

Abstract
INTRODUCTION
Patients receiving intravenous iodinated contrast media for computed tomography (CT) are predisposed to contrast-induced nephropathy. Chronic kidney disease is an important risk factor, and hydration is the mainstay of prevention. While inpatients can undergo intravenous hydration, limited knowledge exists regarding regimens for outpatients. We employed a rapid outpatient hydration protocol to reduce postponement of imaging appointments for patients with suboptimal estimated glomerular filtration rate (eGFR).
METHODS
From June 2015, we amended our CT preparation protocol to mandate rapid hydration (oral, intravenous or both) for patients with an eGFR of 30–60 mL/min/1.73 m2. Patients receiving this hydration protocol from June to November 2015 were followed up for one month to monitor any admissions for fluid overload, and up to one year to determine the long-term effect on eGFR.
RESULTS
226 outpatients received the hydration protocol, which correlated with a 95% reduction in postponement of imaging appointments. No complications of fluid overload from hydration were encountered. A significant association was observed between age and decrease in eGFR, but this was not significant when stratified by drop in eGFR category. No statistical significance was found between decrease in eGFR and gender or race. Higher baseline eGFR was less likely to be associated with decrease in eGFR after imaging. Type of hydration was not related to a drop in eGFR category for patients with an eGFR of 45–59 mL/min/1.73 m2.
CONCLUSION
We defined a shorter hydration regimen that is safe to use in the outpatient setting.
INTRODUCTION
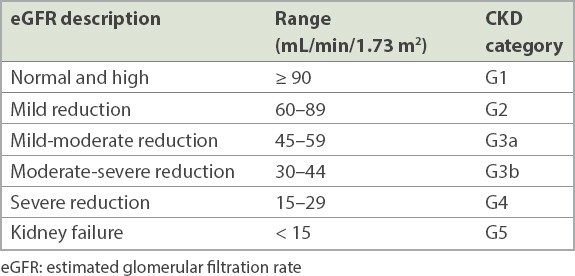
Computed tomography (CT) is one of the most commonly utilised radiological modalities for the imaging of structures within the human body, given its high spatial resolution and rapid image acquisition. In CT, intravenous iodinated contrast media (IOCM) is often used to enhance the visibility of internal organs and pathology. Patients receiving intravenous IOCM for CT imaging are predisposed to contrast-induced nephropathy (CIN). Impairment of renal function is reflected in the glomerular filtration rate (GFR), although there is no way of measuring this. Instead, surrogate measures such as serum creatinine and estimated glomerular filtration rate (eGFR) are used, but they have their drawbacks.
Although serum creatinine is the most commonly used measure of renal function, it has limitations as an accurate measure of GFR. Serum creatinine is considerably influenced by the patient’s gender, muscle mass, nutritional status and age. Test results can be normal even if GFR is abnormal, up to a nearly 50% reduction in GFR. This is because serum creatinine levels lag behind changes in renal function.(1) Although eGFR is more accurate than serum creatinine, its formula also partly relies on serum creatinine levels. Further, eGFR equations were established based on studies of narrow populations and individuals at a stable level of renal function, and not patients who were in an unsteady state when they were admitted.(2) As such, eGFR values will not be accurate at approximately the time after IOCM administration, when GFR is expected to fluctuate.
