

Abstract
Radiation thyroiditis resulting from radioactive iodine-131 treatment for Graves’ disease is an uncommon complication. Although a majority of patients are asymptomatic or manifest mild symptoms that can be managed conservatively, published literature describing severe radiation thyroiditis resulting in significant morbidity is lacking. We herein report on six patients with severe radiation thyroiditis that resulted in hospitalisation, including an unusual complication of myopericarditis.
INTRODUCTION
Radioactive iodine-131 (RAI) has been utilised for the definitive treatment of Graves’ disease (GD) for many decades. Adverse events are uncommon, including thyroid swelling, radiation thyroiditis, sialadenitis and worsening of Graves’ ophthalmopathy (GO; also called Graves’ orbitopathy).(1) Radiation thyroiditis tends to occur within two weeks of RAI administration and is generally asymptomatic in most patients.(2) About 1%–5% of patients with GD develop radiation thyroiditis after RAI treatment. We herein report on six patients with GD who developed severe radiation thyroiditis that required hospitalisation subsequent to RAI treatment.
CASE SERIES
This was a retrospective case record review of 1,772 patients who received RAI treatment for GD from January 2014 to June 2018 at Singapore General Hospital, Singapore. The diagnosis of GD was established based on elevated free thyroxine (fT4) levels, with suppressed thyroid-stimulating hormone (TSH; or thyrotropin) levels and clinical examination findings such as diffusely enlarged goitre, typical signs and symptoms of hyperthyroidism, supported by positive TSH receptor antibodies (TRAb). The diagnosis of GO was made after consultation with an ophthalmologist and was based on the diagnostic criteria defined by Bartley and Gorman;(3) for instance, GO was deemed as present if eyelid retraction occurred in association with thyroid dysfunction, exophthalmos, optic nerve dysfunction or extraocular muscle involvement, and other confounding causes such as idiopathic orbital inflammation were excluded. The disease severity and activity of GO were scored based on the International Thyroid Eye Disease Society’s VISA classification.(4)
All patients received semi-empirical RAI dosing based on the estimated thyroid volume via clinical palpation. Goitre size was estimated according to the World Health Organization’s simplified classification of goitre: (a) small goitre (Grade 0), with no palpable or visible goitre; (b) moderate-sized goitre (Grade 1), with a mass in the neck that was consistent with an enlarged thyroid that was palpable but not visible when the neck was in the normal position; or (c) large goitre (Grade 2), with a swelling in the neck that was visible when the neck was in the normal position and was consistent with an enlarged thyroid when the neck was palpated.(5)
At our institution, small goitres generally receive 10–15 millicuries (mCi), moderate-sized goitres receive 15–20 mCi and large goitres receive 20–30 mCi of RAI. Antithyroid drugs (ATDs) are routinely discontinued 4–7 days prior to RAI treatment and restarted after three days at the discretion of the treating nuclear medicine physician. In addition, patients are instructed to follow a strict low-iodine diet for up to one week following the same period of ATD discontinuation for RAI treatment. Steroid prophylaxis, defined as at least two weeks of treatment with a pharmacological dose of glucocorticoids, is generally prescribed to patients with pre-existing GO, those with risk factors for GO progression (e.g. high TRAb and smoking) and those with large goitres to reduce the risk of radiation thyroiditis.
