

Abstract
INTRODUCTION
We developed an accelerated clinical pathway involving outpatient surgery for patients undergoing total knee arthroplasty (TKA) who are healthy enough for early discharge.
METHODS
Between March 2014 and April 2015, 89 TKAs were performed at a single institution by a single orthopaedic surgeon. 31 patients met the inclusion criteria for the study. All patients received 2 g tranexamic acid and 750 mg cefuroxime sodium intravenously 30 minutes prior to surgery. A multimodal protocol for perioperative pain management was used for all patients.
RESULTS
31 patients (three male, 28 female), with a mean age of 67 (range 49–78) years, who underwent TKA were enrolled in this study. The mean length of hospital stay was 28.7 (range 16–49) hours and mean duration of surgery was 92 (range 75–128) minutes. Combined spinal epidural anaesthesia was performed for 23 (74.2%) patients and general anaesthesia was used in 8 (25.8%) patients. Among the 31 patients, 23 (74.2%) patients were discharged within 23 hours of surgery.
CONCLUSION
Early discharge of patients following outpatient surgery for TKA was not associated with any procedure-related complications among the selected patients up to three months postoperatively.
INTRODUCTION
Total knee arthroplasty (TKA) and hip arthroplasty surgeries have traditionally been performed in an inpatient setting. The average length of stay after TKA has decreased in recent years because of improved postoperative clinical pathways,(1-3) which are associated with improvements in postoperative pain management, rehabilitation protocols, less invasive surgical techniques and early mobilisation of patients. Previous publications have indicated that the average length of stay following TKA can be decreased without increasing perioperative complications.(4,5) We developed an accelerated clinical pathway for patients undergoing outpatient surgery for TKA who are healthy enough for early discharge. This pathway combines preoperative patient education, oral pain medications, early mobilisation and intensive physical therapy. This article reports our initial experience of attempting outpatient TKA.
METHODS
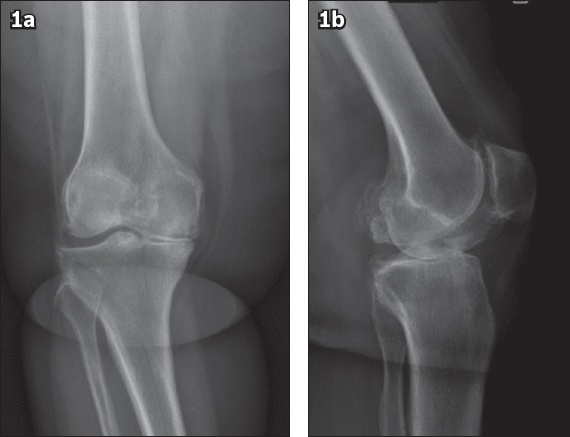
Between March 2014 and April 2015, 89 TKAs were performed at Private Medicabil Hospital in Bursa, Turkey, by a single orthopaedic surgeon. All patients were clinically and radiologically indicated for TKA (
Fig. 1
Preoperative radiographs in (a) anteroposterior and (b) lateral view show a patient’s knee prior to total knee arthroplasty.
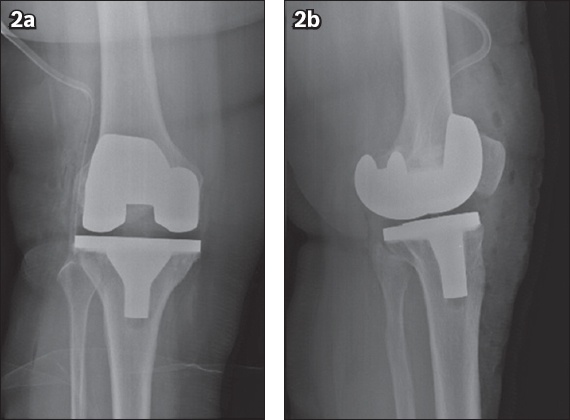
Patients were admitted to the hospital on the day of surgery. All surgeries were performed by the same orthopaedic surgeon using an anteromedial standard-length incision in the standard parapatellar approach, with the application of an uncemented prosthesis (SIGMA® Total Knee System [DePuy Synthes, Raynham, MA, USA]; GENESIS II Total Knee System [Smith & Nephew, London, UK]) (
Fig. 2
Postoperative radiographs in (a) anteroposterior and (b) lateral view show a patient’s knee following total knee arthroplasty.