After IOCM administration, serum creatinine usually begins to rise within 24 hours, peaks within four days and returns to baseline within 7–10 days.(3) Diagnosis of CIN can be defined as a 25% increase in serum creatinine from baseline or 0.5 mg/dL rise in absolute creatinine over 48–72 hours.(3) It is unusual for patients to progress to acute kidney injury (AKI) or develop permanent renal dysfunction.(4) However, few studies have followed patients for more than 72 hours.(5)
The incidence of CIN ranges from 0% to 24%, varying widely depending on risk factors.(3) One important risk factor for CIN is having chronic kidney disease (CKD).(3,5,6) Compared to serum creatinine-based thresholds, eGFR thresholds (
With regard to the lower limit at which contrast should be avoided unless the benefits outweigh the risks of CIN, two large propensity score-adjusted studies have been reported. One showed no risk of CIN from IOCM, regardless of baseline eGFR,(11) while another revealed that patients with an eGFR < 30 mL/min/1.73 m2 are at significant risk (and those with eGFR 30–44 mL/min/1.73 m2 are borderline but do not have a statistically significant risk).(12) Hence, a lower limit of 30 mL/min/1.73 m2 appears most appropriate.(5)
As there is no definitive treatment for AKI, prevention of CIN is crucial.(3) Intravenous physiological saline is the established prophylaxis for CIN in patients with CKD.(5,9,13-15) A popular regimen is normal saline infused at 1 mL/kg/h for 6–12 hours before the procedure and continued for 6–12 hours afterwards.(3) Another possible protocol would be 0.9% saline at 100 mL/h, beginning 6–12 hours before and continuing 4–12 hours after the procedure, but this is practical only in the inpatient setting.(5) Two regimens have been reported – a standard protocol (0.9% normal saline at 3–4 mL/kg/h for four hours before and after contrast administration) and a long protocol (0.9% normal saline at 1 mL/kg/h for 12 hours before and after contrast administration).(2) For same-day infusion, normal saline is infused at 3 mL/kg/h for at least one hour before the procedure and six hours afterwards.(4) Isotonic fluids are preferred (lactated Ringer’s solution or 0.9% normal saline), but the ideal infusion rate and volume are unknown.(5)
These proposed regimens involve long periods of infusion, which are suitable for inpatients. However, there is a gap in knowledge regarding administering hydration in the outpatient setting. Hydrating outpatients would likely entail a more rapid rate given the constraints of time and space. A report by Hossain et al discusses barriers to implementing hydration from several perspectives.(3) Issues pertinent to us are lack of space for infusing, time and manpower required for monitoring, and a suitable billing charge for providing this adjunct service.(3,6,14)
Given the controversies regarding the degree of renal impairment at which there is increased risk of CIN and the potential limitations of hydration in an outpatient setting, the aims of our study were twofold. The primary aim was to ensure the safety of a rapid outpatient hydration protocol in the local setting of a tertiary hospital, thereby reducing postponements. Our secondary aim was to determine whether there is long-term impact on renal function beyond the expected duration of CIN (characterised by a statistically significant change in absolute eGFR values as well as eGFR categories), which could be affected by individuals’ demographics, baseline renal function and type of hydration.
MethodS
We conducted a retrospective review of secondary data of patients receiving hydration over a six-month period from June to November 2015, which was collected as part of quality improvement. All data had been collected on hard copies and filed. This included patients’ details, baseline eGFR, method of hydration, any admissions for fluid overload and follow-up eGFR levels. The data was tabulated in Microsoft Excel 2003.
Prior to 2015, our institution had followed a protocol for outpatients with intermediate risk (eGFR 30–60 mL/min/1.73 m2) who required IOCM for their CT (
Box 1
Protocol for outpatients with intermediate risk:
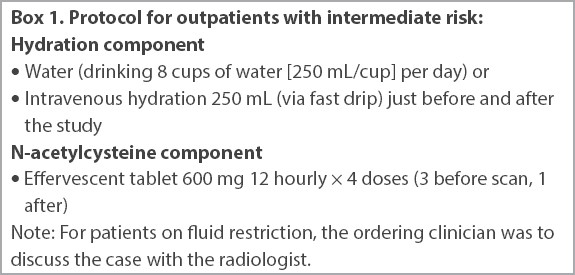
As N-acetylcysteine (NAC) was cost-effective and potentially beneficial with no adverse effects, it was recommended as part of the renal protective regimen.(3) The option of hydration was already in place but greatly underutilised. Only a minority of patients underwent intravenous hydration that required insertion of a cannula. Also, the definition of ‘fast drip’ was not clearly specified and carried a risk for patients on fluid restriction. Thus, it was easier to encourage patients to consume NAC orally, albeit with improper supervision and follow-up on the actual volume. Publications from 2014 to 2015 showed less support for the efficacy of NAC in the prevention of CIN.(3-6) Non-prescription of this medication by referring clinicians led to frequent postponements and rescheduled imaging. A consensus was reached among the main referring disciplines of the hospital, with the primary intention of reducing the postponement rate and inconvenience for the patient and the carer as part of quality improvement.