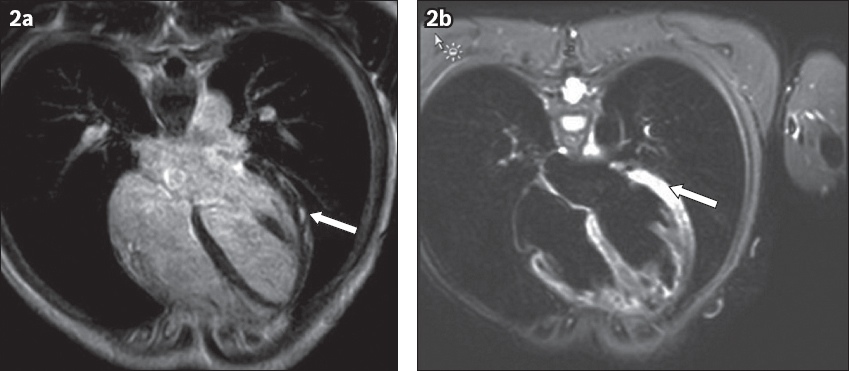
A summary of the clinical features and biochemical parameters of six patients who developed severe radiation thyroiditis that required hospitalisation subsequent to RAI treatment is presented in
Table I
Clinical characteristics of patients with severe radiation thyroiditis subsequent to RAI treatment (n = 6).
Patient 1
A 49-year-old Malay woman was diagnosed with Graves’ hyperthyroidism by her general practitioner after she presented with weight loss, palpitations and tremors. She was treated with carbimazole 5 mg OM (every morning). A month after treatment, she was admitted for fever and symptoms of upper respiratory tract infection. She was noted to be neutropenic, with an absolute neutrophil count of 0.0 × 103/mL, and was diagnosed with carbimazole-induced agranulocytosis. Her fT4 was 25.64 (normal range [NR] 10.0–20.0) pmol/L, TSH levels were suppressed, free tri-iodothyronine (fT3) level was 5.80 (reference range 2.6–5.7) pmol/L and TRAb level was elevated at 5.8 (NR < 2.0) IU/L. Carbimazole treatment was promptly withdrawn and she was referred for early RAI treatment. She received 23 mCi of RAI one day after hospital discharge, one week after carbimazole cessation. However, she was readmitted nine days after RAI treatment with high fever and severe neck pain. On examination, she was noted to be clinically thyrotoxic, and her neck was tender to palpation. Her fT4 level was 53.74 pmol/L and fT3 level was 22.8 pmol/L. Leucocyte count was normal at 5.8 × 103 (NR 4.0–10.0 × 103)/mL. Erythrocyte sedimentation rate was elevated at 87 (NR 3–15) mm/hr and C-reactive protein was 118.7 (NR < 3.0) mg/L. The patient was commenced on a tapering course of prednisolone 30 mg OM over three weeks, cholestyramine 4 g thrice daily and propranolol 20 mg thrice daily, with resolution of her symptoms. She developed hypothyroidism six weeks later and was commenced on thyroid hormone replacement.
Patient 2
A 72-year-old Malay woman had a seven-year history of GD complicated by thyrocardiac disease, with atrial fibrillation and recurrent admissions for congestive cardiac failure. A transthoracic echocardiogram in 2014 found an ejection fraction of 50%, severe triscupid regurgitation complicated by pulmonary hypertension (pulmonary artery systolic pressure 43 mmHg) and absence of regional wall motion abnormalities. The patient was eventually convinced to undergo definitive treatment and received 20 mCi of RAI. Her pre-RAI fT4 level was 6.4 (NR 8.8–14.4) pmol/L and TSH level was 26.4 (NR 0.65–3.70) mIU/L on carbimazole 5 mg OM. Five weeks after treatment, she presented with dyspnoea, diaphoresis and palpitations. She was noted to be febrile at 39.6°C, in fast atrial fibrillation of 206 beats per minute and hypertensive (systolic blood pressure/diastolic blood pressure 167/103 mmHg). There was no neck tenderness on physical examination. The patient was diagnosed with decompensated congestive cardiac failure complicated by fast atrial fibrillation, and was admitted to the high-dependency unit. Her fT4 level had increased to 41 (NR 8–21 L) pmol/L and TSH level to 6.32 (NR 0.34–5.60) mIU/L. TRAb was 0.6 (NR 0.0–1.0) IU/L but thyroid-stimulating immunoglobulins were elevated at 400% (NR 50%–179%). White blood cell count was elevated at 11.8 × 109 (NR 3.6–9.3 × 109)/L but C-reactive protein level was normal. The patient was restarted on carbimazole 2.5 mg OM, and intravenous hydrocortisone was administered. This was followed by rapid normalisation of her fT4 level to 15 (NR 8–21) pmol/L by Day 4 of admission. She was discharged without medications but eventually developed permanent hypothyroidism requiring long-term thyroid hormone replacement two months later.
