Author Information >Copyright and License information >
1Department of Neonatal and Developmental Medicine, Singapore General Hospital, Singapore 2Duke-NUS Medical School, Singapore 3Yong Loo Lin School of Medicine, National University of Singapore, Singapore 4National Resuscitation Council Singapore, Members of the Neonatal Resuscitation Guidelines Workgroup (2015–2016), Singapore 5Department of Neonatology, National University Hospital, Singapore 6Kinder Clinic Pte Ltd, Singapore 7Department of Neonatology, KK Women’s and Children’s Hospital, Singapore Correspondence: Adj A/Prof Yeo Cheo Lian, Senior Consultant Paediatrician, Department of Neonatal and Developmental Medicine, Singapore General Hospital, 20 College Road, Academia, Singapore 169856. yeo.cheo.lian@singhealth.com.sg
We present the revised Neonatal Resuscitation Guidelines for Singapore. The 2015 International Liaison Committee on Resuscitation Neonatal Task Force’s consensus on science and treatment recommendations (2015), and guidelines from the American Heart Association and European Resuscitation Council were debated and discussed. The final recommendations of the National Resuscitation Council, Singapore, were derived after the task force had carefully reviewed the current available evidence in the literature and addressed their relevance to local clinical practice.
Keywords: National Resuscitation Council guidelines for resuscitation 2016, neonatal resuscitation, newborn resuscitation
BACKGROUND AND INTRODUCTION
Ongoing research and evidence is a stimulus for change to the science and art of neonatal resuscitation. With the release of the 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations (CoSTR),(1-3) the National Resuscitation Council, Singapore, convened a workgroup to review and update the existing guidelines on neonatal resuscitation. The update is based on the international recommendations from the International Liaison Committee on Resuscitation (ILCOR), adjusted appropriately for relevance to local clinical practice and previously evaluated evidence.(4,5) The review updates and enhances the existing newborn and paediatric resuscitation guidelines, which were last reviewed and released in 2011.(6)
The guideline applies to newly born infants (infant at time of birth) transitioning from intrauterine to extrauterine life irrespective of place of birth, and newborn infants who have completed newborn transition and require resuscitation during the initial hospitalisation. The sequence of the discussion on treatment recommendations and practice guidelines is organised in alignment with the newborn resuscitation algorithm:
Detection of heart rate (HR) – comparing electrocardiography (ECG) with oximetry or auscultation
Oxygen administration and continuous positive airway pressure (CPAP)
Positive pressure ventilation (PPV) and positive end-expiratory pressure (PEEP)
Endotracheal intubation and laryngeal mask airway (LMA)
Chest compression
Medications
Post-resuscitation care
Withholding resuscitation and discontinuing resuscitative efforts
Briefing and debriefing
Training in neonatal resuscitation – provider and instructor training
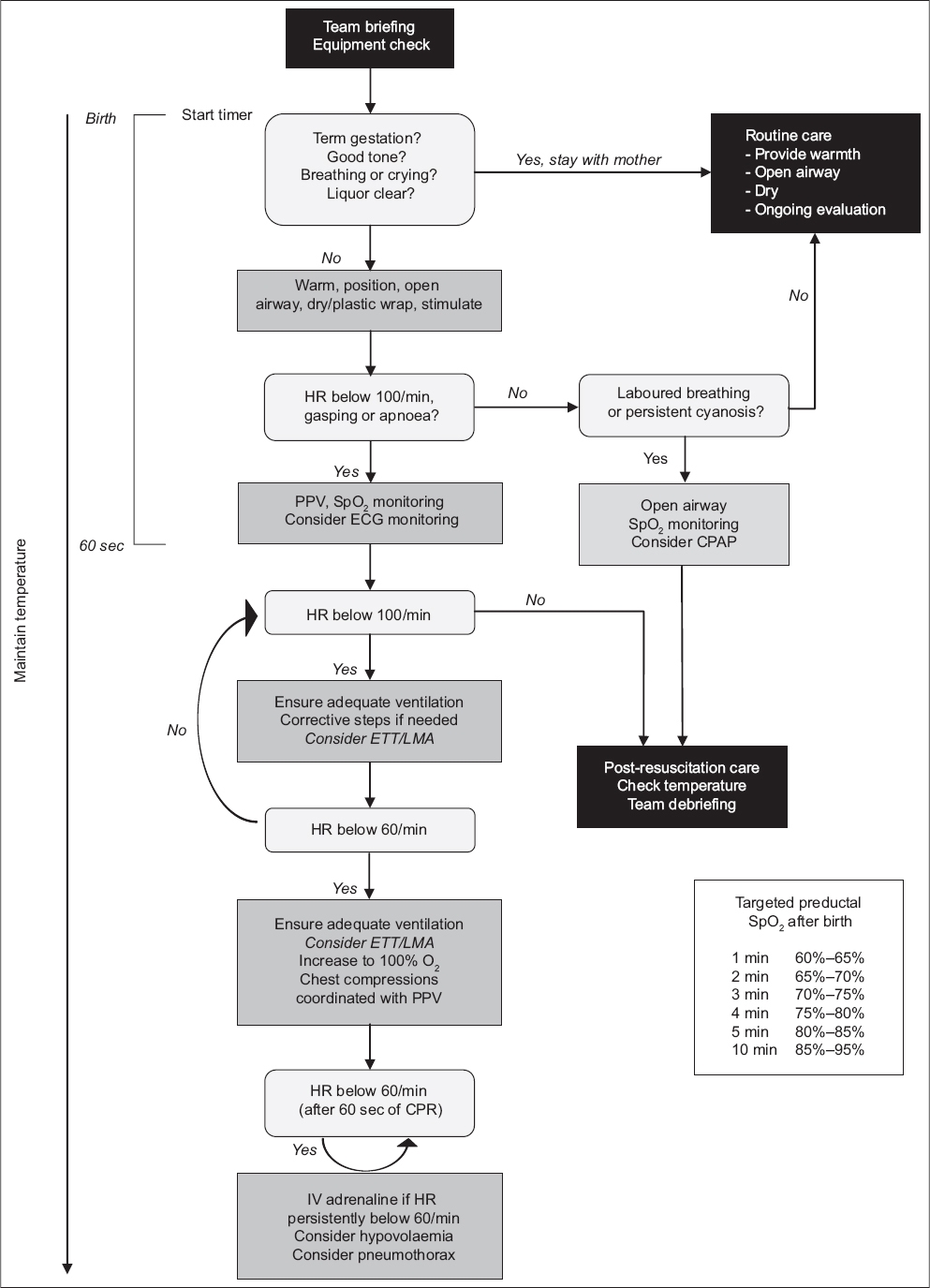
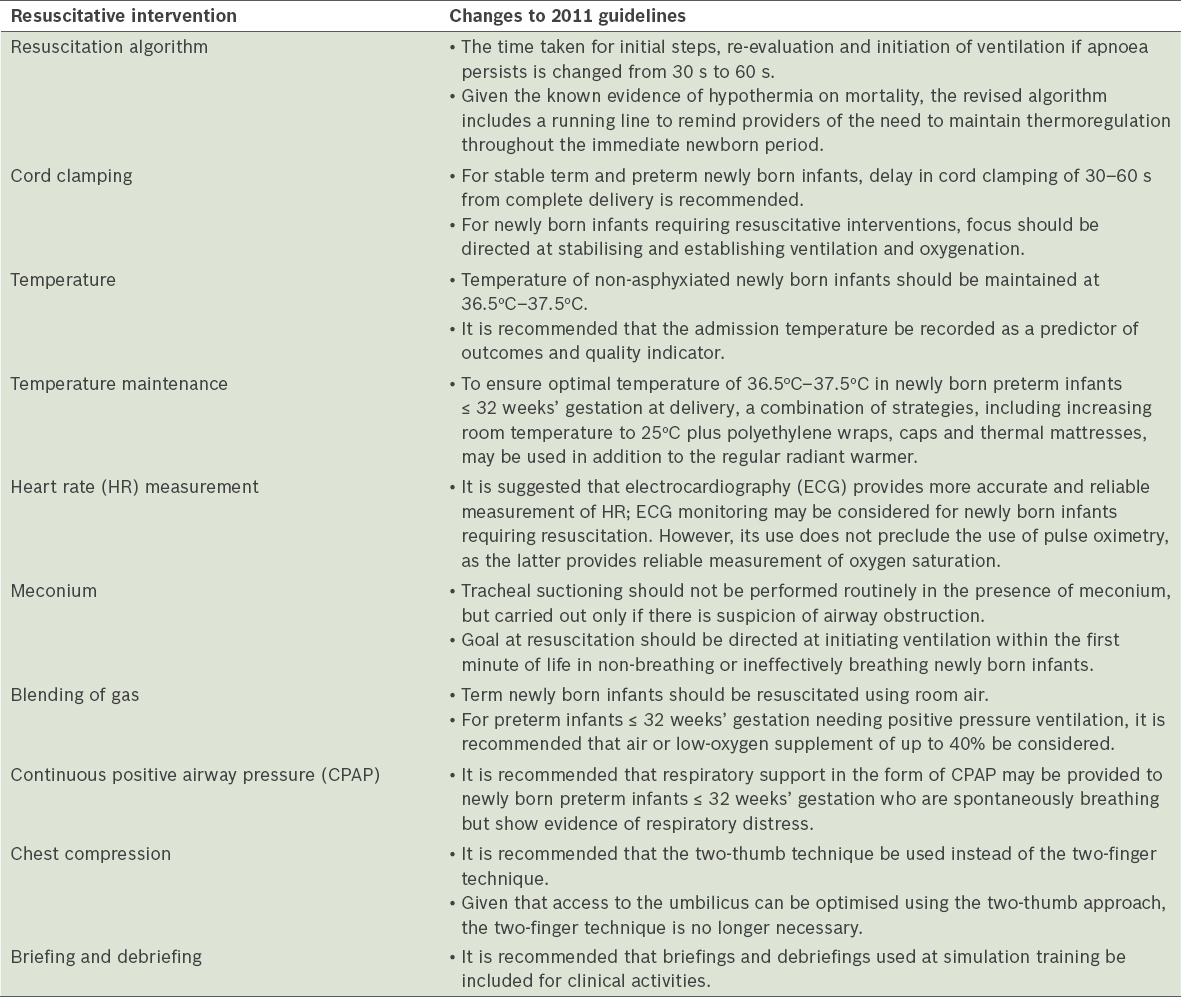
In general, newly born term infants who are vigorous and have regular breathing effort and good tone do not require extra intervention at delivery, and may be left with the mother for routine care. Newly born preterm infants and term infants with poor tone, poor cry or breathing effort need support transitioning from fetal to extrauterine life. The newborn in need of support should be transferred to a radiant warmer to receive one or more of the sequential interventions, viz. initial steps, ventilation and oxygenation, initiation of chest compression and administration of adrenaline and/or volume expansion, if required. The first 60 seconds, also known as the ‘golden minute’, are allocated for provision of the initial steps, re-evaluation of HR and respiration, and to initiate ventilation. Based on the HR and respiration, the newborn may proceed to receive PPV. Once PPV is initiated, re-evaluation is assessed at intervals of 30 seconds using the HR, respiration and oxygen saturation by pulse oximetry, as illustrated in the newborn resuscitation algorithm (Fig. 1). Changes to the 2011 guidelines on resuscitation of newly born infants are summarised and tabulated (Table I).
Summary of changes to the 2011 Newborn and Paediatric Resuscitation Guidelines.(6)
ANTICIPATE NEED AND PREPARE EQUIPMENT
Transition from fetal to extrauterine life is a complex physiological process involving the conversion of placental gas exchange, with intrauterine lungs filled with fluid, to pulmonary respiration with aerated lungs. Approximately 85% of newborn infants born at term have been shown to initiate spontaneous respiration within 10–30 seconds of birth, with an additional 10% responding during drying and stimulation and about 3% initiating respiration after PPV; 2% of newborn infants need intubation to support respiratory function and 0.1% require chest compressions and/or adrenaline.(7-9) Out of 10,114 newly born infants delivered at a local tertiary neonatal centre over a six-year period (2002–2008), 5.9% required PPV, 0.9% required intubation with or without chest compression, and 0.1% required adrenaline and/or volume infusion at delivery. Prematurity was strongly associated with the need for at least PPV at delivery, with the following odds ratio (OR) and 95% confidence interval (CI): newborns < 28 weeks: OR 123.6, 95% CI 68.8–222.1; newborns at 28–33 weeks: OR 12.5, 95% CI 9.7–16.1; and newborns at 34–36 weeks: OR 2.4, 95% CI 1.9–3.1.(10) Besides prematurity, the same study also showed that resuscitation or support of transition is more likely to be needed by newborns with intrapartum evidence of fetal compromise, newborns requiring instrumentation at delivery (inclusive of emergency and elective lower-segment Caesarean section), newborns with meconium-stained liquor, and in cases of antepartum haemorrhage and multiple pregnancies.(10)
As the need for resuscitation at birth is often a predictable event, it is possible to prepare the environment and equipment before delivery. Resuscitation should take place in a warm, well-lit area with a flat resuscitation surface, preferably under a radiant warmer (if in a hospital). Equipment used at delivery should be regularly checked and tested following institutional policy. It is recommended that centres that cater to newborn infants have a written policy on maintenance of resuscitative equipment. In unexpected deliveries occurring in non-designated areas, warm, dry towels may be used to maintain normothermia. Although it is possible to predict the need for resuscitation or stabilisation before a newborn is delivered, this is not always so. Hence, it is recommended that neonatal centres caring for newly born infants have in place policies and procedures to activate and mobilise a team with complete resuscitation skills to meet the unanticipated need for resuscitation of newborns with no apparent risk factors.
Recommendations on equipping and preparing staff in resuscitation
All healthcare workers involved in the care of newborns are encouraged to be trained in neonatal basic life support.