From June 2015, the CT preparation protocol was amended to make NAC optional. With the exclusion of NAC, we were compelled to adhere more closely to hydration, in particular via the intravenous route. The details and effects of hydration had hitherto been unproven.(14,15) Radiology trainees were tasked to screen for patients who might have undiagnosed renal dysfunction, counsel those with risk factors for CIN, employ a suitable hydration protocol for this group of patients and follow up for any adverse outcome, particularly admissions for fluid overload.
For patients at risk, eGFR was traced. Those who did not have a baseline eGFR were offered point-of-care testing (POCT) on the day of their imaging at a small cost, using the i-STAT® 1 Analyser MN:300 (Abbott Point of Care Inc, Abbott Park, IL, USA) device. The result of the POCT creatinine test is displayed in mol/L. This had to be converted to an eGFR value. Even prior to this study, our department had been using the online eGFR calculator available from the St George’s University of London’s website.(10) This calculator estimates eGFR based on the four-item Modification of Diet in Renal Disease (MDRD) formula: creatinine, age, gender and ethnicity.(10)
Thereafter, a suitable type of hydration was employed. For patients with a poorer eGFR of 30–44 mL/min/1.73 m2, intravenous infusion of 250 mL of normal saline before imaging and another 250 mL after imaging, over half an hour each, was recommended. Those with a better eGFR of 45–60 mL/min/1.73 m2 received a 500-mL bottle of mineral water and were encouraged to consume as much water as possible prior to imaging and to finish the remainder after imaging, before leaving the department. An oral-intravenous combination was permitted to make up the 500 mL. This was applicable to patients requiring CT of the abdomen and pelvis, who needed to drink fluids to fill the bowel loops as a type of contrast agent. The doctor decided on the ratio of the oral route to the intravenous route, depending on the patient’s tolerability to either. Care was taken for those with risks of fluid overload, including but not limited to cardiac and renal failure. We deemed that most patients would be under-hydrated owing to the need to fast for at least three hours before CT.
Given the space and manpower constraints, we decided to undertake infusion within the department. This also permitted close supervision of the patient to ensure that the necessary volume had been consumed. The patient then proceeded for the imaging. The contrast medium was low-osmolar iohexol 350, and the volume varied between 50 mL and 120 mL.
The rapidity of the infusion was an initial concern. Patients who had received hydration were followed up for one month to assess whether they had been admitted for fluid overload. Any eGFR test performed within this period was also noted. The earliest legitimate follow-up eGFR of those patients whose eGFR was still not measured within the month was retrieved from our hospital records within one year of CT. If this reading was not available, a creatinine value during a period of stability (e.g. close to the end of an admission) was used and converted to eGFR using the same calculator. The hospital laboratory also calculates eGFR using an MDRD formula that we acknowledge to be more accurate.(10) When it was available, we prioritised the laboratory result over our derived one.(10)
With regard to the determination of the category of CKD, our laboratory was unable to provide exact values whenever the eGFR was > 60 mL/min/1.73 m2 or < 30 mL/min/1.73 m2, which was a limitation. Thus, we did not treat eGFR as a continuous variable, but considered it in terms of whether it decreased or not. Similarly, we were unable to differentiate between CKD category G1 and G2 as well as between category G4 and G5. For practical purposes, we also evaluated CKD categories according to whether there was a decrease in eGFR.
Statistical analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp, Armonk, NY, USA) after data was anonymised. Student’s t-test was used to analyse continuous variables and Fisher’s exact test was applied to categorical variables. The study was approved by our institution’s Domain Specific Review Board.