Patient 3
A 16-year-old Chinese girl was diagnosed with GD at the age of nine years, with multiple hospitalisations for thyrotoxicosis due to non-compliance to ATDs. She received 20 mCi of RAI seven years after diagnosis. Her pre-RAI fT4 level was 20.03 (NR 10.7–18.4) pmol/L, TSH level was 0.008 (NR 0.35–5.0) mIU/L and TRAb level was 17.3 (NR 0.0–1.5) IU/L. She was prescribed a tapering two-week course of oral prednisolone 25 mg OM starting five days prior to RAI due to a pre-existing large goitre and was maintained on carbimazole 25 mg OM after RAI treatment. However, she was admitted two days after RAI treatment with palpitations and was noted to be tachycardic, with a heart rate of 119 beats per minute. There was no neck tenderness on examination. Her fT4 level on admission was 61.93 (NR 10.0–20.0) pmol/L, and TSH level < 0.004 (NR 0.4–4.0) mIU/L. White blood cell count was 10.4 × 103 (NR 4.0–10.0 × 103)/mL. She was continued on carbimazole 25 mg OM as well as oral prednisolone 15 mg OM for one week during her admission, with resolution of symptoms. She remained hyperthyroid after RAI and was maintained on carbimazole 15 mg OM. Further RAI treatment was planned at a later date.
Patient 4
A 56-year-old Chinese man was diagnosed with GD complicated by thyrocardiac disease ten years prior to RAI treatment. He was admitted for thyroid storm precipitated by non-compliance to ATDs and respiratory tract infection four years earlier. He eventually agreed to undergo definitive treatment with RAI and received 25 mCi of RAI. His pre-RAI fT4 level was 47.6 (NR 8.8–14.4) pmol/L and TSH level was 0.015 (NR 0.65–3.70) mIU/L while on carbimazole 30 mg OM. Tapering oral prednisolone at 20 mg OM was initiated over one week after RAI due to a pre-existing large goitre. However, the patient was admitted three weeks after RAI with fast atrial fibrillation and congestive cardiac failure. He was afebrile, tachycardic (heart rate 123 beats per minute) and normotensive (systolic blood pressure/diastolic blood pressure 110/79 mmHg). He was noted to have stopped his ATDs after RAI despite having been instructed to restart carbimazole post treatment. At this point, his fT4 level was 71.6 pmol/L, fT3 level was 24.3 (NR 3.2–5.3) pmol/L, TSH level was < 0.015 mIU/L, and both white blood cell count and C-reactive protein level were normal. He was restarted on carbimazole 15 mg twice daily and was commenced on a course of oral prednisolone 20 mg OM tapered over two weeks. He subsequently received a second course of RAI (dose 27 mCi) three months later due to persistent hyperthyroidism. No recurrence of radiation thyroiditis was noted after the second course of RAI. The patient developed permanent hypothyroidism two months later.