Every birth should be attended to by at least one person whose primary responsibility is to care for the newly born infant. This person should be capable of performing the initial steps of newborn resuscitation and PPV.
In the presence of significant perinatal risk factors, a team with skills in chest compression, intubation and umbilical catheterisation should be mobilised and the team leader identified.
The team should arrive ahead of delivery and, using standardised checklists, ensure that specific equipment and supplies (depending on perinatal risk factors) are present and functioning.
Whenever time permits, the team leader should conduct a preresuscitation briefing, identify interventions that may be required, and assign roles and responsibilities to team members.(4,5)
UMBILICAL CORD MANAGEMENT – DELAYED CORD CLAMPING VERSUS CORD MILKING
Delayed cord clamping
Immediate cord clamping soon after birth is a common practice. However, evidence suggests that there are benefits in DCC at birth, especially for newborn infants who do not require resuscitation.(11) DCC is associated with lower incidence of all grades of intraventricular haemorrhage (IVH), higher systemic blood pressure and volume, lower need for blood transfusion, and lower incidence of necrotising enterocolitis. However, no difference has been demonstrated in severe IVH, mortality, temperature instability and long-term outcomes, although an increase in serum bilirubin associated with a greater need for phototherapy has been noted. This is regardless of gestational age.(1-3)
Recommendations on cord clamping
DCC for 30–60 seconds is recommended for both stable term and preterm newborns who do not require resuscitation at birth. The following should be noted:
Newly born infants who do not require resuscitation should be vigorous, have regular breathing effort and good tone, even if there is a history of meconium-stained amniotic fluid (MSAF).
Newly born infants may be placed at or below the level of the placenta till the umbilical cord is clamped.
Umbilical cord clamping timing should take precedence over cord blood collection for the purpose of cord blood banking.
DCC is contraindicated in deliveries involving monochorionic twins when placental circulation is compromised secondary to placental abruption, bleeding placenta praevia or cord avulsion, and in situations where immediate resuscitation is indicated (e.g. congenital diaphragmatic hernias).
Umbilical cord milking
Umbilical cord milking as an alternative to DCC for newborns with less than 29 weeks’ gestation has generated some interest. Cord milking has been shown to improve blood pressure and haematologic indices, as well as reduce the risk of intracranial haemorrhage. However, no evidence of improved long-term outcomes has been demonstrated.(12-14) The safety profile of this practice is still unknown, particularly the safety of rapid changes in blood volume for extremely preterm newborns. Hence, cord milking cannot yet be recommended as a routine practice. Umbilical cord milking should be restricted to the confines of research.
TEMPERATURE MAINTENANCE AND INITIAL STEPS
Temperature maintenance
Reports have suggested that the admission temperature of newly born non-asphyxiated infants is a strong predictor of mortality for all gestational ages.(15-49) Preterm newborns are especially vulnerable to hypothermia. Serious morbidities associated with hypothermia include increased risk of IVH, respiratory issues, hypoglycaemia and late-onset sepsis. Because of this, ILCOR recommended in 2015 that admission temperature be recorded as a predictor of outcomes and a quality indicator.(3)
Recommendations on thermoregulation
The temperature of newly born non-asphyxiated infants should be maintained at a temperature of between 36.5°C and 37.5°C after birth, through admission and stabilisation. This can be done through the following steps:
Maintain the ambient environment of the delivery suite at 23°C–25°C, where feasible. For delivery of preterm newborns ≤ 32 weeks’ gestation, an ambient temperature ≥ 25°C is preferred.
Dry stable term and preterm newborns ≥ 33 weeks’ gestation immediately after birth. Whenever possible, provide skin-to-skin contact to help maintain body temperature. Cover both the newborn infant and mother with a towel. In situations where delivery occurs unexpectedly out of the delivery area, nursing the newborn skin-to-skin is especially effective in maintaining the newborn’s body temperature.
Unstable term or preterm newborns ≥ 33 weeks’ gestation who require resuscitation should be nursed under a radiant warmer to maintain normothermia.
Newly born infants ≤ 32 weeks’ gestation should have their head and body covered using polyethylene wraps without drying the newborn beforehand, and the newborn should be placed under a radiant warmer. In addition, thermal mattress and caps may be used.
Check the temperature of the newborn – skin, axillary or rectal – before transfer and while maintaining skin-to-skin contact with the mother.
Admission temperature should be recorded soon after stabilisation or resuscitation.
Avoid hyperthermia (temperature > 38°C).
In newly born infants who are unintentionally hypothermic (temperature < 36°C) on admission, current evidence does not support either rapid (≥ 0.5°C/hour) or slow rewarming (< 0.5°C/hour).(50-53) These newborns’ body temperature should be monitored during rewarming to avoid hyperthermia (> 38°C). Studies on newborns delivered to hyperthermic mothers showed increased risk of respiratory depression, neonatal seizures, early death and long-term adverse neurodevelopmental outcome.(54-60)
Initial steps
The initial steps of newborn resuscitation are best performed on a flat resuscitation table under a radiant warmer. The following four action steps should be performed in sequence:
Maintain normal temperature of the newly born infant.
Place the newly born infant flat with the neck in a neutral, ‘sniffing’ position to open the airway (Fig. 2).
Fig. 2
Photograph shows the ‘sniffing’ position to maintain airway patency.
Clear secretions, if needed, with a bulb syringe or a 10F–12F suction catheter using a suction pressure of 80–100 mmHg.
Dry the newly born infant (replace with polyethylene wrap in preterm newborns ≤ 32 weeks’ gestation) and stimulate the newborn to breathe. Avoid overstimulation.
Newly born infants who are vigorous and have regular breathing effort and good tone require only drying and wrapping in a warm towel. These newborns can continue to be kept warm through skin-to-skin contact with their mothers. Newborns may begin to breastfeed at this stage. It is important to monitor the body temperature of the newborns to ensure normothermia while maintaining their skin-to-skin contact with their mothers.
If a newly born infant is unable to establish spontaneous effective breathing or has a HR < 100 beats per minute (bpm) following stimulation, newborn life support is needed (Fig. 1). Ventilation is the most important step for the successful resuscitation of newborns who have not responded to the initial steps. The golden minute (60-second) mark for completing the initial steps, re-evaluating and beginning ventilation (if required) replaces the 30-second rule in the previous algorithm.(1-3) The recommendation to complete the initial steps in 30 seconds in the previous algorithm was not evidence-based, and it was felt that more time should be given to support newborns in transiting to extrauterine life. The golden minute emphasises the importance of avoiding unnecessary delay in the initiation of ventilation.
Clearing the airway
There is no need for routine suctioning of the oropharynx. Aggressive suctioning can cause laryngeal spasm and vagal bradycardia; hence, gentle suctioning is needed only if there is evidence of airway obstruction, or prior to endotracheal intubation.(61-63)
Management of newborns with meconium-stained liquor
Routine intrapartum oropharyngeal and nasopharyngeal suctioning of newly born infants who are born through MSAF before delivery of the shoulders does not prevent meconium aspiration syndrome. In healthy newborns, suctioning of the mouth and nose has been associated with cardiorespiratory complications. Thus, routine intrapartum oropharyngeal and nasopharyngeal suctioning of newly born infants who are born with clear amniotic fluid or MSAF is not recommended and strongly discouraged. Gentle clearing of the meconium from the mouth and nose should be reserved for newly born infants who have obvious obstruction to spontaneous breathing or require PPV.(3) For newborns with respiratory depression delivered through MSAF, routine intubation for tracheal suctioning is no longer recommended.(3) There is insufficient evidence to continue recommending this practice. The emphasis should be made on initiating ventilation within the first minute of life in non-breathing or ineffectively breathing newly born infants. Only when there is visible obstruction during PPV should intubation and suction be considered.
Recommendations on suctioning of airway
When amniotic fluid is clear, intrapartum oropharyngeal suctioning (including suctioning with a bulb syringe) is not recommended.
For vigorous newly born infants who are born through MSAF, intrapartum oropharyngeal suctioning is not recommended. Gentle clearing of the meconium from the mouth and nose with a bulb syringe may be done for those with obvious obstruction to spontaneous breathing.
For non-vigorous newly born infants born through MSAF, routine direct oropharyngeal and tracheal suctioning is no longer recommended. The initial steps of resuscitation performed under a radiant warmer should be performed in these newborns. Clear the oropharynx by suctioning with a 10F–12F catheter using a suction pressure of 80–100 mmHg. Initiate PPV if the newborn infant is not breathing or when HR is < 100 bpm after completion of the initial steps of resuscitation. If there is visible obstruction during PPV, consider tracheal suctioning.
DETECTION OF HEART RATE: COMPARING ECG WITH OXIMETRY OR AUSCULTATION
Immediately after birth, the HR is assessed to evaluate the condition of the newly born infant and determine the need for escalation of care. An increase in HR is an indicator of successful resuscitative intervention. Rapid and accurate assessment of HR is of critical importance. Umbilical cord palpation may not be accurate, particularly if the HR is < 100 bpm.(64) Auscultation of the precordium has been proposed as the preferred method, supplemented by the use of pulse oximetry, which provides continuous measure of the peripheral pulse. Emerging evidence has suggested that three-lead ECG displays HR faster than pulse oximetry, without difficulty in applying the leads.(65-68) The applicability of this tool needs further exploration in regular clinical practice.
Recommendations on assessment of heart rate
Auscultation is recommended for clinical assessment of HR. However, if a stethoscope is not available, umbilical cord palpation may be used.
It is suggested that three-lead ECG may be considered for continuous assessment of HR during chest compressions. However, the use of ECG does not replace the need for pulse oximetry to evaluate the newborn’s oxygenation.(65-69)
OXYGEN ADMINISTRATION AND CONTINUOUS POSITIVE AIRWAY PRESSURE
Oxygen administration
Oxygen use in term and preterm newborns was last reviewed in 2010.(4,5) In term newborns receiving resuscitation with intermittent PPV, 100% oxygen was found to confer no advantage over air in the short term, and resulted in increased time to first breath, cry or both. Two meta-analyses of studies comparing term newborns receiving resuscitation with intermittent PPV initiated with room air vs. 100% oxygen showed a decrease in mortality for the former group.(70,71) Based on systematic reviews conducted by ILCOR in 2010, blended gas was recommended in resuscitation of preterm newborns, although the optimal oxygen concentration for these newborns was not clearly defined.
A meta-analysis of seven randomised trials comparing initiating resuscitation of preterm newborns (< 35 weeks’ gestation) with high oxygen (≥ 65%) and low oxygen (21%–30%) concentrations showed no improvement in survival to hospital discharge with the use of high oxygen concentrations.(2) In a subset of studies that evaluated these outcomes, no benefit was seen for the prevention of bronchopulmonary dysplasia, IVH or retinopathy of prematurity.(2) In all studies, irrespective of whether air or high oxygen concentration (including 100%) was used to initiate resuscitation, most newborns were breathing approximately 30% oxygen by the time of stabilisation.(2) Initiating resuscitation of preterm newborns with high oxygen concentrations is not recommended so as to avoid exposing preterm newborns to additional oxygen, as no current data has demonstrated any proven benefits for important outcomes. Therefore, resuscitation of preterm newborns should be initiated with low oxygen concentrations. In circumstances where blenders are not readily available, adaptations may be adopted to deliver supplemental oxygen of up to 40%.
Recommendations on the use of supplemental oxygen
For preterm newborns ≤ 32 weeks’ gestation, resuscitation should be initiated at 21%–40% oxygen concentration. For newborns ≥ 33 weeks’ gestation, resuscitation should be initiated at 21% oxygen. Supplemental oxygen should be titrated as per guidelines based on the preductal oxygen saturation (SpO2) (Fig. 1).
If a newborn is breathing but SpO2 is not within the target range, supplemental oxygen of 30%–40% at a flow rate of 10 L/minute may be delivered. Using the blender, adjust oxygen concentration to achieve preductal SpO2 targets.
If a newborn has laboured breathing, or SpO2 cannot be maintained despite 100% oxygen, a trial of CPAP may be considered.
Continuous positive airway pressure
Three randomised controlled trials (RCTs) involving 2,358 newly born infants delivered at < 30 weeks’ gestation have demonstrated that CPAP, as compared with PPV, reduces the rate of intubation and duration of mechanical ventilation with no significant short-term disadvantage.(72-74) It was recommended that the initial respiratory support for spontaneously breathing preterm newborns may be provided by CPAP rather than intubation. CPAP may be delivered through a face mask or nasal prong interface. Data on the use of CPAP in term newborns is scanty, and appropriate use of this interface is driven by the clinical status and needs of individual term newborns.(75,76)
Recommendations on the use of CPAP
Spontaneously breathing premature newborns ≤ 32 weeks’ gestation may be safely stabilised with CPAP at approximately 5 cmH2O in the delivery room and during transfer, instead of with elective intubation. The need for intubation and surfactant administration should be determined based on institutional policies.
For newborn infants ≥ 33 weeks’ gestation, CPAP at 5 cmH2O may be considered if clinically indicated.
POSITIVE PRESSURE VENTILATION AND POSITIVE END-EXPIRATORY PRESSURE
Positive pressure ventilation
If breathing efforts are absent or inadequate, lung aeration must not be delayed. PPV can be effectively delivered with a flow-inflating bag, self-inflating bag or T-piece resuscitator. The benefits of sustained inflation of > 5 seconds’ duration in reducing the need for mechanical ventilation were evident in three RCTs and two cohort studies.(77-81) No benefit was found for critical outcomes such as reduction of mortality, bronchopulmonary dysplasia or air leak.(2) One cohort study suggested that the need for intubation was less after sustained inflation.(1) However, there is insufficient data about the safety and method of application of sustained inflation for the transitioning newborn. Hence, the routine use of sustained inflation is not recommended.