RESULTS
Fig. 1
Flowchart shows overview of the study. eGFR: estimated glomerular filtration rate
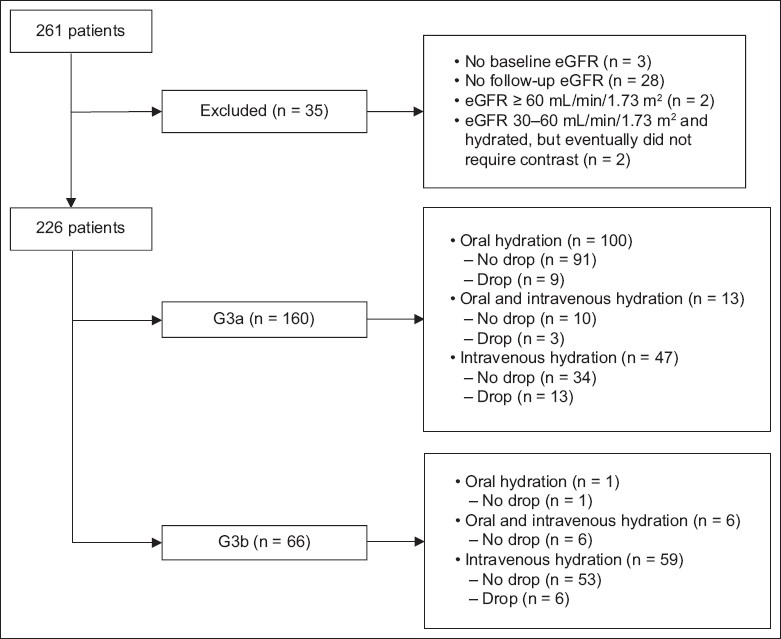
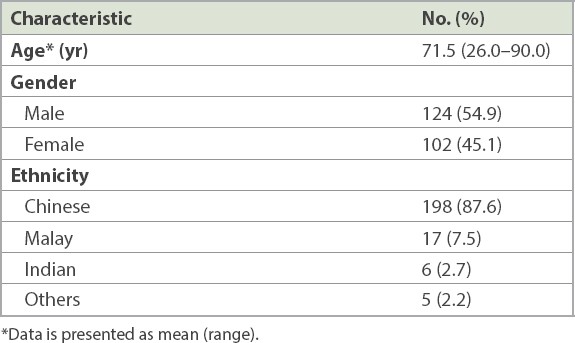
Table II
Demographics of the 226 patients.
No complications of fluid overload from hydration were observed. Only six cases were postponed over these six months, as compared to 119 cases in the preceding six months or 106 in the same period the year before. 73.5% of patients had their baseline eGFR assessed within six months prior to CT imaging. Another 15.9% required POCT on the same day. The remaining 10.6% had their eGFR measured more than six months before imaging. 15.9% of the patients had a follow-up eGFR measurement by 10 days. By six months, 85.8% of the patients had eGFR readings; the remaining 14.2% had their follow-up test at the end of one year.
The mean age of the 138 patients who did not show a decrease in eGFR was 70.4 ± 10.4 years, while that of the 88 patients who experienced a decrease was 73.2 ± 9.7 years, and the difference was statistically significant (p = 0.047). Despite the significant decrease in eGFR, we considered that using a drop in eGFR category as an indicator was more practical, as management of a patient changes only along with a change in eGFR category. The mean age of the 195 patients who did not show a drop in eGFR category was 71.1 ± 10.3 years, whereas that of the 31 patients who did was 73.9 ± 9.2 years. There was no significant difference between these groups (p = 0.134). When 60 years, 70 years and 75 years were used as cut-off values for age, the p-values were not statistically significant at 0.081, 0.264 and 0.493, respectively. There was also no statistical significance between decrease in eGFR and gender (p = 0.085) or race (p = 0.156).
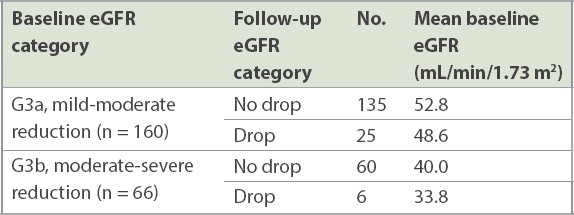
Table III
Changes in estimated glomerular filtration rate (eGFR) and baseline categories.
