Breast cancer metastases causing acute appendicitis are exceedingly rare, with only 14 reported cases,(1,2) for which the majority of the patients underwent appendicectomy and only 3 (21.4%) cases underwent right hemicolectomy. Knowledge of this phenomenon is important because while surgical appendicectomy is a straightforward operation, a complicated mass with suspicious nodes may present occasionally and require a more extensive operation.
A 59-year-old domestic helper presented with sudden-onset right iliac fossa pain of two days’ duration. On examination, her right iliac fossa was tender. Her total white cell count was 8 × 109/L. Computed tomography (CT) of the abdomen was performed in view of the high incidence of right-sided diverticulitis in the local community.(3) It showed a 4.3 cm × 1.2 cm rim-enhancing collection adjacent to the tip of an inflamed appendix with periappendiceal fat stranding, prominent ileocolic nodes and caecal wall thickening. A diagnosis of perforated appendicitis was made and laparoscopic appendicectomy was planned.
The patient also complained of a left breast lump that was getting larger. It had been evaluated two years before and classified as a suspicious (Breast Imaging Reporting and Data System score of 4) solid cystic lump with microcalcifications. She had been scheduled for histological correlation but subsequently defaulted on follow-up. On examination then, two lumps were present at the upper outer quadrant, measuring 4 cm and 5 cm, with palpable axillary lymph nodes. She had a family history of breast cancer, reached menarche at 14 years of age and had three children before 30 years of age, all of whom were breastfed for more than six months. Intraoperatively, we found a hard appendiceal mass, whose tip was adherent to the terminal ileum, and lymph nodes at the root of the mesentery. An open right hemicolectomy was performed. She recovered well and was discharged on postoperative Day 6.
Triple assessment of the breasts showed invasive ductal carcinoma with metastasis to the lymph nodes; it was found to be oestrogen receptor (ER) negative, progesterone receptor (PR) positive (weak) and human epidermal growth factor receptor 2 (HER2) positive. Pathological examination of the right hemicolectomy specimen showed a poorly differentiated adenocarcinoma involving the proximal appendix, with periappendicular abscess formation. Lymphovascular invasion was present. Five out of 18 lymph nodes had metastatic carcinoma. Neuroendocrine markers were negative. ER, PR and HER2 receptor status mirrored that of the breast carcinoma. Further workup with CT of the thorax did not locate any other sites of metastases. A final diagnosis of metastatic breast carcinoma causing acute appendicitis was established. Her case was discussed at a multidisciplinary tumour board meeting and surgical resection of the breast tumour, followed by chemotherapy and/or targeted therapy, was recommended. In view of financial reasons, she decided to return home to the Philippines for further treatment.
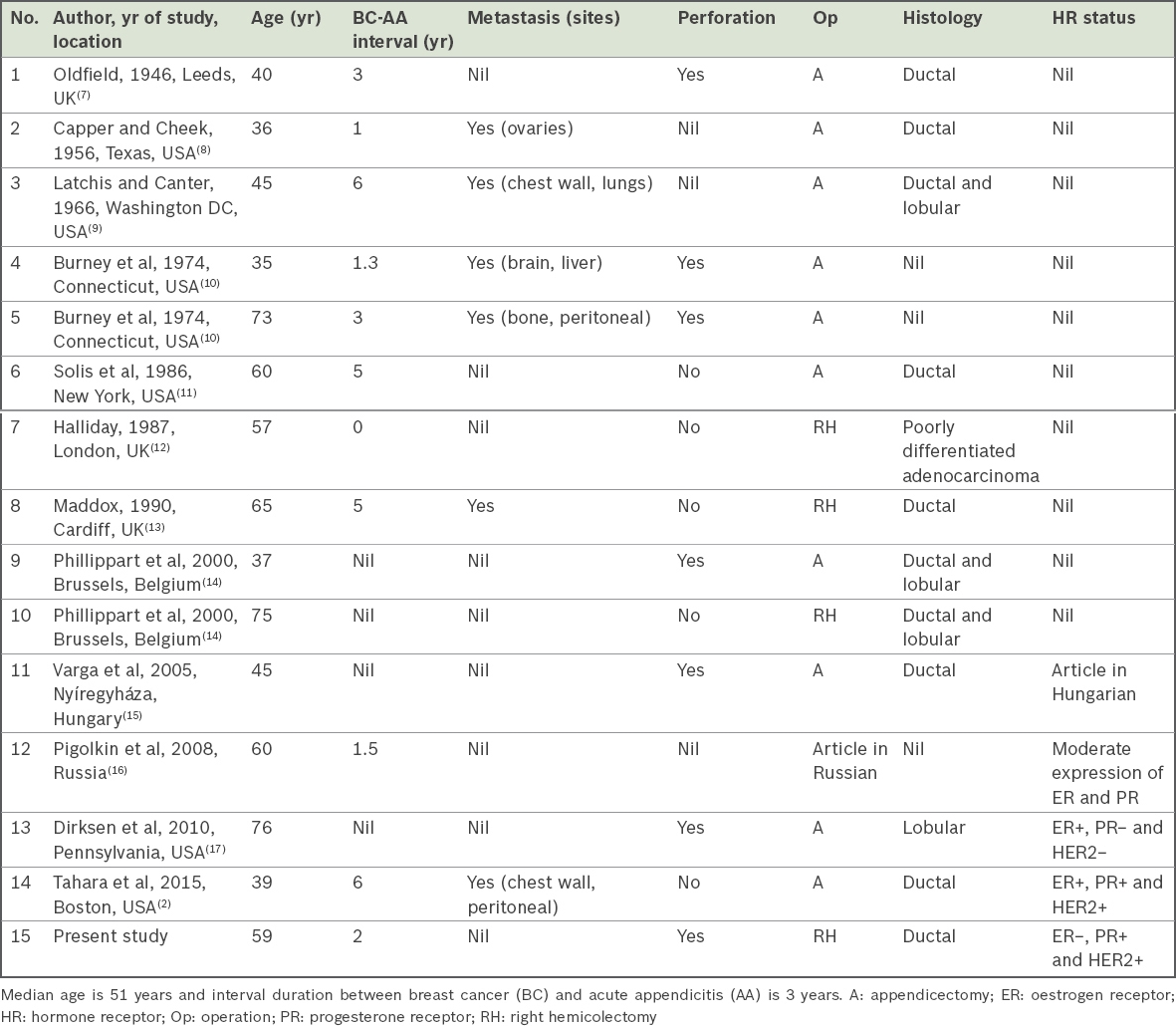