The pressure required to aerate fluid-filled lung averages 20 cmH2O (range 15–30 cmH2O).(82,83) Efficacy of ventilation can be estimated by a prompt increase in HR and by observing for chest rise. If these are not achieved, then the airway and/or mask should be repositioned and the inflation pressure increased, if required. Most newborns would respond within 30 seconds of lung inflation.
If HR rises to > 100 bpm but the newborn is not breathing spontaneously, then ventilation should be continued at 40–60 breaths/minute until regular spontaneous breathing is established. In situations where HR fails to respond, possible causes include inadequate airway control or ventilation secondary to mask leak, inappropriate airway position and airway obstruction. Consider taking corrective steps (MR SOPA), which includes: mask repositioning to correct for mask leak, repositioning of the newborn’s head to achieve ‘sniffing’ position, suctioning to clear possible airway obstruction, opening of the mouth, increasing of ventilatory pressure to achieve chest rise, and alternative airway such as endotracheal intubation or laryngeal mask.
Without adequate ventilation, chest compression will not be effective; hence, it is important to ensure adequate lung aeration and ventilation before progressing to circulatory support. Continue ventilation until the newborn has established normal regular breathing.
Positive end-expiratory pressure
Two RCTs have suggested that the addition of PEEP during delivery room resuscitation of preterm newborns did not result in improvement in mortality, HR, need for cardiac drugs, chest compressions or intubation, pulmonary air leaks, chronic lung disease, and Apgar scores, although the studies were too underpowered to have sufficient confidence in a no-difference conclusion.(2) However, considering the evidence from animal studies and another trial that provided low-quality evidence that the maximum amount of supplementary oxygen required to achieve target SpO2 may be slightly lower when using PEEP, it has been suggested that PEEP ventilation should be used in premature newborns during delivery room resuscitation.(4,5)
Recommendations for effective PPV
The decision for PPV is determined by simultaneous assessment of respiration (apneoa, gasping or laboured breathing) and HR (< 100 bpm).
For newly born infants requiring PPV, inspiratory pressure should be initiated at about 20–25 cmH2O while assessing for adequate ventilation and response. The inflation pressure should be monitored and increased, when required.
The routine use of initial sustained inflation (> 5 seconds’ duration) is not recommended.
For preterm newborns ≤ 32 weeks’ gestation requiring PPV, PEEP of about 5 cmH2O is suggested. For newborns ≥ 33 weeks requiring PPV, PEEP ventilation can be considered, if resources are available.
Assisted ventilation should be delivered at a rate of 40–60 breaths per minute till normal regular breathing is established.
Once PPV is started, the assessment of the newborn should consist of simultaneous evaluation of HR, respiration and SpO2.
ENDOTRACHEAL INTUBATION AND LARYNGEAL MASK AIRWAY
Endotracheal intubation
Tracheal intubation may be considered at several time points during neonatal resuscitation. However, the procedure of intubation is a skill that is difficult to master and teach. Timing of tracheal intubation is dependent on the availability of a skilled resuscitator. Tube size to use and depth to insert is based on gestational age and/or estimated weight of the newborn at birth (Table II). Vocal cord guide on endotracheal tube (ETT) is only an approximation and may not reliably indicate the correct insertion depth. Tube position must be confirmed using chest radiography.
Table II
Endotracheal tube (ETT) size and depth of tube placement (oral intubation).
Exhaled carbon dioxide detection remains the most reliable method for confirmation of ETT placement.(84-87) The absence of detectable carbon dioxide suggests orogastric intubation, whereas cardiac arrest and tracheal obstruction may result in false negatives.(84,86) Additional clinical indicators of correct ETT placement include chest movement, equal breath sounds bilaterally and condensation of the ETT, and their routine use should be continued. Following endotracheal intubation and the delivery of effective ventilation, a prompt increase in HR is the best indicator that the tube is in the trachea.(88)
Recommendations for endotracheal intubation
Endotracheal intubation may be considered:
When bag-mask ventilation is ineffective or prolonged.
When suctioning the lower airway to remove presumed tracheal obstruction.
When chest compressions are performed.
In special circumstances such as congenital diaphragmatic hernia or to instil surfactant.
Select the appropriate tube size and determine the length of tube to insert (Table II).
Check position to confirm appropriate placement.
Laryngeal mask airway
The ability to secure an airway when face-mask ventilation fails is a critical determinant of successful resuscitation. The LMA has been proposed as an alternative, either as a primary device, replacing face-mask ventilation, or as a secondary device when intubation fails or is not feasible.
Three RCTs, which enrolled a total of 469 term newborns and compared the use of LMA to the face mask as a primary device, showed that LMA was more effective than face-mask ventilation in achieving vital signs and delivering adequate ventilation with no evidence of increased morbidities such as vomiting or gastric distension.(89-91)
For comparison of LMA to ETT as a secondary device (i.e. LMA or intubation when bag-mask ventilation has failed) for term newborns requiring PPV for resuscitation, one RCT involving 40 term newborns showed that LMA was as effective as endotracheal intubation in achieving vital signs or successful resuscitation.(92) The use of LMA resulted in lower risk of trauma to the soft tissue compared with endotracheal intubation.
While studies have proven the safety and feasibility of the LMA device as an alternative to endotracheal intubation in late-preterm and term newborns (≥ 34 weeks’ gestation), more studies are needed on its use for newborns that are more premature.
Recommendations on the use of LMA
LMA may be used as an alternative to tracheal intubation during resuscitation of late-preterm and term newborns (≥ 34 weeks’ gestation) if ventilation via face mask is unsuccessful.
Where intubation is not feasible or unsuccessful after failed PPV, LMA is recommended for resuscitation of late-preterm and term newborns (≥ 34 weeks’ gestation).
CHEST COMPRESSION
Circulatory support with chest compression is effective only if the lungs are sufficiently inflated. Begin chest compression when HR is < 60 bpm after at least 30 seconds of effective ventilation, preferably via an ETT/LMA. The two-thumb technique, with both thumbs over the lower third of the sternum and fingers encircling the torso and supporting the newborn’s back, is preferred (Fig. 3). The technique generates higher blood pressure, leading to improved perfusion and gas exchange during cardiopulmonary resuscitation (CPR), as well as less fatigue than the two-finger technique.(93-101)Once the ETT/LMA is secured, the two-thumb technique can be delivered effectively from the head of the bed, while the umbilicus is accessed for insertion of an umbilical catheter; hence, the two-finger technique is no longer recommended.
Fig. 3
Photograph shows the two-thumb compression technique. Note the positioning of the thumbs and fingers in this technique.
The compression rate of 3:1 ventilation recommended for newborns with cardiovascular collapse results in a total of 120 events per minute (i.e. 90 compressions to 30 ventilations). Animal studies on higher compression-to-ventilation ratios compared to the current 3:1 ratio showed no improvement in short-term survival, gas exchange during CPR, time to recovery of spontaneous circulation (ROSC) and markers of tissue injury.(102-106) In addition, manikin studies have shown disadvantages in higher ratios for compressor fatigue and minute ventilation.(107) Quality of compressions and breaths are as important, if not more important, than the compression rates. The chest should be allowed to re-expand fully during relaxation, but the rescuer’s thumb should not leave the chest. Effective coordination of compression and ventilation is recommended to avoid simultaneous delivery. Since hypoxia is the predominant cause of cardiovascular collapse in the newborn, effective resuscitation requires significant focus on ventilation. It is recommended that a 3:1 compression-to-ventilation ratio be retained for neonatal CPR.(1-3)
By the time the resuscitation of a newborn infant has reached the stage of chest compression, efforts to achieve ROSC using effective ventilation with low-concentration oxygen should have been attempted. Thus, it would appear sensible to increase the supplementary oxygen concentration to 100% at the initiation of chest compression. However, there are no human studies to support this, and animal studies have shown that 100% oxygen during CPR had no advantage.(108-114)
Coordinated chest compression and ventilation with oxygen at 100% for 60 seconds should be continued before HR, respiration and SpO2 are rechecked. If HR is > 60 bpm, stop chest compression but continue PPV at a rate of 40–60 breaths per minute. If HR is > 100 bpm and the newborn is breathing spontaneously, slowly withdraw PPV. If the newborn is not responding and HR remains at < 60 bpm, review the adequacy of ventilation, supplementary oxygen, depth of chest compression, and coordination of compressions and ventilations.
Recommendations for synchronised CPR
Begin chest compressions when HR is < 60 bpm after at least 30 seconds of effective ventilation, preferably via an ETT/LMA.
Increase supplementary oxygen to 100%.
Apply the two-thumb technique by encircling the newborn’s torso with both hands and placing both thumbs side by side, or over one another if the newborn is small. Compress the lower third of the sternum using the thumbs, with the fingers supporting the newborn’s back.
Depress the sternum about one-third of the anteroposterior diameter of the chest and release to allow chest recoil and ventilation.
Ensure coordinated compressions and ventilation at a ratio of 3:1.
Continue chest compressions for 60 seconds before rechecking HR, respiration and SpO2.
MEDICATIONS
Drugs are rarely indicated in resuscitation. Inadequate lung inflation and extreme hypoxaemia are common causes for bradycardia in newly born infants. The most effective intervention to correct bradycardia is adequate ventilation. If HR remains at < 60 bpm despite at least 30 seconds of adequate ventilation and another 60 seconds of adequate ventilation with 100% oxygen and coordinated chest compression, administration of adrenaline or volume, or both is indicated.
Recommendations on the use of adrenaline
Intravenous adrenaline is preferred. Tracheal route should be avoided, where possible. There is no safety or efficacy data on high tracheal doses.
Adrenaline (1:10,000) at 0.1–0.3 mL/kg (intravenous) should be administered rapidly followed by 0.5–1.0 mL of saline flush.(1,3-5) If the intravenous route is not available, the endotracheal route at 0.5–1.0 mL/kg may be used.(4,5,9,115-120) If indicated, administration should be repeated via the intravenous route once umbilical venous or intraosseous access is established. There is no need to wait 3–5 minutes after the ETT dose.
Continue coordinated chest compression and ventilation following administration of adrenaline and assess its effect by measuring HR 60 seconds after the administration.
Intravenous adrenaline may be repeated at 3–5 minutes interval, if indicated.
Recommendations on the use of volume expansion
Consider volume expansion if blood loss is known or suspected, and HR has not responded to previous resuscitative intervention.(121)
Umbilical venous access is recommended.
Isotonic fluid such as 0.9% normal saline or type-O Rh-negative blood at 10 mL/kg may be administered intravenously.
Infuse predetermined volume over 10–15 minutes. Avoid rapid infusion in preterm newborns. Large volumes given rapidly to preterm newborns have been associated with IVH.
Repeat infusion may be given, if indicated.
Recommendations on the use of sodium bicarbonate and naloxone
There is currently no evidence to support the routine use of sodium bicarbonate infusion in newborns with metabolic acidosis.
The safety and efficacy of naloxone in newborns with respiratory depression born to mothers exposed to opiate remains uncertain. Animal studies and case reports highlighted complications such as pulmonary oedema, cardiac arrest and seizures with the use of naloxone.(122,123)
POST-RESUSCITATION CARE
Newly born infants may deteriorate following initial stabilisation after resuscitative intervention. These newborns should be monitored in an environment where anticipatory care is available.
Glucose control
Hypoglycaemia is associated with poor neurological outcome.(124) One clinical study demonstrated an association between hypoglycaemia and poor neurological outcome following perinatal asphyxia.(125) While hyperglycaemia in children following hypoxic ischaemia does not appear to result in harm, the range of blood glucose concentration that is associated with the least brain injury following asphyxia cannot be defined.
Recommendations for optimal glucose control
It is recommended that serum glucose should be monitored after resuscitation.(4,5)
Early parenteral nutrition should be provided to prevent hypoglycaemia, and hypoglycaemia should be corrected once it is detected.
Therapeutic hypothermia for moderate or severe hypoxic ischaemic encephalopathy
The 2010 ILCOR systematic review recommended that term or near-term newborns (> 36 weeks’ gestation) with moderate to severe hypoxic ischaemic encephalopathy (HIE) should be offered therapeutic hypothermia (33.5°C–34.5°C) within six hours, if possible. In 2015, ILCOR suggested that the use of therapeutic hypothermia in resource-limited settings may be considered and offered to newborns of > 36 weeks’ gestation with evolving moderate-to-severe HIE, but the procedure should be performed under clearly defined protocols similar to those used in published clinical trials and in facilities with capabilities for multidisciplinary care and longitudinal follow-up.(4,5)
Recommendation on management of moderate or severe HIE
Therapeutic hypothermia should be offered to eligible newborns, and the procedure must be performed in accordance with clearly defined protocols at centres with capabilities for multidisciplinary care and longitudinal follow-up.
WITHHOLDING RESUSCITATION AND DISCONTINUING RESUSCITATIVE EFFORTS
Withholding resuscitation
The 2010 ILCOR guideline suggested that when gestation, birth weight or congenital anomalies are associated with an almost certain early death and when unacceptably high morbidity is likely among the rare survivors, resuscitation is not indicated. In conditions associated with uncertain prognosis, when there is borderline survival with a high rate of morbidity and high burden to the child, the parents’ views on resuscitation should be supported.(4,5) Studies have indicated that parents desire a larger role in decisions to resuscitate and continue life support in severely compromised infants.(126,127)
Recommendations on withholding resuscitation
In deliveries at a confirmed gestational age of < 23 weeks’ gestation or where known congenital anomalies are associated with an almost certain early death and unacceptably high morbidity among the rare survivors (e.g. anencephaly, Bart’s hydrops, Trisomy 13, Trisomy 18), initiation of resuscitation is not an ethical treatment option and should not be offered.