Patient 5
A 63-year-old Chinese man was diagnosed with GD five years earlier, presenting with fT4 level of 64.7 (NR 8.8–14.4) pmol/L, TSH level of 0.038 (NR 0.65–3.70) mIU/L and TRAb of 14.5 (NR 0.0–1.5) IU/L. No signs of GO were noted prior to RAI. He was recommended to undergo RAI treatment because he did not go into remission after a prolonged course of ATD treatment and received 15 mCi of RAI. Pre-RAI fT4 level was 16.0 pmol/L, TSH level was 0.033 mIU/L and fT3 level was 5.6 (NR 3.2–5.3) pmol/L while on carbimazole 5 mg OM. He was admitted a week after RAI with palpitations, chest pain, reduced effort tolerance, dyspnoea, diaphoresis, weight loss of 2 kg, hoarseness of voice, dysphagia and an episode of syncope. He also complained of orbital pain on extreme left lateral gaze. Physical examination showed mild left lid retraction but no proptosis, lid lag, lid oedema or chemosis. Extraocular movements were full, but he experienced pain on left upward and downward gaze. No neck tenderness was noted. At this point, his fT4 level was 37.6 pmol/L, TSH level was 0.030 mIU/L and fT3 level was 7.4 (NR 3.2–5.3) pmol/L. White blood cell count was normal at 4.93 × 103 (NR 4.0–10.0 × 103)/mL. He had resumed carbimazole three days after RAI, as instructed. Carbimazole was increased to 10 mg OM during admission, and he was commenced on prednisolone 40 mg OM for three days, with improvement in his symptoms. The patient was diagnosed with new-onset mild inactive thyroid eye disease by the ophthalmologist during admission and treated conservatively with topical lubricants. He was readmitted the day after discharge with fever, chest tightness, diaphoresis and dyspnoea. His fT4 and