Hydration was mostly either oral (44.7%) or intravenous (46.9%), followed by the oral-intravenous combination (8.4%), as shown in
Table IV
Change in baseline estimated glomerular filtration rate (eGFR) category at follow-up based on choice of hydration.

In the G3a group, a statistically significant association was observed between the type of hydration and change in eGFR category (p = 0.005); patients receiving intravenous hydration showed a significant drop in their eGFR category. This was surprising, as intravenous hydration was expected to be more effective than the oral route, which has unreliable absorption and effectiveness.(3-6)
Given that the mean eGFR of the G3a group was 52.13 mL/min/1.73 m2, we stratified this group into two subgroups, one with better renal function (eGFR 53–59 mL/min/1.73 m2) and another with poorer renal function (eGFR 45–52 mL/min/1.73 m2). Chi-square test was repeated and showed no significant difference, with p-values of 0.546 and 0.111, respectively. Hence, the apparently worse outcome of intravenous hydration was more likely attributable to the fact that those receiving it had inherently poorer renal function to begin with. This test was not performed for those in the G3b group, as the number of patients was small.
DISCUSSION
IOCM used in CT carries the risk of CIN in patients with predisposing factors.(16) CIN is defined as acute deterioration of renal function within 48–72 hours of IOCM administration, with pre-existing CKD and concomitant diabetes mellitus being important risk factors.(3-6) Other risk factors include a dehydrated state, usage of a large volume of high-osmolarity IOCM or nephrotoxic medications and advanced age.(3) The risk of CIN is reduced by peri-procedural hydration, using low- or iso-osmolar intravenous IOCM and discontinuation of nephrotoxic drugs.(17-19) Intravenous hydration is the most important intervention, while premedication with reno-protective agent NAC is no longer used.(3-6)
The literature appears to suggest that oral hydration is not inferior to established intravenous hydration in prevention of CIN.(20,21) One potential outpatient hydration protocol included an intravenous bolus of 500 mL of normal saline before contrast administration and oral hydration more than eight hours after contrast administration.(22) Therefore, in mid-2015, our department implemented a rapid outpatient hydration protocol comprising either oral or intravenous peri-procedural hydration. This protocol was reserved for outpatient imaging of patients with pre-existing renal impairment (defined as eGFR < 60 mL/min/1.73 m2) who were not premedicated with NAC (which had been made optional). Under this protocol, imaging was still performed, with the patient receiving peri-procedural hydration intravenously or orally half an hour to one hour before and after imaging.
Implementation and evaluation of the effectiveness of the rapid outpatient hydration protocol in reducing CIN were challenging. Firstly, most established hydration protocols required continuous infusion over 24 hours peri-procedurally, rendering these possible only for inpatients, although a shortened duration over 6–7 hours has been proposed.(2,4) A knowledge gap in the literature still exists regarding the effectiveness of hydration protocols that would be applicable in the outpatient setting. Secondly, monitoring for CIN required trending of serum creatinine at 72 hours and 10 days after imaging, which would also be impractical for outpatients. Therefore, it would be more practical and more clinically relevant to assess the impact of our hydration protocol on renal function in the long term. We performed this by following up on the eGFR of all included patients over the course of one year. The study endpoint would then be suitable for determining whether outpatients with pre-existing renal impairment who were not premedicated with NAC, and who would otherwise have had their imaging postponed, could be safely imaged with this new protocol. Our main concerns were immediate complications, particularly that of fluid overload, as well as long-term impact on renal function in patients with pre-existing renal impairment.
Over the first six months of the implementation of the rapid outpatient hydration protocol, only six outpatient imaging procedures were postponed. This represented a 95% reduction in postponement of imaging. Further, no complications of fluid overload from hydration were observed. Although complication from intravenous hydration has been cited elsewhere,(13,14) it was not observed in our patients, who were all outpatients and may have fasted up to three hours beforehand, rendering them relatively under-hydrated.