When antenatally identified conditions are associated with high mortality and poor outcome, the physician responsible should discuss the risks and benefits of life-sustaining treatment and allow the parents to participate in the decision on whether attempting resuscitation is in their newborn’s best interest. If it is jointly agreed that intensive care will not improve the chance of the newborn’s survival or will pose an unacceptable burden for the newborn, it is ethical to provide compassionate palliative care and not initiate resuscitation.
In deliveries at borderline viability of 23–24 weeks’ gestation, therapeutic options and prognosis must be discussed with the parents before delivery, when feasible, and a combined decision on the resuscitative approach arrived at prior to delivery. In these situations, a consistent and coordinated approach to individual cases by the obstetric and neonatal teams is recommended.
Where the parents are uncertain or when a combined decision (between the parents and physician) has not been reached at the time of delivery, maximal resuscitation should still be provided.
Further critical care intervention and decision to withdraw should be based on response to resuscitation.
Discontinue resuscitative intervention
Apgar score of 0 at ten minutes is a strong predictor of mortality and morbidity in late-preterm and term newborns. It is suggested that when HR remains undetectable after ten minutes of effective resuscitation, cessation of resuscitation is considered reasonable.(1-5) However, the decision should be individualised.
Recommendations on resuscitative intervention
In newborns with an Apgar score of 0 after ten minutes of continuous, effective resuscitation, it may be reasonable to stop assisted ventilation if HR remains undetectable.
The decision to continue or discontinue resuscitative efforts must be individualised according to certain factors, including specific circumstances before delivery (e.g. known timing of insult), whether the resuscitation was considered optimal, and prior understanding of parental views on acceptable morbidities.(128,129)
BRIEFING AND DEBRIEFING
Studies on the effects of debriefs before and after resuscitation have shown improvement in subsequent performance in simulation settings.(130-135) A structured analysis of perinatal management with feedback showed reduction in the incidence of IVH in preterm newborns.(136) Debrief after resuscitation is performed for the purposes of reflective learning and practice improvement in some local neonatal centres.
Recommendations on briefing and debriefing
Whenever possible, the team should discuss and assign responsibilities to individual team members prior to the start of resuscitation.
The resuscitation team is encouraged to conduct a debrief to reflect on the steps of resuscitation and provide constructive feedback at the end of resuscitation.
TRAINING IN NEONATAL RESUSCITATION
Training of providers
The use of simulation in teaching neonatal resuscitation was recommended in the 2010 ILCOR guideline. Studies evaluating the frequency of training of healthcare providers in neonatal resuscitation showed no difference in patient outcomes but some advantages in psychomotor performance, knowledge and confidence when focused training occurred every six months or more frequently.(137-153) The 2015 ILCOR systematic review suggested that neonatal resuscitation task training occurs more frequently than the current two-year interval.(1,2)
Recommendation on retraining of providers
Considering the time, manpower constraints and cost of training, it is suggested that individual providers seek recurrent focused retraining on specific tasks and/or skills at two-yearly intervals or more depending on their needs.
Training of instructors
The best instructor training methodology remains unclear. Studies exploring the impact of preparation of instructors for training of healthcare providers showed no association between the preparation provided and instructor or learner performance.(154-160) The 2015 ILCOR systematic review suggested that training of resuscitation instructors incorporate timely, objective, structured, individually targeted verbal and/or written feedback.(1,2)
Recommendations on educating and retraining of instructors
Enhance instructors’ skills through hands-on training opportunities, with a debrief on their teaching performance at the end of each training session.
To maintain instructorship, each instructor has to teach a minimum of three workshops over two years and refresh their knowledge through completion of e-lessons on neonatal resuscitation and online multiple choice questions once every two years.
It is suggested that instructors consider attending at least one educational course, conference or local instructor update session once every two years.
CONCLUSION
The science and practice of neonatal resuscitation will continue to improve through ongoing studies that evaluate the outcomes of resuscitative interventions, and research on the available feedback devices to guide and fine-tune resuscitation. The consensus on Singapore neonatal resuscitation has been achieved following repeated discussions and debate on the ILCOR neonatal guidelines and recommendations, as well as with better understanding of local practice and needs. The Singapore Neonatal Resuscitation Guidelines 2016 represents the widely accepted view of how resuscitation of newly born infants in need of support can be carried out safely and effectively.
ACKNOWLEDGEMENTS
The authors thank Prof Venkataraman Anantharaman, Chairman, National Resuscitation Council, Singapore, and Senior Consultant, Department of Emergency Medicine, Singapore General Hospital; and Dr Bharadwaj Srabani, Consultant, Department of Neonatal and Developmental Medicine, Singapore General Hospital, for their contributions to the reviews contained in this guideline paper.
References Perlman JM, Wyllie J, Kattwinkel J, et al. Neonatal Resuscitation Chapter CollaboratorsPart 7:Neonatal Resuscitation:2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations.Circulation. 2015;132:16 Suppl 1204-41. Wyckoff MH, Aziz K, Escobedo MB, et al. Part 13:Neonatal Resuscitation:2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.Circulation. 2015;132:18 Suppl 2543-60. Wyllie J, Perlman JM, Kattwinkel J, et al. Neonatal Resuscitation Chapter CollaboratorsPart 7:Neonatal resuscitation:2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations.Resuscitation. 2015;95:169-201. Perlman JM, Wyllie J, Kattwinkel J, et al. Neonatal Resuscitation Chapter CollaboratorsPart 11:Neonatal resuscitation:2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations.Circulation. 2010;122:16 Suppl 2516-38. Wyllie J, Perlman JM, Kattwinkel J, et al. Neonatal Resuscitation Chapter CollaboratorsPart 11:Neonatal resuscitation:2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations.Resuscitation. 2010;81:Suppl 1260-87. Singapore National Resuscitation Council’s Neonatal and Paediatric Resuscitation WorkgroupChong NK.Newborn and paediatric resuscitation 2011 guidelines.Singapore Med J. 2011;52:560-72. Ersdal HL, Mduma E, Svensen E, Perlman JM.Early initiation of basic resuscitation interventions including face mask ventilation may reduce birth asphyxia related mortality in low-income countries:a prospective descriptive observational study.Resuscitation. 2012;83:869-73. Perlman JM, Risser R.Cardiopulmonary resuscitation in the delivery room. Associated clinical events.Arch Pediatr Adolesc Med. 1995;149:20-5. Barber CA, Wyckoff MH.Use and efficacy of endotracheal versus intravenous epinephrine dang neonatal cardiopulmonary resuscitation in the delivery room.Pediatrics. 2006;118:1028-34. Wong CY, Yeo CL.Resuscitation of the newborn in Singapore General Hospital:how often is it required, what factors predict the need for resuscitation at birth, and what are the outcomes?.Poster abstract at PSANZ. 2010;. McDonald SJ, Middleton P, Dowswell T, Morris PS.Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes.Cochrane Database Syst Rev. 2013;CD004074. Hosono S, Mugishima H, Fujita H, et al. Umbilical cord milking reduces the need for red cell transfusions and improves neonatal adaptation in infants born at less than 29 weeks’gestation:a randomised controlled trial.Arch Dis Child Fetal Neonatal Ed. 2008;93:F14-9. Katheria AC, Leone TA, Woelkers D, et al. The effects of umbilical cord milking on hemodynamics and neonatal outcomes in premature neonates.J Pediatr. 2014;164:1045-1050.e1. March MI, Hacker MR, Parson AW, Modest AM, de Veciana M.The effects of umbilical cord milking in extremely preterm infants:a randomized controlled trial.J Perinatol. 2013;33:763-7. Budin P. The Nursling:the Feeding and Hygiene of Premature and Full-term Infants. 1907;London Caxton Publishing Co. A Abd-El Hamid S, Badr-El Din MM, Dabous NI, Saad KM.Effect of the use of a polyethylene wrap on the morbidity and mortality of very low birth weight infants in Alexandria University Children’s Hospital.J Egypt Public Health Assoc. 2012;87:104-8. Acolet D, Elbourne D, McIntosh N, et al. Confidential Enquiry Into Maternal and Child HealthProject 27/28:inquiry into quality of neonatal care and its effect on the survival of infants who were born at 27 and 28 weeks in England, Wales, and Northern Ireland.Pediatrics. 2005;116:1457-65. Bateman DA, O’Bryan L, Nicholas SW, Heagarty MC.Outcome of unattended out-of-hospital births in Harlem.Arch Pediatr Adolesc Med. 1994;148:147-52. Bhoopalam PS, Watkinson M.Babies born before arrival at hospital.Br J Obstet Gynaecol. 1991;98:57-64. Boo NY, Guat-Sim Cheah I.Malaysian National Neonatal RegistryAdmission hypothermia among VLBW infants in Malaysian NICUs.J Trop Pediatr. 2013;59:447-52. Buetow KC, Klein SW.Effects of maintenance of “normal”skin temperature on survival of infants of low birth weight.Pediatrics. 1964;34:163-70. Costeloe K, Hennessy E, Gibson AT, Marlow N, Wilkinson AR.The EPICure study:outcomes to discharge from hospital for infants born at the threshold of viability.Pediatrics. 2000;106:659-71. Costeloe KL, Hennessy EM, Haider S, et al. Short term outcomes after extreme preterm birth in England:comparison of two birth cohorts in 1995 and 2006 (the EPICure studies).BMJ. 2012;345:e7976. da Mota Silveira SM, Gonçalves de Mello MJ, de Arruda Vidal S, de Frias PG, Cattaneo A.Hypothermia on admission:a risk factor for death in newborns referred to the Pernambuco Institute of Mother and Child Health.J Trop Pediatr. 2003;49:115-20. Daga AS, Daga SR, Patole SK.Determinants of death among admissions to intensive care unit for newborns.J Trop Pediatr. 1991;37:53-6. de Almeida MF, Guinsburg R, Sancho GA, et al. Brazilian Network on Neonatal ResearchHypothermia and early neonatal mortality in preterm infants.J Pediatr. 2014;164:271-5.e1. García-Muñoz Rodrigo F, Rivero Rodríguez S, Siles Quesada C.[Hypothermia risk factors in the very low weight newborn and associated morbidity and mortality in a neonatal care unit].An Pediatr (Barc). 2014;80:144-50. Spanish. Harms K, Osmers R, Kron M, et al. [Mortality of premature infants 1980-1990:analysis of data from the Göttingen perinatal center].Z Geburtshilfe Perinatol. 1994;198:126-33. German. Hazan J, Maag U, Chessex P.Association between hypothermia and mortality rate of premature infants--revisited.Am J Obstet Gynecol. 1991;164:1 Pt 1111-2. Jones P, Alberti C, Julé L, et al. Mortality in out-of-hospital premature births.Acta Paediatr. 2011;100:181-7. Kalimba EM, Ballot DE.Survival of extremely low-birth-weight infants.S Afr J Child Health. 2013;7:13-6. Kambarami R, Chidede O.Neonatal hypothermia levels and risk factors for mortality in a tropical country.Cent Afr J Med. 2003;49:103-6. Kent AL, Williams J.Increasing ambient operating theatre temperature and wrapping in polyethylene improves admission temperature in premature infants.J Paediatr Child Health. 2008;44:325-31. Laptook AR, Salhab W, Bhaskar B.Neonatal Research NetworkAdmission temperature of low birth weight infants:predictors and associated morbidities.Pediatrics. 2007;119:643-9. Lee HC, Ho QT, Rhine WD.A quality improvement project to improve admission temperatures in very low birth weight infants.J Perinatol. 2008;28:754-8. Levi S, Taylor W, Robinson LE, Levy LI.Analysis of morbidity and outcome of infants weighing less than 800 grams at birth.South Med J. 1984;77:975-8. Manani M, Jegatheesan P, DeSandre G, et al. Elimination of admission hypothermia in preterm very low-birth-weight infants by standardization of delivery room management.Perm J. 2013;17:8-13. Manji KP, Kisenge R.Neonatal hypothermia on admission to a special care unit in Dar-es-Salaam, Tanzania:a cause for concern.Cent Afr J Med. 2003;49:23-7. Mathur NB, Krishnamurthy S, Mishra TK.Evaluation of WHO classification of hypothermia in sick extramural neonates as predictor of fatality.J Trop Pediatr. 