fT3 levels were 30.6 pmol/L and 6.1 pmol/L, respectively. Carbimazole was maintained, he was restarted on prednisolone 20 mg OM for two weeks, and was also treated with empirical intravenous antibiotics for the fever. The patient subsequently developed hypothyroidism three months after RAI treatment.
Patient 6
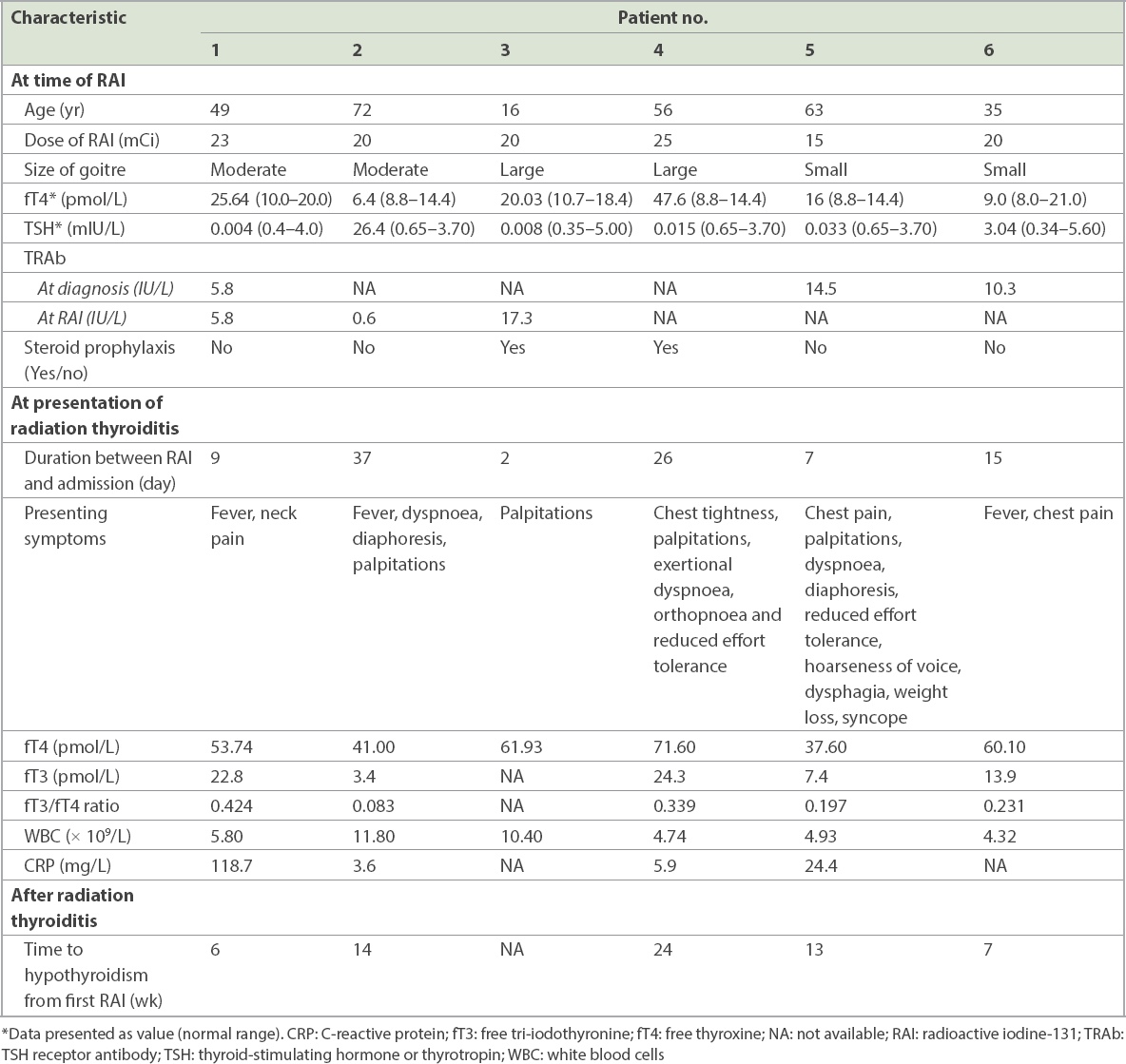
A 35-year-old Malay man was diagnosed with GD in September 2015, with an fT4 level of 56 (NR 8–21) pmol/L, TSH of 0.03 (NR 0.34–5.60) mIU/L and TRAb of 10.3 (NR 0.0–1.0) IU/L. He received 20 mCi of RAI three years after diagnosis. His fT4 level prior to RAI treatment was 9 (NR 8–21) pmol/L and TSH was 3.04 (NR 0.34–5.60) mIU/L while on carbimazole 2.5 mg OM. He was admitted two weeks later, presenting with one week of persistent fever followed by one day of retrosternal, burning chest pain that was exacerbated on lying supine and improved with sitting. He was afebrile, tachycardic (heart rate 114 beats per minute) and normotensive (systolic blood pressure/diastolic blood pressure 111/77 mmHg). There was no neck tenderness on physical examination. His heart sounds were normal, and no murmur or pericardial rub was noted on auscultation. On admission, his fT4 level was 60.1 (NR 8.8–14.4) pmol/L, TSH level 0.020 (NR 0.65–3.70) mIU/L, creatine kinase level 551 (NR 56–336) U/L, creatine kinase-MB (heart muscle) 29.2 (NR 1.0–5.0) mg/L and troponin-T 873 (NR < 30) ng/L. Electrocardiogram demonstrated an early repolarisation pattern (
Fig. 1
ECG of Patient 6 shows an early repolarisation pattern.
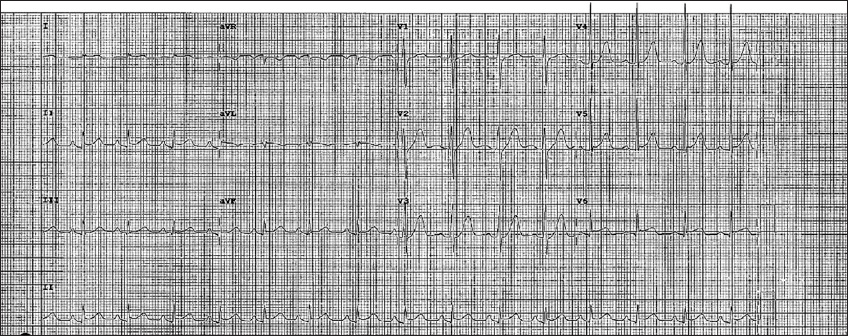
Fig. 2
(a) T1-W and (b) T2-W cardiac MR images of Patient 6 show possible myocarditis (arrows).