At 23 hours after TKA, the dressings were changed and drains removed. Patients were re-evaluated for discharge from the hospital by a team consisting of an orthopaedic surgeon, anaesthesiologist, physical therapist and clinic nurse. Patients were accepted as suitable for discharge if they were able to walk 20 m with a walking aid, climb one or more flights of stairs, and get out of bed and onto a chair independently, and had a visual analogue scale (VAS) score < 3. All patients were prescribed 37.5 mg tramadol/325 mg paracetamol (Zaldiar) and 40 mg enoxaparin (Clexane). Patients were scheduled for wound inspection and evaluation one week following discharge, and for subsequent follow-up examinations at 15 days, one month, two months and three months.
RESULTS
The study included a total of 31 patients (three male, 28 female), with a mean age of 67 (range 49–78) years and mean body mass index of 33.5 (range 26–39) kg/m2. The mean length of hospital stay was 28.7 (range 16–49) hours. The mean duration of surgery was 92 (range 75–128) minutes. Combined spinal epidural anaesthesia was performed for 23 (74.2%) patients and general anaesthesia was used in 8 (25.8%) patients. Erythrocyte suspension was transfused in 15 patients. Of the 31 patients, 23 (74.2%) patients were discharged within 23 hours of surgery. Among the other 8 (25.8%) patients, two could not be efficiently and independently mobilised, three had pain, one had postoperative hypotension, one had decreased oxygen saturation postoperatively, and one stated that she would not feel safe at home. These eight patients were discharged within 48 hours of surgery.
Within the first week after discharge, 5 (21.7%) patients were readmitted to the hospital. Of these, three had drainage in their dressings and had them changed; one had swelling on the operated leg for which a compressive bandage was applied; and the other patient could not tolerate the 37.5 mg tramadol/325 mg paracetamol treatment and the analgesic regimen was changed to 75 mg diclofenac sodium and 500 mg paracetamol. No further problems were encountered during follow-up in these early discharge patients. During follow-up, VAS scores for all patients were < 3 and drainage in the dressing disappeared for three patients. No procedure-related complications were encountered in the study group at the end of three months.
DISCUSSION
Perioperative and postoperative improvements, including less invasive surgery, effective pain control, early mobilisation and rehabilitation protocols, have enabled earlier hospital discharge of patients undergoing TKA. Various studies have shown that patients discharged early following TKA have similar results to those with longer hospital stays.(6) Other centres from the United States and Europe have also reported on outpatient total hip and knee arthroplasty replacements.(7,8) As early hospital discharge entails a reduction in healthcare costs associated with TKA, there is a general trend towards adopting outpatient joint replacement wherever possible, especially as admitted patients are charged by the night in some centres. Another key reason for preferring joint replacement in an outpatient setting is that this approach helps to prevent nosocomial infections and the spread of multiresistant micro-organisms in the hospital.(9)
In our study, 23 (74.2%) of 31 patients fulfilling the discharge criteria went home within 23 hours of surgery. Within one week of discharge, five patients were readmitted to the hospital due to wound leakage in three patients, swelling in one patient and drug intolerance in one patient. No further complications developed in these patients during follow-up. As wound leakage and pain following TKA are not specific to outpatients and can occur in other settings as well, the complications noted among our patients were not necessarily due to the procedure being performed in an outpatient setting.