2005;51:341-5. Miller SS, Lee HC, Gould JB.Hypothermia in very low birth weight infants:distribution, risk factors and outcomes.J Perinatol. 2011;31:Suppl 1S49-56. Mullany LC, Katz J, Khatry SK, et al. Risk of mortality associated with neonatal hypothermia in southern Nepal.Arch Pediatr Adolesc Med. 2010;164:650-6. Nayeri F, Nili F.Hypothermia at birth and its associated complications in newborns:a follow-up study.Iran J Public Health. 2006;35:48-52. Obladen M, Heemann U, Hennecke KH, Hanssler L.[Causes of neonatal mortality 1981-1983:a regional analysis].Z Geburtshilfe Perinatol. 1985;189:181-7. German. Ogunlesi TA, Ogunfowora OB, Adekanmbi FA, Fetuga BM, Olanrewaju DM.Point-of-admission hypothermia among high-risk Nigerian newborns.BMC Pediatr. 2008;8:40. Pal DK, Manandhar DS, Rajbhandari S, et al. Neonatal hypoglycaemia in Nepal 1. Prevalence and risk factors.Arch Dis Child Fetal Neonatal Ed. 2000;82:F46-51. Shah S, Zemichael O, Meng HD.Factors associated with mortality and length of stay in hospitalised neonates in Eritrea, Africa:a cross-sectional study.BMJ Open. 2012;2:e000792. Singh A, Yadav A, Singh A.Utilization of postnatal care for newborns and its association with neonatal mortality in India:an analytical appraisal.BMC Pregnancy Childbirth. 2012;12:33. Sodemann M, Nielsen J, Veirum J, et al. Hypothermia of newborns is associated with excess mortality in the first 2 months of life in Guinea-Bissau, West Africa.Trop Med Int Health. 2008;13:980-6. Stanley FJ, Alberman EV.Infants of very low birthweight. I:Perinatal factors affecting survival.Dev Med Child Neurol. 1978;20:300-12. Motil KJ, Blackburn MG, Pleasure JR.The effects of four different radiant warmer temperature set-points used for rewarming neonates.J Pediatr. 1974;85:546-50. Tafari N, Gentz J.Aspects of rewarming newborn infants with severe accidental hypothermia.Acta Paediatr Scand. 1974;63:595-600. Racine J, Jarjoui E.Severe hypothermia in infants.Helv Paediatr Acta. 1982;37:317-22. Sofer S, Yagupsky P, Hershkowits J, Bearman JE.Improved outcome of hypothermic infants.Pediatr Emerg Care. 1986;2:211-4. Petrova A, Demissie K, Rhoads GG, et al. Association of maternal fever dang labor with neonatal and infant morbidity and mortality.Obstet Gynecol. 2001;98:20-7. Alexander JM, McIntire DM, Leveno KJ.Chorioamnionitis and the prognosis for term infants.Obstet Gynecol. 1999;94:274-8. Greenwell EA, Wyshak G, Ringer SA, et al. Intrapartum temperature elevation, epidural use, and adverse outcome in term infants.Pediatrics. 2012;129:447-54. Goetzl L, Manevich Y, Roedner C, et al. Maternal and fetal oxidative stress and intrapartum term fever.Am J Obstet Gynecol. 2010;202:363-1-5. Glass HC, Pham TN, Danielsen B, et al. Antenatal and intrapartum risk factors for seizures in term newborns:a population-based study, California 1998-2002.J Pediatr. 2009;154:24-28.e1. Lieberman E, Lang J, Richardson DK, et al. Intrapartum maternal fever and neonatal outcome.Pediatrics. 2000;105:1 Pt 18-13. Lieberman E, Eichenwald E, Mathur G, et al. Intrapartum fever and unexplained seizures in term infants.Pediatrics. 2000;106:983-8. Cordero L Jr, Hon EH.Neonatal bradycardia following nasopharyngeal stimulation.J Pediatr. 1971;78:441-7. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section:a prospective randomized controlled trial.Gynecol Obstet Invest. 2006;61:9-14. Waltman PA, Brewer JM, Rogers BP, May WL.Building evidence for practice:a pilot study of newborn bulb suctioning at birth.J Midwifery Womens Health. 2004;49:32-8. Kamlin CO, O’Donnell CP, Everest NJ, Davis PG, Morley CJ.Accuracy of clinical assessment of infant heart rate in the delivery room.Resuscitation. 2006;71:319-21. Dawson JA, Saraswat A, Simionato L, et al. Comparison of heart rate and oxygen saturation measurements from Masimo and Nellcor pulse oximeters in newly born term infants.Acta Paediatr. 2013;102:955-60. Katheria A, Rich W, Finer N.Electrocardiogram provides a continuous heart rate faster than oximetry dang neonatal resuscitation.Pediatrics. 2012;130:1177-81. Mizumoto H, Tomotaki S, Shibata H, et al. Electrocardiogram shows reliable heart rates much earlier than pulse oximetry dang neonatal resuscitation.Pediatr Int. 2012;54:205-7. van Vonderen JJ, Hooper SB, Kroese JK, et al. Pulse oximetry measures a lower heart rate at birth compared with electrocardiography.J Pediatr. 2015;166:49-53. Kamlin CO, Dawson JA, O’Donnell CP, et al. Accuracy of pulse oximetry measurement of heart rate of newborn infants in the delivery room.J Pediatr. 2008;152:756-60. Davis PG, Tan A, O’Donnell CP, Schulze A.Resuscitation of newborn infants with 100% oxygen or air:a systematic review and meta-analysis.Lancet. 2004;364:1329-33. Rabi Y, Rabi D, Yee W.Room air resuscitation of the depressed newborn:a systematic review and meta-analysis.Resuscitation. 2007;72:353-63. Morley CJ, Davis PG, Doyle LW, et al. COIN Trial InvestigatorsNasal CPAP or intubation at birth for very preterm infants.N Engl J Med. 2008;358:700-8. SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research NetworkFiner NN, Carlo WA, et al. Early CPAP versus surfactant in extremely preterm infants.N Engl J Med. 2010;362:1970-9. Dunn MS, Kaempf J, de Klerk A, et al. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates.Pediatrics. 2011;128:1069-76. Hishikawa K, Goishi K, Fujiwara T, et al. Pulmonary air leak associated with CPAP at term birth resuscitation.Arch Dis Child Fetal Neonatal Ed. 2015;100:F382-7. Poets CF, Rüdiger M.Mask CPAP dang neonatal transition:too much of a good thing for some term infants?.Arch Dis Child Fetal Neonatal Ed. 2015;100:F378-9. Harling AE, Beresford MW, Vince GS, Bates M, Yoxall CW.Does sustained lung inflation at resuscitation reduce lung injury in the preterm infant?.Arch Dis Child Fetal Neonatal Ed. 2005;90:F406-10. Lindner W, Högel J, Pohlandt F.Sustained pressure-controlled inflation or intermittent mandatory ventilation in preterm infants in the delivery room? A randomized, controlled trial on initial respiratory support via nasopharyngeal tube.Acta Paediatr. 2005;94:303-9. Lista G, Boni L, Scopesi F, et al. SLI Trial InvestigatorsSustained lung inflation at birth for preterm infants:a randomized clinical trial.Pediatrics. 2015;135:457-64. Lindner W, Vossbeck S, Hummler H, Pohlandt F.Delivery room management of extremely low birth weight infants:spontaneous breathing or intubation?.Pediatrics. 1999;103:5 pt 1961-7. Lista G, Fontana P, Castoldi F, Cavigioli F, Dani C.Does sustained lung inflation at birth improve outcome of preterm infants at risk for respiratory distress syndrome?.Neonatology. 2011;99:45-50. Vyas H, Milner AD, Hopkin IE, Boon AW.Physiologic responses to prolonged and slow-rise inflation in the resuscitation of the asphyxiated newborn infant.J Pediatr. 1981;99:635-9. Boon AW, Milner AD, Hopkin IE.Lung expansion, tidal exchange, and formation of the functional residual capacity dang resuscitation of asphyxiated neonates.J Pediatr. 1979;95:1031-6. Aziz HF, Martin JB, Moore JJ.The pediatric disposable end-tidal carbon dioxide detector role in endotracheal intubation in newborns.J Perinatol. 1999;19:110-3. Bhende MS, LaCovey D.A note of caution about the continuous use of colorimetric end-tidal CO2 detectors in children.Pediatrics. 1995;95:800-1. Repetto JE, Donohue PA-C PK, Baker SF, Kelly L, Nogee LM.Use of capnography in the delivery room for assessment of endotracheal tube placement.J Perinatol. 2001;21:284-7. Roberts WA, Maniscalco WM, Cohen AR, Litman RS, Chhibber A.The use of capnography for recognition of esophageal intubation in the neonatal intensive care unit.Pediatr Pulmonol. 1995;19:262-8. Gill I, O’Donnell CP.Vocal cord guides on neonatal endotracheal tubes.Arch Dis Child Fetal Neonatal Ed. 2014;99:F344. Singh R, Mohan CV, Taxak S.Controlled trial to evaluate the use of LMA for neonatal resuscitation.J Anaesth Clin Pharmacol. 2005;21:303-6. Zhu XY, Lin BC, Zhang QS, Ye HM, Yu RJ.A prospective evaluation of the efficacy of the laryngeal mask airway dang neonatal resuscitation.Resuscitation. 2011;82:1405-9. Feroze F, Khuwaja A, Masood N, Malik FI.Neonatal resuscitation:the use of laryngeal mask airway.Professional Med J. 2008;15:148-52. Esmail N, Saleh M, Ali A.Laryngeal mask airway versus endotracheal intubation for Apgar score improvement in neonatal resuscitation.Egypt J Anesthesiol. 2002;18:115-21. Christman C, Hemway RJ, Wyckoff MH, Perlman JM.The two-thumb is superior to the two-finger method for administering chest compressions in a manikin model of neonatal resuscitation.Arch Dis Child Fetal Neonatal Ed. 2011;96:F99-F101. Dorfsman ML, Menegazzi JJ, Wadas RJ, Auble TE.Two-thumb vs. two-finger chest compression in an infant model of prolonged cardiopulmonary resuscitation.Acad Emerg Med. 2000;7:1077-82. Hoa PK, Frank LR, Menegazzi JJ, Taylor R.A randomized, controlled trial of two-thumb vs two-finger chest compression in a swine infant model of cardiac arrest [see comment].Prehosp Emerg Care. 1997;1:65-7. Martin PS, Kemp AM, Theobald PS, Maguire SA, Jones MD.Do chest compressions dang simulated infant CPR comply with international recommendations?.Arch Dis Child. 2013;98:576-81. Martin PS, Kemp AM, Theobald PS, Maguire SA, Jones MD.Does a more “physiological”infant manikin design effect chest compression quality and create a potential for thoracic over-compression dang simulated infant CPR?.Resuscitation. 2013;84:666-71. Martin P, Theobald P, Kemp A, et al. Real-time feedback can improve infant manikin cardiopulmonary resuscitation by up to 79%--a randomised controlled trial.Resuscitation. 2013;84:1125-30. Menegazzi JJ, Auble TE, Nicklas KA, et al. Two-thumb versus two-finger chest compression dang CPR in a swine infant model of cardiac arrest.Ann Emerg Med. 1993;22:240-3. Udassi S, Udassi JP, Lamb MA, et al. Two-thumb technique is superior to two-finger technique dang lone rescuer infant manikin CPR.Resuscitation. 2010;81:712-7. Whitelaw CC, Slywka B, Goldsmith LJ.Comparison of a two-finger versus two-thumb method for chest compressions by healthcare providers in an infant mechanical model.Resuscitation. 2000;43:213-6. Dannevig I, Solevåg AL, Saugstad OD, Nakstad B.Lung injury in asphyxiated newborn pigs resuscitated from cardiac arrest - the impact of supplementary oxygen, longer ventilation intervals and chest compressions at different compression-to-ventilation ratios.Open Respir Med J. 2012;6:89-96. Dannevig I, Solevåg AL, Sonerud T, Saugstad OD, Nakstad B.Brain inflammation induced by severe asphyxia in newborn pigs and the impact of alternative resuscitation strategies on the newborn central nervous system.Pediatr Res. 2013;73:163-70. Solevåg AL, Dannevig I, Wyckoff M, Saugstad OD, Nakstad B.Extended series of cardiac compressions dang CPR in a swine model of perinatal asphyxia.Resuscitation. 2010;81:1571-6. Solevåg AL, Dannevig I, Wyckoff M, Saugstad OD, Nakstad B.Return of spontaneous circulation with a compression:ventilation ratio of 15:2 versus 3:1 in newborn pigs with cardiac arrest due to asphyxia.ArchDis Child Fetal Neonatal Ed. 2011;96:F417-21. Solevåg AL, Madland JM, Gjærum E, Nakstad B.Minute ventilation at different compression to ventilation ratios, different ventilation rates, and continuous chest compressions with asynchronous ventilation in a newborn manikin.Scand J Trauma Resusc Emerg Med. 2012;20:73. Hemway RJ, Christman C, Perlman J.The 3:1 is superior to a 15:2 ratio in a newborn manikin model in terms of quality of chest compressions and number of ventilations.Arch Dis Child Fetal Neonatal Ed. 2013;98:F42-5. Linner R, Werner O, Perez-de-Sa V, Cunha-Goncalves D.Circulatory recovery is as fast with air ventilation as with 100% oxygen after asphyxia-induced cardiac arrest in piglets.Pediatr Res. 2009;66:391-4. Lipinski CA, Hicks SD, Callaway CW.Normoxic ventilation dang resuscitation and outcome from asphyxial cardiac arrest in rats.Resuscitation. 1999;42:221-9. Perez-de-Sa V, Cunha-Goncalves D, Nordh A, et al. High brain tissue oxygen tension dang ventilation with 100% oxygen after fetal asphyxia in newborn sheep.Pediatr Res. 2009;65:57-61. Solevåg AL, Dannevig I, Nakstad B, Saugstad OD.Resuscitation of severely asphyctic newborn pigs with cardiac arrest by using 21% or 100% oxygen.Neonatology. 2010;98:64-72. Temesvári P, Karg E, Bódi I, et al. Impaired early neurologic outcome in newborn piglets reoxygenated with 100% oxygen compared with room air after pneumothorax-induced asphyxia.Pediatr Res. 2001;49:812-9. Walson KH, Tang M, Glumac A, et al. Normoxic versus hyperoxic resuscitation in pediatric asphyxial cardiac arrest:effects on oxidative stress.Crit Care Med. 2011;39:335-43. Yeh ST, Cawley RJ, Aune SE, Angelos MG.Oxygen requirement dang cardiopulmonary resuscitation (CPR) to effect return of spontaneous circulation.Resuscitation. 