In a series of 7,970 appendicectomies, Connor et al(1) found that the incidence of metastasis to the appendix was 0.14%. To date, there have only been 14 reported cases (Table I) of breast metastasis to the appendix, which usually presents as acute appendicitis.(2) Right hemicolectomy for primary adenocarcinoma of the appendix, even as a secondary procedure, has shown a survival advantage.(4) Unfortunately, it is difficult to determine if this procedure provides a similar survival advantage for secondary metastases to the appendix, as there is insufficient data.
Finally, studies have previously shown that invasive lobular carcinoma is more likely to metastasise to the gastrointestinal tract than invasive ductal carcinoma.(5) This pattern is indeed evident in the series of 14 cases reported, with 4 (33%) out of 12 cases (after excluding cases with unknown types of breast cancer) having lobular pathology, higher than the usual incidence of lobular carcinoma (8%–14%).(6)
Table I
Case series of breast metastasis to appendix, as reported in the existing medical literature.
Yours sincerely,
References Connor SJ, Hanna GB, Frizelle FA.Appendiceal tumors: retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies.Dis Colon Rectum. 1998;41:75-80. Tahara RK, Keraliya A, Ramaiya NH, et al. Acute appendicitis secondary to metastatic carcinoma of the breast: case report and review of the literature.Cancer Treat Commun. 2015;4:41-5. Fong SS, Tan EY, Foo A, Sim R, Cheong DM.The changing trend of diverticular disease in a developing nation.Colorectal Dis. 2011;13:312-6. Nitecki SS, Wolff BG, Schlinkert R, Sarr MG.The natural history of surgically treated primary adenocarcinoma of the appendix.Ann Surg. 1994;219:51-7. Borst MJ, Ingold JA.Metastatic patterns of invasive lobular versus invasive ductal carcinoma of the breast.Surgery. 1993;114:637-41. Arpino G, Bardou VJ, Clark GM, Elledge RM.Infiltrating lobular carcinoma of the breast: tumor characteristics and clinical outcome.Breast Cancer Res. 2004;6:R149-56. Oldfield MC.Individual resistance to malignant disease;illustrated by a case in which a metastatic deposit from a carcinoma of the breast occurred in the appendix and led to perforation and peritonitis.Br Med J. 1946;2:153-5. Capper RS, Cheek JH.Acute appendicitis secondary to metastatic carcinoma of the breast.AMA Arch Surg. 1956;73:220-3. Latchis KS, Canter JW.Acute appendicitis secondary to metastatic carcinoma.Am J Surg. 1966;111:220-3. Burney RE, Koss N, Goldenberg IS.Acute appendicitis secondary to metastatic carcinoma of the breast. A report and review of two cases.Arch Surg. 1974;108:872-5. Solis OG, Ruffolo R, Pfieffer NC.Metastatic breast carcinoma presenting as acute appendicitis.N Y State J Med. 1986;86:271-2. Halliday A.Breast carcinoma presenting as acute appendicitis.Br J Clin Pract. 1987;41:804-5. Maddox PR.Acute appendicitis secondary to metastatic carcinoma of the breast.Br J Clin Pract. 1990;44:376-8. Philippart P, da Costa PM, Heymans O, et al. Metastatic involvement of ceco-appendicular segment: a diagnosis of right lower quadrant abdominal pain in patient receiving chemotherapy.Hepatogastroenterology. 2000;47:1627-9. Varga S, Konczili V, Zemanek P, Francz M, Nábrádi Z.[Metastasis of breast cancer presenting in the appendix].Magy Seb. 2005;58:334-6. Hungarian. Pigolkin II, DolzhanskiÄ OV, Kostin AI.[Appendicular metastatic involvement in breast cancer].Arkh Patol. 2008;70:46-8. Russian. Dirksen JL, Souder MG, Back AJ.Metastatic breast carcinoma presenting as perforated appendicitis.Breast Care (Basel). 2010;5:409-10.