DISCUSSION
In this study, we described six patients who developed severe radiation thyroiditis subsequent to RAI treatment for GD that was significant enough to result in hospitalisation. Half of the patients were hyperthyroid at the time of RAI administration – Patient 2 was biochemically hypothyroid and two other patients were euthyroid. Interestingly, two patients (Patients 3 and 4) had received steroid prophylaxis for large goitres, but this did not prevent radiation thyroiditis from occurring. Although glucocorticoid prophylaxis is often given in clinical practice to prevent radiation thyroiditis, there are no guidelines that specify the indications for prophylaxis, or the dose and duration of glucocorticoid therapy. Hospitalisations occurred at a median of 12 (range 2–37) days after RAI. All six patients had a marked increase in fT4 between the time of RAI and hospital admission. The majority of the individuals had no leucocytosis on admission. Notably, only Patient 1 had neck pain. Two patients (Patients 2 and 4) had underlying thyrocardiac disease and presented with fast atrial fibrillation and congestive cardiac failure. Patient 5 developed mild GO after RAI, a complication with a reported incidence of 4.8%–8%(6,7) that is postulated to increase TRAb directed against released thyroid autoantigens after RAI, stimulating orbital TSH receptors and mediating orbital inflammation.(8) De novo occurrence of GO post RAI is uncommon but has been described in the published literature.(9) Patient 6 had an atypical presentation of myopericarditis.
The postulated mechanism for radiation thyroiditis involves RAI-induced injury to the thyroid follicular cells, which results in the acute release of stored thyroid hormone into the circulation, resulting in variable clinical manifestations such as anterior neck swelling, neck pain and tenderness, dysphagia and, rarely, thyroid storm.(10) The temporary exacerbation of thyrotoxicosis may also be contributed by cessation of ATDs around the time of RAI, and this was most apparent in Patient 4, who did not resume carbimazole three days after RAI. The cited prevalence of radiation thyroiditis after RAI for GD is 1%–5%, but this figure may be underreported since a majority of patients are asymptomatic and those who have symptoms are typically treated in the outpatient setting.(11) Those at risk of severe exacerbation of thyrotoxicosis are typically elderly or have severe symptoms of thyrotoxicosis, an fT4 level that is at least two times above the reference range, or underlying cardiovascular or cerebrovascular disease.(10)
Risk factors for the development of radiation thyroiditis reported in the literature include high TRAb at diagnosis, high dose of RAI and high fT4.(12,13) Radiation thyroiditis is presumed to be unlikely at doses below 200 Gy (equivalent to about 15 mCi), with each 100-Gy increment above 200 Gy resulting in an additional 5% risk of radiation thyroiditis.(13) Nonetheless, the dose-response relationship between the two is not linear, and large inter-individual variations do exist.(14) We note that five of the six patients in our series received more than 15 mCi of RAI. The RAI doses used for treatment of GD are generally higher in our institution’s experience, presumably due to the longer duration of ATD treatment locally. This is because our patients are generally less receptive to using RAI therapy early on in the course of their disease, as was demonstrated by Sztal-Mazer et al, who reported that 29.4% of patients in Asia selected RAI as the primary treatment modality, in contrast to 58.6% in North America.(15)
Several studies have demonstrated an increase in cardiovascular morbidity and mortality after treatment of hyperthyroidism with RAI when compared to treatment with thyroidectomy; this is attributed to a delay in the restoration of a euthyroid state after RAI, resulting in more prolonged exposure to stress on the cardiovascular system when compared to patients who underwent thyroidectomy.(16-18) Patients 2 and 4 in our study had underlying thyrocardiac disease, and presented with fast atrial fibrillation and congestive cardiac failure. In our institution, we routinely withdraw ATDs 4–7 days before RAI treatment and resume them three days after RAI treatment for all patients. Previous studies have shown that ATD treatment given in the week before RAI treatment reduced the success rate of RAI.(19) ATDs were resumed after RAI treatment to avoid transient exacerbation of thyrotoxicosis after RAI and its potential negative consequences, especially for patients who may be at risk of complications from thyrotoxicosis.(20)