2009;80:951-5. Richmond S, Wyllie J.European Resuscitation Council Guidelines for Resuscitation 2010 Section 7. Resuscitation of babies at birth.Resuscitation. 2010;81:1389-99. Crespo SG, Schoffstall JM, Fuhs LR, Spivey WH.Comparison of two doses of endotracheal epinephrine in a cardiac arrest model.Ann Emerg Med. 1991;20:230-4. Jasani MS, Nadkarni VM, Finkelstein MS, et al. Effects of different techniques of endotracheal epinephrine administration in pediatric porcine hypoxic-hypercarbic cardiopulmonary arrest.Crit Care Med. 1994;22:1174-80. Mielke LL, Frank C, Lanzinger MJ, et al. Plasma catecholamine levels following tracheal and intravenous epinephrine administration in swine.Resuscitation. 1998;36:187-92. Roberts JR, Greenberg MI, Knaub MA, Kendrick ZV, Baskin SI.Blood levels following intravenous and endotracheal epinephrine administration.JACEP. 1979;8:53-6. Hörnchen U, Schüttler J, Stoeckel H, Eichelkraut W, Hahn N.Endobronchial instillation of epinephrine dang cardiopulmonary resuscitation.Crit Care Med. 1987;15:1037-9. Wyckoff MH, Perlman JM, Laptook AR.Use of volume expansion dang delivery room resuscitation in near-term and term infants.Pediatrics. 2005;115:950-5. Segal S, Anyan WR, Hill RM, Kauffman RE, Mofenson H, Pruitt AW, Shinefield HR, Singer HS, Weinberger MM.Naloxone use in newborns.Pediatrics. 1980;65:667. Moe-Byrne T1, Brown JV, McGuire W.Naloxone for opiate-exposed newborn infants.Cochrane Database Syst Rev. 2013;Feb28:2CD003483-doi:10.1002/14651858.CD003483.pub2. Brambrink AM, Ichord RN, Martin LJ, Koehler RC, Traystman RJ.Poor outcome after hypoxia-ischemia in newborns is associated with physiological abnormalities dang early recovery. Possible relevance to secondary brain injury after head trauma in infants.Exp Toxicol Pathol. 1999;51:151-62. Salhab WA, Wyckoff MH, Laptook AR, Perlman JM.Initial hypoglycemia and neonatal brain injury in term infants with severe fetal acidemia.Pediatrics. 2004;114:361-6. Lee SK, Penner PL, Cox M.Comparison of the attitudes of health care professionals and parents toward active treatment of very low birth weight infants.Pediatrics. 1991;88:110-4. Harrington DJ, Redman CW, Moulden M, Greenwood CE.The long-term outcome in surviving infants with Apgar zero at 10 minutes:a systematic review of the literature and hospital-based cohort.Am J Obstet Gynecol. 2007;196:463.e1-5. Patel H, Beeby PJ.Resuscitation beyond 10 minutes of term babies born without signs of life.J Paediatr Child Health. 2004;40:136-8. Casalaz DM, Marlow N, Speidel BD.Outcome of resuscitation following unexpected apparent stillbirth.Arch Dis Child Fetal Neonatal Ed. 1998;78:F112-5. Savoldelli GL, Naik VN, Park J, et al. Value of debriefing dang simulated crisis management:oral versus video-assisted oral feedback.Anesthesiology. 2006;105:279-85. Edelson DP, Litzinger B, Arora V, et al. Improving in-hospital cardiac arrest process and outcomes with performance debriefing.Arch Intern Med. 2008;168:1063-9. DeVita MA, Schaefer J, Lutz J, Wang H, Dongilli T.Improving medical emergency team (MET) performance using a novel curriculum and a computerized human patient simulator.Qual Saf Health Care. 2005;14:326-31. Wayne DB, Butter J, Siddall VJ, et al. Simulation-based training of internal medicine residents in advanced cardiac life support protocols:a randomized trial.Teach Learn Med. 2005;17:210-6. Clay AS, Que L, Petrusa ER, Sebastian M, Govert J.Debriefing in the intensive care unit:a feedback tool to facilitate bedside teaching.Crit Care Med. 2007;35:738-54. Blum RH, Raemer DB, Carroll JS, Dufresne RL, Cooper JB.A method for measang the effectiveness of simulation-based team training for improving communication skills.Anesth Analg. 2005;100:1375-80. Schmid MB, Reister F, Mayer B, et al. Prospective risk factor monitoring reduces intracranial hemorrhage rates in preterm infants.Dtsch Arztebl Int. 2013;110:489-96. Berden HJ, Willems FF, Hendrick JM, Pijls NH, Knape JT.How frequently should basic cardiopulmonary resuscitation training be repeated to maintain adequate skills?.BMJ. 1993;306:1576-7. Ernst KD, Cline WL, Dannaway DC, et al. Weekly and consecutive day neonatal intubation training:comparable on a pediatrics clerkship.Acad Med. 2014;89:505-10. Kaczorowski J, Levitt C, Hammond M, et al. Retention of neonatal resuscitation skills and knowledge:a randomized controlled trial.Fam Med. 1998;30:705-11. Kovacs G, Bullock G, Ackroyd-Stolarz S, Cain E, Petrie D.A randomized controlled trial on the effect of educational interventions in promoting airway management skill maintenance.Ann Emerg Med. 2000;36:301-9. Montgomery C, Kardong-Edgren SE, Oermann MH, Odom-Maryon T.Student satisfaction and self report of CPR competency:HeartCode BLS courses, instructor-led CPR courses, and monthly voice advisory manikin practice for CPR skill maintenance.Int J Nurs Educ Scholarsh. 2012;9:. Oermann MH, Kardong-Edgren SE, Odom-Maryon T.Effects of monthly practice on nursing students’CPR psychomotor skill performance.Resuscitation. 2011;82:447-53. Stross JK.Maintaining competency in advanced cardiac life support skills.JAMA. 1983;249:3339-41. Su E, Schmidt TA, Mann NC, Zechnich AD.A randomized controlled trial to assess decay in acquired knowledge among paramedics completing a pediatric resuscitation course.Acad Emerg Med. 2000;7:779-86. Sutton RM, Niles D, Meaney PA, et al. “Booster“training:evaluation of instructor-led bedside cardiopulmonary resuscitation skill training and automated corrective feedback to improve cardiopulmonary resuscitation compliance of Pediatric Basic Life Support providers dang simulated cardiac arrest.Pediatr Crit Care Med. 2011;12:116-21. Turner NM, Scheffer R, Custers E, Cate OT.Use of unannounced spaced telephone testing to improve retention of knowledge after life-support courses.Med Teach. 2011;33:731-7. Lubin J, Carter R.The feasibility of daily mannequin practice to improve intubation success.Air Med J. 2009;28:195-7. Mosley CM, Shaw BN.A longitudinal cohort study to investigate the retention of knowledge and skills following attendance on the Newborn Life support course.Arch Dis Child. 2013;98:582-6. Nadel FM, Lavelle JM, Fein JA, et al. Teaching resuscitation to pediatric residents:the effects of an intervention.Arch Pediatr Adolesc Med. 2000;154:1049-54. Niles D, Sutton RM, Donoghue A, et al. “Rolling Refreshers”:a novel approach to maintain CPR psychomotor skill competence.Resuscitation. 2009;80:909-12. Nishisaki A, Donoghue AJ, Colborn S, et al. Effect of just-in-time simulation training on tracheal intubation procedure safety in the pediatric intensive care unit.Anesthesiology. 2010;113:214-23. O’Donnell CM, Skinner AC.An evaluation of a short course in resuscitation training in a district general hospital.Resuscitation. 1993;26:193-201. Breckwoldt J, Svensson J, Lingemann C, Gruber H.Does clinical teacher training always improve teaching effectiveness as opposed to no teacher training? A randomized controlled study.BMC Med Educ. 2014;14:6. Boerboom TB, Jaarsma D, Dolmans DH, et al. Peer group reflection helps clinical teachers to critically reflect on their teaching.Med Teach. 2011;33:615-23. Litzelman DK, Stratos GA, Marriott DJ, Lazaridis EN, Skeff KM.Beneficial and harmful effects of augmented feedback on physicians’ clinical-teaching performances.Acad Med. 1998;73:324-32. Naji SA, Maguire GP, Fairbairn SA, Goldberg DP, Faragher EB.Training clinical teachers in psychiatry to teach interviewing skills to medical students.Med Educ. 1986;20:140-7. Schum TR, Yindra KJ.Relationship between systematic feedback to faculty and ratings of clinical teaching.Acad Med. 1996;71:1100-2. Skeff KM, Stratos G, Campbell M, Cooke M, Jones HW, 3rdlastEvaluation of the seminar method to improve clinical teaching.J Gen Intern Med. 1986;1:315-22. Lye P, Heidenreich C, Wang-Cheng R, Bragg D, Simpson D.Advanced Faculty Development GroupExperienced clinical educators improve their clinical teaching effectiveness.Ambul Pediatr. 2003;3:93-7. Regan-Smith M, Hirschmann K, Iobst W.Direct observation of faculty with feedback:an effective means of improving patient-centered and learner-centered teaching skills.Teach Learn Med. 2007;19:278-86.
REFERENCES
1. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Part 7: Neonatal Resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2015; 132(16 Suppl 1):S204-41. https://doi.org/10.1161/CIR.0000000000000276
PMid:26472855
2. Wyckoff MH, Aziz K, Escobedo MB, et al. Part 13: Neonatal Resuscitation: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015; 132(18 Suppl 2):S543-60. https://doi.org/10.1161/CIR.0000000000000267
PMid:26473001
3. Wyllie J, Perlman JM, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Part 7: Neonatal resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2015; 95:e169-201. https://doi.org/10.1016/j.resuscitation.2015.07.045
PMid:26477424
4. Perlman JM, Wyllie J, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2010; 122(16 Suppl 2):S516-38. https://doi.org/10.1161/CIRCULATIONAHA.110.971127
PMid:20956259
5. Wyllie J, Perlman JM, Kattwinkel J, et al; Neonatal Resuscitation Chapter Collaborators. Part 11: Neonatal resuscitation: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2010; 81 Suppl 1:e260-87. https://doi.org/10.1016/j.resuscitation.2010.08.029
PMid:20956039
6. Singapore National Resuscitation Council's Neonatal and Paediatric Resuscitation Workgroup, Chong NK. Newborn and paediatric resuscitation 2011 guidelines. Singapore Med J 2011; 52:560-72.
PMid:21879213
7. Ersdal HL, Mduma E, Svensen E, Perlman JM. Early initiation of basic resuscitation interventions including face mask ventilation may reduce birth asphyxia related mortality in low-income countries: a prospective descriptive observational study. Resuscitation 2012; 83:869-73. https://doi.org/10.1016/j.resuscitation.2011.12.011
PMid:22198423
9. Barber CA, Wyckoff MH. Use and efficacy of endotracheal versus intravenous epinephrine during neonatal cardiopulmonary resuscitation in the delivery room. Pediatrics 2006; 118:1028-34. https://doi.org/10.1542/peds.2006-0416
PMid:16950994
10. Wong CY, Yeo CL. Resuscitation of the newborn in Singapore General Hospital: how often is it required, what factors predict the need for resuscitation at birth, and what are the outcomes? Poster abstract at PSANZ, 2010.
11. McDonald SJ, Middleton P, Dowswell T, Morris PS. Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Cochrane Database Syst Rev 2013; CD004074. https://doi.org/10.1002/14651858.CD004074.pub3
12. Hosono S, Mugishima H, Fujita H, et al. Umbilical cord milking reduces the need for red cell transfusions and improves neonatal adaptation in infants born at less than 29 weeks' gestation: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed 2008; 93:F14-9. https://doi.org/10.1136/adc.2006.108902
PMid:17234653
13. Katheria AC, Leone TA, Woelkers D, et al. The effects of umbilical cord milking on hemodynamics and neonatal outcomes in premature neonates. J Pediatr 2014; 164:1045-1050.e1. https://doi.org/10.1016/j.jpeds.2014.01.024
PMid:24560179
14. March MI, Hacker MR, Parson AW, Modest AM, de Veciana M. The effects of umbilical cord milking in extremely preterm infants: a randomized controlled trial. J Perinatol 2013; 33:763-7. https://doi.org/10.1038/jp.2013.70
PMid:23867960 PMCid:PMC3916936
15. Budin P. The Nursling: the Feeding and Hygiene of Premature and Full-term Infants. London: Caxton Publishing Co, 1907.
16. A Abd-El Hamid S, Badr-El Din MM, Dabous NI, Saad KM. Effect of the use of a polyethylene wrap on the morbidity and mortality of very low birth weight infants in Alexandria University Children's Hospital. J Egypt Public Health Assoc 2012; 87:104-8. https://doi.org/10.1097/01.EPX.0000421565.24496.d9
PMid:23196883
17. Acolet D, Elbourne D, McIntosh N, et al; Confi dential Enquiry Into Maternal and Child Health. Project 27/28: inquiry into quality of neonatal care and its effect on the survival of infants who were born at 27 and 28 weeks in England, Wales, and Northern Ireland. Pediatrics 2005; 116:1457-65. https://doi.org/10.1542/peds.2004-2691
PMid:16322171
18. Bateman DA, O'Bryan L, Nicholas SW, Heagarty MC. Outcome of unattended out-of-hospital births in Harlem. Arch Pediatr Adolesc Med 1994; 148:147-52. https://doi.org/10.1001/archpedi.1994.02170020033005
PMid:8118531
20. Boo NY, Guat-Sim Cheah I; Malaysian National Neonatal Registry. Admission hypothermia among VLBW infants in Malaysian NICUs. J Trop Pediatr 2013; 59:447-52. https://doi.org/10.1093/tropej/fmt051
PMid:23774951
21. Buetow KC, Klein SW. Effects of maintenance of "normal" skin temperature on survival of infants of low birth weight. Pediatrics 1964; 34:163-70.