REFERENCES
1. Connor SJ, Hanna GB, Frizelle FA. Appendiceal tumors: retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies. Dis Colon Rectum 1998; 41:75-80. https://doi.org/10.1007/BF02236899
PMid:9510314
2. Tahara RK, Keraliya A, Ramaiya NH, et al. Acute appendicitis secondary to metastatic carcinoma of the breast: case report and review of the literature. Cancer Treat Commun 2015; 4:41-5. https://doi.org/10.1016/j.ctrc.2015.04.001
3. Fong SS, Tan EY, Foo A, Sim R, Cheong DM. The changing trend of diverticular disease in a developing nation. Colorectal Dis 2011; 13:312-6. https://doi.org/10.1111/j.1463-1318.2009.02121.x
PMid:19906060
4. Nitecki SS, Wolff BG, Schlinkert R, Sarr MG. The natural history of surgically treated primary adenocarcinoma of the appendix. Ann Surg 1994; 219:51-7. https://doi.org/10.1097/00000658-199401000-00009
PMid:8297177 PMCid:PMC1243090
5. Borst MJ, Ingold JA. Metastatic patterns of invasive lobular versus invasive ductal carcinoma of the breast. Surgery 1993; 114:637-41.
PMid:8211676
6. Arpino G, Bardou VJ, Clark GM, Elledge RM. Infiltrating lobular carcinoma of the breast: tumor characteristics and clinical outcome. Breast Cancer Res 2004; 6:R149-56. https://doi.org/10.1186/bcr767
PMid:15084238 PMCid:PMC400666
7. Oldfield MC. Individual resistance to malignant disease; illustrated by a case in which a metastatic deposit from a carcinoma of the breast occurred in the appendix and led to perforation and peritonitis. Br Med J 1946; 2:153-5. https://doi.org/10.1136/bmj.2.4465.153
PMCid:PMC2053824
10. Burney RE, Koss N, Goldenberg IS. Acute appendicitis secondary to metastatic carcinoma of the breast. A report and review of two cases. Arch Surg 1974; 108:872-5. https://doi.org/10.1001/archsurg.1974.01350300102025
PMid:4829813
11. Solis OG, Ruffolo R, Pfieffer NC. Metastatic breast carcinoma presenting as acute appendicitis. N Y State J Med 1986; 86:271-2.
PMid:3459087
12. Halliday A. Breast carcinoma presenting as acute appendicitis. Br J Clin Pract 1987; 41:804-5.
PMid:3446280
13. Maddox PR. Acute appendicitis secondary to metastatic carcinoma of the breast. Br J Clin Pract 1990; 44:376-8.
PMid:2223534
14. Philippart P, da Costa PM, Heymans O, et al. Metastatic involvement of ceco-appendicular segment: a diagnosis of right lower quadrant abdominal pain in patient receiving chemotherapy. Hepatogastroenterology 2000; 47:1627-9.
PMid:11149019
15. Varga S, Konczili V, Zemanek P, Francz M, Nábrádi Z. [Metastasis of breast cancer presenting in the appendix]. Magy Seb 2005; 58:334-6. Hungarian.
PMid:16496779
16. Pigolkin II, Dolzhanskiĭ OV, Kostin AI. [Appendicular metastatic involvement in breast cancer]. Arkh Patol 2008; 70:46-8. Russian.
PMid:18727435
17. Dirksen JL, Souder MG, Burick AJ. Metastatic breast carcinoma presenting as perforated appendicitis. Breast Care (Basel) 2010; 5:409-10. https://doi.org/10.1159/000322656
PMid:21494407 PMCid:PMC3076354