Pericarditis associated with GD has rarely been reported. The exact aetiology is unknown, but an autoimmune mechanism has been postulated.(21) Myopericarditis, on the other hand, has not been reported in the published literature, to our knowledge. Our patient had high creatine kinase-MB, which suggested myocardial injury. In addition, the presence of normal coronary arteries on cardiac catheterisation, apical hypokinesia on echocardiogram and magnetic resonance imaging findings of myocardial oedema and delayed subepicardial enhancement with gadolinium contrast were in keeping with the diagnosis of myopericarditis. The temporal sequence between the occurrence of myopericarditis and the dramatic acute surge in the patient’s thyroid hormones by sixfold over two weeks due to RAI thyroiditis is suggestive of an association. Several lines of evidence may support this association: RAI treatment may have contributed to an acute alteration in fatty acid metabolism in the pericardium.(17) Pericardial brown adipose tissue is activated by hyperthyroidism, which drives an increase in fatty acid oxidation and inflammation, thus leading to pericarditis.(17) Moreover, TSH receptor mRNA has been demonstrated to exist in the myocardium.(18) Concomitant myocardial injury in our patient may be due to the rise in TRAb targeted at thyroid autoantigens released from damaged thyroid follicular cells after RAI, which, in turn, stimulate myocardial TSH receptors and mediate myocardial inflammation. No myocardial biopsy was performed for our patient, and his symptoms rapidly resolved upon initiation of anti-inflammatory drugs and with improvement of his thyroid hormones. To the best of our knowledge, this is the first report of myopericarditis occurring in a patient with severe radiation thyroiditis subsequent to RAI treatment for GD.
The management of radiation thyroiditis includes nonsteroidal anti-inflammatory drugs, beta-blockers to control the adrenergic symptoms, and glucocorticoids. A majority of our patients were treated with a combination of carbimazole and prednisolone at presentation, which highlights the challenge in establishing a definitive diagnosis of radiation thyroiditis versus a transient exacerbation of thyrotoxicosis due to cessation of ATD. Notably, a majority of our patients did not present with neck pain or tenderness, and three patients presented with thyrotoxicosis more than two weeks after RAI treatment. Some authors have suggested the use of thyroid scintigraphy or thyroid ultrasonography, with colour flow Doppler, to distinguish thyroid hyperactivity from destructive thyroiditis.(22,23) The ratio of tri-iodothyronine (T3) to thyroxine (T4) may also be useful, as a hyperactive thyroid produces more T3 than T4, whereas more T4 is released in thyroiditis, so that a T3/T4 ratio less than 20 is suggestive of thyroiditis.(24,25) More recently, Chen et al have suggested a fT3/fT4 cut-off of 0.4056 to distinguish GD from destructive thyroiditis, with a sensitivity of 96.6% and specificity of 72.7%.(26) We noted with interest that an fT3/fT4 ratio of less than 0.4056 was seen in four of five patients in our series for whom this data was available. Nonetheless, the rapidity of symptom resolution and improvement of thyroid hormone levels upon initiation of anti-inflammatory agents in all our patients suggest that post-radiation thyroiditis was the predominant cause of their clinical presentations.
In conclusion, radiation thyroiditis is a complication of RAI for treatment of GD and may result in significant morbidity. It has variable onset and clinical presentation, as demonstrated in this case series, ranging from symptoms of thyrotoxicosis to exacerbation of thyrocardiac disease and myopericarditis. Patients admitted with severe thyrotoxicosis soon after RAI should be suspected to have radiation thyroiditis as the aetiology, as pain and fever are uncommon as presenting symptoms. Thus, a high index of suspicion is necessary to ensure prompt initiation of anti-inflammatory treatment. In addition, extra caution should be exercised when administering RAI to patients with thyrocardiac disease, and closer monitoring of these patients is prudent.