PMid:14211076
22. Costeloe K, Hennessy E, Gibson AT, Marlow N, Wilkinson AR. The EPICure study: outcomes to discharge from hospital for infants born at the threshold of viability. Pediatrics 2000; 106:659-71. https://doi.org/10.1542/peds.106.4.659
PMid:11015506
23. Costeloe KL, Hennessy EM, Haider S, et al. Short term outcomes after extreme preterm birth in England: comparison of two birth cohorts in 1995 and 2006 (the EPICure studies). BMJ 2012; 345:e7976. https://doi.org/10.1136/bmj.e7976
PMid:23212881 PMCid:PMC3514472
24. da Mota Silveira SM, Gonçalves de Mello MJ, de Arruda Vidal S, de Frias PG, Cattaneo A. Hypothermia on admission: a risk factor for death in newborns referred to the Pernambuco Institute of Mother and Child Health. J Trop Pediatr 2003; 49:115-20. https://doi.org/10.1093/tropej/49.2.115
PMid:12729295
25. Daga AS, Daga SR, Patole SK. Determinants of death among admissions to intensive care unit for newborns. J Trop Pediatr 1991; 37:53-6. https://doi.org/10.1093/tropej/37.2.53
PMid:2027164
26. de Almeida MF, Guinsburg R, Sancho GA, et al; Brazilian Network on Neonatal Research. Hypothermia and early neonatal mortality in preterm infants. J Pediatr 2014; 164:271-5.e1. https://doi.org/10.1016/j.jpeds.2013.09.049
PMid:24210925
27. García-Mu-oz Rodrigo F, Rivero Rodríguez S, Siles Quesada C. [Hypothermia risk factors in the very low weight newborn and associated morbidity and mortality in a neonatal care unit]. An Pediatr (Barc) 2014; 80:144-50. Spanish.
28. Harms K, Osmers R, Kron M, et al. [Mortality of premature infants 1980-1990: analysis of data from the Göttingen perinatal center]. Z Geburtshilfe Perinatol 1994; 198:126-33. German.
PMid:7975798
29. Hazan J, Maag U, Chessex P. Association between hypothermia and mortality rate of premature infants--revisited. Am J Obstet Gynecol 1991; 164(1 Pt 1):111-2. https://doi.org/10.1016/0002-9378(91)90638-8
31. Kalimba EM, Ballot DE. Survival of extremely low-birth-weight infants. S Afr J Child Health 2013; 7:13-6. https://doi.org/10.7196/sajch.488
32. Kambarami R, Chidede O. Neonatal hypothermia levels and risk factors for mortality in a tropical country. Cent Afr J Med 2003; 49:103-6.
PMid:15298464
33. Kent AL, Williams J. Increasing ambient operating theatre temperature and wrapping in polyethylene improves admission temperature in premature infants. J Paediatr Child Health 2008; 44:325-31. https://doi.org/10.1111/j.1440-1754.2007.01264.x
PMid:18194198
34. Laptook AR, Salhab W, Bhaskar B; Neonatal Research Network. Admission temperature of low birth weight infants: predictors and associated morbidities. Pediatrics 2007; 119:e643-9. https://doi.org/10.1542/peds.2006-0943
PMid:17296783
35. Lee HC, Ho QT, Rhine WD. A quality improvement project to improve admission temperatures in very low birth weight infants. J Perinatol 2008; 28:754-8. https://doi.org/10.1038/jp.2008.92
PMid:18580878
36. Levi S, Taylor W, Robinson LE, Levy LI. Analysis of morbidity and outcome of infants weighing less than 800 grams at birth. South Med J 1984; 77:975-8. https://doi.org/10.1097/00007611-198408000-00010
PMid:6463697
37. Manani M, Jegatheesan P, DeSandre G, et al. Elimination of admission hypothermia in preterm very low-birth-weight infants by standardization of delivery room management. Perm J 2013; 17:8-13. https://doi.org/10.7812/TPP/12-130
PMid:24355884 PMCid:PMC3783084
38. Manji KP, Kisenge R. Neonatal hypothermia on admission to a special care unit in Dar-es-Salaam, Tanzania: a cause for concern. Cent Afr J Med 2003; 49:23-7.
PMid:14562586
39. Mathur NB, Krishnamurthy S, Mishra TK. Evaluation of WHO classification of hypothermia in sick extramural neonates as predictor of fatality. J Trop Pediatr 2005; 51:341-5. https://doi.org/10.1093/tropej/fmi049
PMid:16014762
40. Miller SS, Lee HC, Gould JB. Hypothermia in very low birth weight infants: distribution, risk factors and outcomes. J Perinatol 2011; 31 Suppl 1:S49-56. https://doi.org/10.1038/jp.2010.177
PMid:21448204
41. Mullany LC, Katz J, Khatry SK, et al. Risk of mortality associated with neonatal hypothermia in southern Nepal. Arch Pediatr Adolesc Med 2010; 164:650-6. https://doi.org/10.1001/archpediatrics.2010.103
PMid:20603466
42. Nayeri F, Nili F. Hypothermia at birth and its associated complications in newborns: a follow-up study. Iran J Public Health. 2006; 35:48-52.
43. Obladen M, Heemann U, Hennecke KH, Hanssler L. [Causes of neonatal mortality 1981-1983: a regional analysis]. Z Geburtshilfe Perinatol 1985; 189:181-7. German.
PMid:3876659
45. Pal DK, Manandhar DS, Rajbhandari S, et al. Neonatal hypoglycaemia in Nepal 1. Prevalence and risk factors. Arch Dis Child Fetal Neonatal Ed 2000; 82:F46-51. https://doi.org/10.1136/fn.82.1.F46
PMid:10634842 PMCid:PMC1721035
46. Shah S, Zemichael O, Meng HD. Factors associated with mortality and length of stay in hospitalised neonates in Eritrea, Africa: a cross-sectional study. BMJ Open 2012; 2. pii: e000792. https://doi.org/10.1136/bmjopen-2011-000792
47. Singh A, Yadav A, Singh A. Utilization of postnatal care for newborns and its association with neonatal mortality in India: an analytical appraisal. BMC Pregnancy Childbirth 2012; 12:33. https://doi.org/10.1186/1471-2393-12-33
PMid:22571689 PMCid:PMC3405468
48. Sodemann M, Nielsen J, Veirum J, et al. Hypothermia of newborns is associated with excess mortality in the first 2 months of life in Guinea-Bissau, West Africa. Trop Med Int Health 2008; 13:980-6. https://doi.org/10.1111/j.1365-3156.2008.02113.x
PMid:18631315
49. Stanley FJ, Alberman EV. Infants of very low birthweight. I: Perinatal factors affecting survival. Dev Med Child Neurol 1978; 20:300-12. https://doi.org/10.1111/j.1469-8749.1978.tb15220.x
PMid:669063
50. Motil KJ, Blackburn MG, Pleasure JR. The effects of four different radiant warmer temperature set-points used for rewarming neonates. J Pediatr 1974; 85:546-50. https://doi.org/10.1016/S0022-3476(74)80467-1
54. Petrova A, Demissie K, Rhoads GG, et al. Association of maternal fever during labor with neonatal and infant morbidity and mortality. Obstet Gynecol 2001; 98:20-7. https://doi.org/10.1097/00006250-200107000-00005
PMid:11430951
56. Greenwell EA, Wyshak G, Ringer SA, et al. Intrapartum temperature elevation, epidural use, and adverse outcome in term infants. Pediatrics 2012; 129:e447-54. https://doi.org/10.1542/peds.2010-2301
PMid:22291120 PMCid:PMC3357045
57. Goetzl L, Manevich Y, Roedner C, et al. Maternal and fetal oxidative stress and intrapartum term fever. Am J Obstet Gynecol 2010; 202:363.e1-5. https://doi.org/10.1016/j.ajog.2010.01.034
PMid:20350644 PMCid:PMC4594801
58. Glass HC, Pham TN, Danielsen B, et al. Antenatal and intrapartum risk factors for seizures in term newborns: a population-based study, California 1998-2002. J Pediatr 2009; 154:24-28.e1. https://doi.org/10.1016/j.jpeds.2008.07.008
PMid:18760807 PMCid:PMC2635430
59. Lieberman E, Lang J, Richardson DK, et al. Intrapartum maternal fever and neonatal outcome. Pediatrics 2000; 105(1 Pt 1):8-13. https://doi.org/10.1542/peds.105.1.8
PMid:10617697
60. Lieberman E, Eichenwald E, Mathur G, et al. Intrapartum fever and unexplained seizures in term infants. Pediatrics 2000; 106:983-8. https://doi.org/10.1542/peds.106.5.983
PMid:11061764
62. Gungor S, Kurt E, Teksoz E, et al. Oronasopharyngeal suction versus no suction in normal and term infants delivered by elective cesarean section: a prospective randomized controlled trial. Gynecol Obstet Invest 2006; 61:9-14. https://doi.org/10.1159/000087604
PMid:16113579
63. Waltman PA, Brewer JM, Rogers BP, May WL. Building evidence for practice: a pilot study of newborn bulb suctioning at birth. J Midwifery Womens Health 2004; 49:32-8.
PMid:14710138
64. Kamlin CO, O'Donnell CP, Everest NJ, Davis PG, Morley CJ. Accuracy of clinical assessment of infant heart rate in the delivery room. Resuscitation 2006; 71:319-21. https://doi.org/10.1016/j.resuscitation.2006.04.015
PMid:16989935
65. Dawson JA, Saraswat A, Simionato L, et al. Comparison of heart rate and oxygen saturation measurements from Masimo and Nellcor pulse oximeters in newly born term infants. Acta Paediatr 2013; 102:955-60. https://doi.org/10.1111/apa.12329
PMid:23800004
66. Katheria A, Rich W, Finer N. Electrocardiogram provides a continuous heart rate faster than oximetry during neonatal resuscitation. Pediatrics 2012; 130:e1177-81. https://doi.org/10.1542/peds.2012-0784
PMid:23090347
67. Mizumoto H, Tomotaki S, Shibata H, et al. Electrocardiogram shows reliable heart rates much earlier than pulse oximetry during neonatal resuscitation. Pediatr Int 2012; 54:205-7. https://doi.org/10.1111/j.1442-200X.2011.03506.x
PMid:22044505
68. van Vonderen JJ, Hooper SB, Kroese JK, et al. Pulse oximetry measures a lower heart rate at birth compared with electrocardiography. J Pediatr 2015; 166:49-53. https://doi.org/10.1016/j.jpeds.2014.09.015
PMid:25444526
69. Kamlin CO, Dawson JA, O'Donnell CP, et al. Accuracy of pulse oximetry measurement of heart rate of newborn infants in the delivery room. J Pediatr 2008; 152:756-60. https://doi.org/10.1016/j.jpeds.2008.01.002
PMid:18492509
70. Davis PG, Tan A, O'Donnell CP, Schulze A. Resuscitation of newborn infants with 100% oxygen or air: a systematic review and meta-analysis. Lancet 2004; 364:1329-33. https://doi.org/10.1016/S0140-6736(04)17189-4
71. Rabi Y, Rabi D, Yee W. Room air resuscitation of the depressed newborn: a systematic review and meta-analysis. Resuscitation 2007; 72:353-63. https://doi.org/10.1016/j.resuscitation.2006.06.134
PMid:17240032
72. Morley CJ, Davis PG, Doyle LW, et al; COIN Trial Investigators. Nasal CPAP or intubation at birth for very preterm infants. N Engl J Med 2008; 358:700-8. https://doi.org/10.1056/NEJMoa072788
PMid:18272893
73. SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network, Finer NN, Carlo WA, et al. Early CPAP versus surfactant in extremely preterm infants. N Engl J Med 2010; 362:1970-9. https://doi.org/10.1056/NEJMoa0911783
PMid:20472939 PMCid:PMC3071534
74. Dunn MS, Kaempf J, de Klerk A, et al. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics 2011; 128:e1069-76. https://doi.org/10.1542/peds.2010-3848
PMid:22025591
75. Hishikawa K, Goishi K, Fujiwara T, et al. Pulmonary air leak associated with CPAP at term birth resuscitation. Arch Dis Child Fetal Neonatal Ed 2015; 100:F382-7. https://doi.org/10.1136/archdischild-2014-307891
PMid:25854822
76. Poets CF, Rüdiger M. Mask CPAP during neonatal transition: too much of a good thing for some term infants? Arch Dis Child Fetal Neonatal Ed 2015; 100:F378-9. https://doi.org/10.1136/archdischild-2015-308236
PMid:25877285
77. Harling AE, Beresford MW, Vince GS, Bates M, Yoxall CW. Does sustained lung inflation at resuscitation reduce lung injury in the preterm infant? Arch Dis Child Fetal Neonatal Ed 2005; 90:F406-10. https://doi.org/10.1136/adc.2004.059303
PMid:15863490 PMCid:PMC1721927
78. Lindner W, Högel J, Pohlandt F. Sustained pressure-controlled inflation or intermittent mandatory ventilation in preterm infants in the delivery room? A randomized, controlled trial on initial respiratory support via nasopharyngeal tube. Acta Paediatr 2005; 94:303-9.
PMid:16028648
79. Lista G, Boni L, Scopesi F, et al; SLI Trial Investigators. Sustained lung inflation at birth for preterm infants: a randomized clinical trial. Pediatrics 2015; 135:e457- 64. https://doi.org/10.1542/peds.2014-1692
PMid:25624390
80. Lindner W, Vossbeck S, Hummler H, Pohlandt F. Delivery room management of extremely low birth weight infants: spontaneous breathing or intubation? Pediatrics 1999; 103(5 pt 1):961-7. https://doi.org/10.1542/peds.103.5.961
PMid:10224173
81. Lista G, Fontana P, Castoldi F, Cavigioli F, Dani C. Does sustained lung inflation at birth improve outcome of preterm infants at risk for respiratory distress syndrome? Neonatology 2011; 99:45-50. https://doi.org/10.1159/000298312
PMid:20616570
82. Vyas H, Milner AD, Hopkin IE, Boon AW. Physiologic responses to prolonged and slow-rise inflation in the resuscitation of the asphyxiated newborn infant. J Pediatr 1981; 99:635-9. https://doi.org/10.1016/S0022-3476(81)80279-X
83. Boon AW, Milner AD, Hopkin IE. Lung expansion, tidal exchange, and formation of the functional residual capacity during resuscitation of asphyxiated neonates. J Pediatr 1979; 95:1031-6. https://doi.org/10.1016/S0022-3476(79)80304-2
84. Aziz HF, Martin JB, Moore JJ. The pediatric disposable end-tidal carbon dioxide detector role in endotracheal intubation in newborns. J Perinatol 1999; 19:110-3. https://doi.org/10.1038/sj.jp.7200136
PMid:10642970
85. Bhende MS, LaCovey D. A note of caution about the continuous use of colorimetric end-tidal CO2 detectors in children. Pediatrics 1995; 95:800-1.
