Out of 20 admissions, only 2 (10%) had injuries sustained on a home trampoline.
A study conducted by Linakis et al on ED visits in the United States for paediatric TRIs concluded that the relatively inexpensive home trampoline has made home trampoline use very popular, and its use continues to be a significant source of childhood injury morbidity.(16) There are other studies conducted overseas in which the majority of TRIs were sustained on home trampolines.(4,17) However, this is not the case in Singapore, probably due to space constraints and the number of trampoline parks within a short distance of each other. Travelling to a public trampoline park may be much more convenient in Singapore.
Several studies have correspondingly identified that double bouncing, or having multiple users on a trampoline, was a significant cause of injury.(6,16,18,20-22) In this study, ten injuries were caused by multiple users being on the trampoline, resulting in the injured child either falling off the trampoline due to a heavier force on the trampoline or being involved in a collision. Consistent with the aforementioned studies, the injuries in which multiple users were on the trampoline happened more often in younger children, with six out of ten of them occurring in children aged below six years and none in the 11–16 years group. All the injuries from double bouncing were minor and did not require any long-term follow-up.
Several studies have evaluated the effectiveness of safety measures in trampoline use, and most reported that safety measures have minimal impact on the frequency of TRIs.(7,19,23-26) Ashby et al showed that a voluntary standard in Australia had little effect on spring and frame injuries, and none on multiple-user injuries.(24) Nysted and Drogset concluded that trampoline nets may not have helped to reduce TRIs at all.(7)
In Singapore, safety rules and features have been put in place in public trampoline parks. The safety nets surrounding the periphery of public trampolines may have served their purpose, as only a minority of falls off trampolines occurred in public trampoline parks. Another rule is that children aged below 18 years require a parent or guardian’s approval, and all children below four years need to be supervised by an adult. Additionally, all users are required to wear grip socks to prevent slipping, and all pockets are to be emptied, with no handheld objects allowed during jumping. Of note, none of the children who visited our ED for TRIs had sustained injuries from handheld objects. Flipping is allowed but at one’s own risk.(1) Studies and policies overseas also suggest that adult or parental supervision would significantly help to reduce TRIs.(4,12-14,22) However, there was no documentation on the presence of supervision in the data to sufficiently conclude if adult supervision had been adequate during trampoline use.
While most trampolines sold for home use have standard safety measures such as padded frames, these have shown to become ineffective over time. Moreover, private users may choose not to use additional safety equipment that may be sold with the trampoline. Ten of the injuries in our study were a result of the child falling directly onto the frame. Two children sustained lacerations to the face or head that required toileting and suturing, one required an ORIF and one sustained a fracture that was manually reduced in the ED. However, in three of these injuries, the child had been engaged in an activity that was not on the trampoline and had accidentally hit the frame, while another was a result of a child not following safety measures. It may be useful for outlets selling trampolines to ensure that buyers are adequately educated on the risks associated with trampoline use by providing safety handouts for users and caretakers. It should also be mandatory to have soft mats placed around the periphery of the trampoline. Double bouncing should be discouraged on home trampolines. Schools and homes can also take measures to install trampolines away from spaces where children are engaging in other sports activities.
This study was not without limitations. Being a retrospective study, the data collected depended entirely on the information documented by the ED physician who attended to the child on the day of presentation. As such, the amount of information collected for each ED visit varied. There was some incomplete data regarding the mechanism of injury, the location of injury, the design of the trampoline and the safety measures in place, limiting our assessment of the adequacy of these safety measures. Furthermore, this study also only examined a representative sample of ED visits. There was no way to ascertain the number of TRIs that did not present to our hospital, hence our findings may not be representative of the total number of paediatric TRIs in Singapore. As the aim of this study was to focus on the epidemiology and characteristics of each TRI, each child was not followed up on for long-term complications, such as neuropathies, or the psychological impact of the fall, although we noted that some children required long-term rehabilitation.
Further studies can be conducted in future with a larger sample size, to explore other factors such as the safety measures in place, type of trampoline used, size of the trampoline, body mass index of the injured patient, the presence of other users on the same trampoline, extent of parental supervision, and whether the child was performing a stunt. In addition, they can examine whether experience can reduce the number and severity of TRIs, such as comparing the number of days of trampoline experience and correlating it with the severity of the injury.
In conclusion, this study has found that the increase in the prevalence of trampolines has resulted in an increase in ED visits for TRIs, although the majority of the TRIs seen at our hospital were mild, with no deaths or severe neurological sequelae. To date, there have been many studies supporting regulation or banning of trampoline activities. However, trampolining is an engaging indoor activity that helps to improve motor control in children, and there are risks of falls and injuries as with all forms of physical activity. Instead of a ban, we would recommend that additional safety measures be taken, such as adequate education when selling trampolines, ensuring adult supervision, mandatory placement of mats around the periphery of all trampolines and restricting trampoline use to one person. Public trampoline parks can also consider increasing the age limit for public trampoline use.
ACKNOWLEDGEMENTS
We sincerely thank Ms Ng Wai Yee, Statistician, Department of Biostatistics, National University of Singapore, Singapore, for assisting in the interpretation of data. We also sincerely thank all of the ED doctors in KKH for contributing to the data collected as well as the staff of the National Trauma Registry, from whom we obtained the data.