Although our study suggested that advanced age was associated with a reduction in eGFR, this became statistically non-significant when it was correlated with a drop in eGFR category. Although different guidelines have proposed varying cut-off ages of 60, 70 and 75 years for when an individual would be at risk for CIN,(4,5) we found no evidence of this in our study. Our study also showed that change in eGFR was not significantly affected by gender or race.
Having a higher baseline eGFR, implying better renal function, may safeguard a patient from experiencing a drop in eGFR. Within groups G3a and G3b, this mean baseline eGFR was 52.8 mL/min/1.73 m2 and 40.0 mL/min/1.73 m2, respectively.
Our study also showed that change in eGFR category was not affected by the route of hydration (for the G3a group). This is consistent with reports in the literature that hydration may not be necessary for those with an eGFR of 45–59 mL/min/1.73 m2 receiving intravenous IOCM.(4) The initial and apparently worse outcome of intravenous hydration when compared to oral hydration was more likely attributable to the fact that this cohort of patients had inherently poorer renal function to begin with. They were then provided intravenous rather than oral hydration, with the assumption that the former would be more effective.(3-6)
Based on the first, single post-CT eGFR value, 31 patients showed a drop in at least one eGFR category from their baseline. None of these patients received cumulative doses of IOCM over the course of one year in the form of multiple CT imaging or angiography procedures that could have contributed to progressive chronic renal impairment.(1,23) The eGFR of 24 of these patients eventually recovered to the baseline category. The seven patients who showed no improvement had significant comorbidities (e.g. hypertension, diabetes mellitus and ischaemic heart disease) that could potentially have contributed to the progression. These had not been considered and were one limitation of the study. Provided that these patients remained stable, a longer follow-up period may be better to determine whether their eGFR gradually trended back towards baseline.
There is little evidence that IOCM is an independent risk factor for AKI in patients with eGFR ≥ 30 mL/min/1.73 m2.(1) Recent evidence suggested that there might be no significant difference in the incidence of CIN and contrast-independent acute renal impairment in patients with pre-existing renal impairment.(1,24,25) In line with our findings, we incidentally discovered two patients who received the hydration protocol and then eventually underwent non-contrast CT. One showed no drop in eGFR, while the other dropped one category following CT.
Our study had other minor limitations. Firstly, different methods were used to derive the baseline eGFR. In some patients, the creatinine value was derived from POCT and then converted to eGFR using an online calculator.(6) To minimise any discrepancy, priority was given to the value from the laboratory.(6)
Secondly, baseline eGFR was measured at different times. The maximum acceptable interval between baseline renal function assessment and contrast medium administration in at-risk patients has not been ascertained and can be up to six months.(4,5) Progressive deterioration in renal function may be ongoing between acquisition of baseline eGFR and imaging, exaggerating the results of patients with a decrease in eGFR or a drop in eGFR category. In addition, follow-up eGFR values were obtained at different times. However, our main aim was to evaluate safety based on whether any patient had been admitted for complications and the long-term impact on renal function, and not to plot the acute rise-drop of creatinine that suggests CIN. We considered only a single follow-up eGFR result, as we were not overly concerned with the trend of development and normalisation of eGFR, but rather with whether there was a change in absolute eGFR reading or change in category. Given the single reading, the absolute decrease was not as relevant, because a follow-up test might reveal normalisation. Therefore, more emphasis was placed on a drop in category, as this would affect management.
Finally, we acknowledge that this study was limited to hydration status and underlying renal function as risk factors for long-term eGFR decline. Other confounders such as concomitant diseases, both acute and chronic, and the primary cause for renal impairment were not studied, and may thus impair the conclusions stated.
In conclusion, our institution’s rapid outpatient hydration protocol has delineated a shorter period of hydration that is safe to use in the outpatient setting. This will alleviate patient and carer inconvenience, reduce expenditure and free up slots to accommodate more acute inpatients by avoiding rescheduling of postponed cases.
ACKNOWLEDGEMENTS
We would like to thank Mr Joshua Wong Guo Xian, Senior Medical Statistician, Office of Clinical Epidemiology, Analytics and Knowledge, Tan Tock Seng Hospital, Singapore, for his advice and help with statistics.