It is important that plans for outpatient treatment protocols be explained to patients. A clear explanation of postoperative pain management protocols and the overall concept of outpatient surgery provided by the surgeon would reassure patients that the primary aim of opting for such an approach is their comfort and safety. Generally, patients would be agreeable to a shorter hospital stay if they understood what was being planned. The major hindrance, in our experience, is convincing patients that they would remain safe, comfortable and pain-free at home in spite of early discharge following surgery. Therefore, for the patient to believe in the benefits of undergoing surgery in an outpatient setting, it is imperative that clear, comprehensible information be provided preoperatively about every aspect of the treatment.
Given that the main objective of performing surgery in an outpatient setting is to achieve early postoperative mobilisation with the aim of same-day discharge, postoperative pain management must be effectively provided for these patients without any analgesic gaps or periods of inadequate pain control.(10) The multimodal analgesic regimen chosen should cover the entire operative period. The course of action for the preoperative period includes patient education, a short fasting period, proper hydration, pre-emptive analgesia with fentanyl and sedation with midazolam. Periarticular injection is a part of the multimodal regimen. The combination indicated by the Ranawat Orthopaedic Center(11) was used in this study. The agents were administered directly into the surgical site by the orthopaedic surgeon. As the combined duration of the effect extends from the immediate intraoperative period to as long as 48–72 hours postoperatively, it is an attractive option for preventing analgesic gaps.(12) Using these medications intraoperatively also reduces the requirement for postoperative opioids in many patients, which helps to reduce the risk of opioid-related adverse events.
In their study, Kolisek et al used continuous femoral nerve block and single sciatic nerve block with intravenous sedation for patients’ anaesthesia.(6) In another study, spinal anaesthesia was performed after femoral nerve block for postoperative pain management.(13) These authors reported good results for pain control.(13) Prior to the present study, we had attempted anaesthesia via sciatic and femoral nerve blocks and also used a femoral nerve catheter for postoperative pain control. However, in our previous study, weakness of the quadriceps muscle in patients after femoral block prevented physical therapy and early mobilisation. Accordingly, we avoided the use of peripheral nerve blocks in the present study to allow for the early mobilisation of patients.
Outpatient arthroplasty is not appropriate for all patients.(14) Those who are considered for it should have no history of cardiac, pulmonary, renal or vascular disease. It is absolutely vital that there is family or other support available for postoperative care at home.(15) The patient should also reside in the same city as the centre of surgery in order to enable easy patient access for the surgeon in case of need. Finally, the patient should consent to the surgery in an outpatient setting. In our study, although 89 TKA operations were performed during the study period, only 31 procedures were performed in the outpatient setting. A key reason for the small sample size was patient refusal of outpatient arthroplasty surgery. This again highlights the importance of patient education.
Our study was not without limitations. The study population was small. Furthermore, the study was not designed as a randomised controlled trial nor were results compared among patients with respect to variables such as complications, clinical outcomes, patient satisfaction or financial analysis. Although the mean length of hospital stay for patients undergoing traditional TKA surgery at our hospital was 2.4 days, nearly the same protocol was used in all arthroplasty procedures for rapid recovery and early mobilisation of patients. It was also not possible to make a direct comparison of outcomes between inpatients and outpatients, as variations among surgical techniques, anaesthetic techniques and rehabilitation programmes were likely to have influenced recovery and outcomes in these two cohorts. In addition, the nature of the study did not allow any randomisation of patients. As patients in outpatient settings are younger and likely to be without comorbidities, selection bias was inherent in the choice of patients for outpatient TKA. A randomised study with a similar patient group is warranted to eliminate such factors that could affect patient outcomes.
In conclusion, the present study was designed to describe our initial experience of outpatient TKA under an accelerated clinical pathway. The demand for TKAs is expected to rise as populations continue to age. Healthcare systems exert pressure on orthopaedic surgeons to produce successful outcomes and reduce the costs incurred by the system. Although no financial analysis was done to compare our patients with those undergoing traditional TKA, our findings indicate that early discharge did not result in significant procedure-related complications up to three months postoperatively among patients selected to undergo TKA in outpatient settings.