PMid:7724335
86. Repetto JE, Donohue PA-C PK, Baker SF, Kelly L, Nogee LM. Use of capnography in the delivery room for assessment of endotracheal tube placement. J Perinatol 2001; 21:284-7. https://doi.org/10.1038/sj.jp.7210534
PMid:11536020
87. Roberts WA, Maniscalco WM, Cohen AR, Litman RS, Chhibber A. The use of capnography for recognition of esophageal intubation in the neonatal intensive care unit. Pediatr Pulmonol 1995; 19:262-8. https://doi.org/10.1002/ppul.1950190504
PMid:7567200
89. Singh R, Mohan CV, Taxak S. Controlled trial to evaluate the use of LMA for neonatal resuscitation. J Anaesth Clin Pharmacol 2005; 21:303-6.
90. Zhu XY, Lin BC, Zhang QS, Ye HM, Yu RJ. A prospective evaluation of the efficacy of the laryngeal mask airway during neonatal resuscitation. Resuscitation 2011; 82:1405-9. https://doi.org/10.1016/j.resuscitation.2011.06.010
PMid:21763393
91. Feroze F, Khuwaja A, Masood N, Malik FI. Neonatal resuscitation: the use of laryngeal mask airway. Professional Med J 2008; 15:148-52.
92. Esmail N, Saleh M, Ali A. Laryngeal mask airway versus endotracheal intubation for Apgar score improvement in neonatal resuscitation. Egypt J Anesthesiol 2002; 18:115-21.
93. Christman C, Hemway RJ, Wyckoff MH, Perlman JM. The two-thumb is superior to the two-finger method for administering chest compressions in a manikin model of neonatal resuscitation. Arch Dis Child Fetal Neonatal Ed 2011; 96:F99-F101. https://doi.org/10.1136/adc.2009.180406
PMid:20847197
94. Dorfsman ML, Menegazzi JJ, Wadas RJ, Auble TE. Two-thumb vs. two-finger chest compression in an infant model of prolonged cardiopulmonary resuscitation. Acad Emerg Med 2000; 7:1077-82. https://doi.org/10.1111/j.1553-2712.2000.tb01255.x
PMid:11015237
95. Houri PK, Frank LR, Menegazzi JJ, Taylor R. A randomized, controlled trial of two-thumb vs two-finger chest compression in a swine infant model of cardiac arrest [see comment]. Prehosp Emerg Care 1997; 1:65-7. https://doi.org/10.1080/10903129708958789
PMid:9709339
96. Martin PS, Kemp AM, Theobald PS, Maguire SA, Jones MD. Do chest compressions during simulated infant CPR comply with international recommendations? Arch Dis Child 2013; 98:576-81. https://doi.org/10.1136/archdischild-2012-302583
PMid:23193200
97. Martin PS, Kemp AM, Theobald PS, Maguire SA, Jones MD. Does a more "physiological" infant manikin design effect chest compression quality and create a potential for thoracic over-compression during simulated infant CPR? Resuscitation 2013; 84:666-71. https://doi.org/10.1016/j.resuscitation.2012.10.005
PMid:23123431
98. Martin P, Theobald P, Kemp A, et al. Real-time feedback can improve infant manikin cardiopulmonary resuscitation by up to 79%--a randomised controlled trial. Resuscitation 2013; 84:1125-30. https://doi.org/10.1016/j.resuscitation.2013.03.029
PMid:23571117
99. Menegazzi JJ, Auble TE, Nicklas KA, et al. Two-thumb versus two-finger chest compression during CPR in a swine infant model of cardiac arrest. Ann Emerg Med 1993; 22:240-3. https://doi.org/10.1016/S0196-0644(05)80212-4
100. Udassi S, Udassi JP, Lamb MA, et al. Two-thumb technique is superior to two-finger technique during lone rescuer infant manikin CPR. Resuscitation 2010; 81:712-7. https://doi.org/10.1016/j.resuscitation.2009.12.029
PMid:20227156
101. Whitelaw CC, Slywka B, Goldsmith LJ. Comparison of a two-finger versus two-thumb method for chest compressions by healthcare providers in an infant mechanical model. Resuscitation 2000; 43:213-6. https://doi.org/10.1016/S0300-9572(99)00145-8
102. Dannevig I, Solevåg AL, Saugstad OD, Nakstad B. Lung injury in asphyxiated newborn pigs resuscitated from cardiac arrest - the impact of supplementary oxygen, longer ventilation intervals and chest compressions at different compression-to-ventilation ratios. Open Respir Med J 2012; 6:89-96. https://doi.org/10.2174/1874306401206010089
PMid:23115599 PMCid:PMC3480705
103. Dannevig I, Solevåg AL, Sonerud T, Saugstad OD, Nakstad B. Brain inflammation induced by severe asphyxia in newborn pigs and the impact of alternative resuscitation strategies on the newborn central nervous system. Pediatr Res 2013; 73:163-70. https://doi.org/10.1038/pr.2012.167
PMid:23168577
104. Solevåg AL, Dannevig I, Wyckoff M, Saugstad OD, Nakstad B. Extended series of cardiac compressions during CPR in a swine model of perinatal asphyxia. Resuscitation 2010; 81:1571-6. https://doi.org/10.1016/j.resuscitation.2010.06.007
PMid:20638769
105. Solevåg AL, Dannevig I, Wyckoff M, Saugstad OD, Nakstad B. Return of spontaneous circulation with a compression: ventilation ratio of 15:2 versus 3:1 in newborn pigs with cardiac arrest due to asphyxia. ArchDis Child Fetal Neonatal Ed 2011; 96:F417-21. https://doi.org/10.1136/adc.2010.200386
PMid:21393311
106. Solevåg AL, Madland JM, Gjærum E, Nakstad B. Minute ventilation at different compression to ventilation ratios, different ventilation rates, and continuous chest compressions with asynchronous ventilation in a newborn manikin. Scand J Trauma Resusc Emerg Med 2012; 20:73. https://doi.org/10.1186/1757-7241-20-73
PMid:23075128 PMCid:PMC3558408
107. Hemway RJ, Christman C, Perlman J. The 3:1 is superior to a 15:2 ratio in a newborn manikin model in terms of quality of chest compressions and number of ventilations. Arch Dis Child Fetal Neonatal Ed 2013; 98:F42-5. https://doi.org/10.1136/archdischild-2011-301334
PMid:22491015
108. Linner R, Werner O, Perez-de-Sa V, Cunha-Goncalves D. Circulatory recovery is as fast with air ventilation as with 100% oxygen after asphyxia-induced cardiac arrest in piglets. Pediatr Res 2009; 66:391-4. https://doi.org/10.1203/PDR.0b013e3181b3b110
PMid:19581834
109. Lipinski CA, Hicks SD, Callaway CW. Normoxic ventilation during resuscitation and outcome from asphyxial cardiac arrest in rats. Resuscitation 1999; 42:221-9. https://doi.org/10.1016/S0300-9572(99)00083-0
110. Perez-de-Sa V, Cunha-Goncalves D, Nordh A, et al. High brain tissue oxygen tension during ventilation with 100% oxygen after fetal asphyxia in newborn sheep. Pediatr Res 2009; 65:57-61. https://doi.org/10.1203/PDR.0b013e31818a01a4
PMid:18703995
111. Solevåg AL, Dannevig I, Nakstad B, Saugstad OD. Resuscitation of severely asphyctic newborn pigs with cardiac arrest by using 21% or 100% oxygen. Neonatology 2010; 98:64-72. https://doi.org/10.1159/000275560
PMid:20068361
112. Temesvári P, Karg E, Bódi I, et al. Impaired early neurologic outcome in newborn piglets reoxygenated with 100% oxygen compared with room air after pneumothorax-induced asphyxia. Pediatr Res 2001; 49:812-9. https://doi.org/10.1203/00006450-200106000-00017
PMid:11385143
113. Walson KH, Tang M, Glumac A, et al. Normoxic versus hyperoxic resuscitation in pediatric asphyxial cardiac arrest: effects on oxidative stress. Crit Care Med 2011; 39:335-43. https://doi.org/10.1097/CCM.0b013e3181ffda0e
PMid:21057313
114. Yeh ST, Cawley RJ, Aune SE, Angelos MG. Oxygen requirement during cardiopulmonary resuscitation (CPR) to effect return of spontaneous circulation. Resuscitation 2009; 80:951-5. https://doi.org/10.1016/j.resuscitation.2009.05.001
PMid:19520479
115. Richmond S, Wyllie J. European Resuscitation Council Guidelines for Resuscitation 2010 Section 7. Resuscitation of babies at birth. Resuscitation 2010; 81:1389-99. https://doi.org/10.1016/j.resuscitation.2010.08.018
PMid:20956046
116. Crespo SG, Schoffstall JM, Fuhs LR, Spivey WH. Comparison of two doses of endotracheal epinephrine in a cardiac arrest model. Ann Emerg Med 1991; 20:230-4. https://doi.org/10.1016/S0196-0644(05)80928-X
117. Jasani MS, Nadkarni VM, Finkelstein MS, et al. Effects of different techniques of endotracheal epinephrine administration in pediatric porcine hypoxichypercarbic cardiopulmonary arrest. Crit Care Med 1994; 22:1174-80. https://doi.org/10.1097/00003246-199407000-00021
PMid:8026209
118. Mielke LL, Frank C, Lanzinger MJ, et al. Plasma catecholamine levels following tracheal and intravenous epinephrine administration in swine. Resuscitation 1998; 36:187-92. https://doi.org/10.1016/S0300-9572(98)00007-0
119. Roberts JR, Greenberg MI, Knaub MA, Kendrick ZV, Baskin SI. Blood levels following intravenous and endotracheal epinephrine administration. JACEP 1979; 8:53-6. https://doi.org/10.1016/S0361-1124(79)80036-2
120. Hörnchen U, Schüttler J, Stoeckel H, Eichelkraut W, Hahn N. Endobronchial instillation of epinephrine during cardiopulmonary resuscitation. Crit Care Med 1987; 15:1037-9. https://doi.org/10.1097/00003246-198711000-00009
PMid:3677746
121. Wyckoff MH, Perlman JM, Laptook AR. Use of volume expansion during delivery room resuscitation in near-term and term infants. Pediatrics 2005; 115:950-5. https://doi.org/10.1542/peds.2004-0913
PMid:15805369
122. Segal S, Anyan WR, Hill RM, Kauffman RE, Mofenson H, Pruitt AW, Shinefield HR, Singer HS, Weinberger MM. Naloxone use in newborns. Pediatrics 1980;65;667
123. Moe-Byrne T1, Brown JV, McGuire W. Naloxone for opiate-exposed newborn infants. Cochrane Database Syst Rev 2013 Feb 28;(2):CD003483.
PMid:23450541
124. Brambrink AM, Ichord RN, Martin LJ, Koehler RC, Traystman RJ. Poor outcome after hypoxia-ischemia in newborns is associated with physiological abnormalities during early recovery. Possible relevance to secondary brain injury after head trauma in infants. Exp Toxicol Pathol 1999; 51:151-62. https://doi.org/10.1016/S0940-2993(99)80089-X
125. Salhab WA, Wyckoff MH, Laptook AR, Perlman JM. Initial hypoglycemia and neonatal brain injury in term infants with severe fetal acidemia. Pediatrics 2004; 114:361-6. https://doi.org/10.1542/peds.114.2.361
PMid:15286217
126. Lee SK, Penner PL, Cox M. Comparison of the attitudes of health care professionals and parents toward active treatment of very low birth weight infants. Pediatrics 1991; 88:110-4. https://doi.org/10.1016/S0890-8567(10)80002-4
127. Harrington DJ, Redman CW, Moulden M, Greenwood CE. The long-term outcome in surviving infants with Apgar zero at 10 minutes: a systematic review of the literature and hospital-based cohort. Am J Obstet Gynecol 2007; 196:463.e1-5. https://doi.org/10.1016/j.ajog.2006.10.877
PMid:17466703
128. Patel H, Beeby PJ. Resuscitation beyond 10 minutes of term babies born without signs of life. J Paediatr Child Health 2004; 40:136-8. https://doi.org/10.1111/j.1440-1754.2004.00314.x
PMid:15009579
129. Casalaz DM, Marlow N, Speidel BD. Outcome of resuscitation following unexpected apparent stillbirth. Arch Dis Child Fetal Neonatal Ed 1998; 78:F112-5. https://doi.org/10.1136/fn.78.2.F112
PMid:9577280 PMCid:PMC1720775
130. Savoldelli GL, Naik VN, Park J, et al. Value of debriefing during simulated crisis management: oral versus video-assisted oral feedback. Anesthesiology 2006; 105:279-85. https://doi.org/10.1097/00000542-200608000-00010
PMid:16871061
131. Edelson DP, Litzinger B, Arora V, et al. Improving in-hospital cardiac arrest process and outcomes with performance debriefing. Arch Intern Med 2008; 168:1063-9. https://doi.org/10.1001/archinte.168.10.1063
PMid:18504334
132. DeVita MA, Schaefer J, Lutz J, Wang H, Dongilli T. Improving medical emergency team (MET) performance using a novel curriculum and a computerized human patient simulator. Qual Saf Health Care 2005; 14:326-31. https://doi.org/10.1136/qshc.2004.011148
PMid:16195564 PMCid:PMC1744065
133. Wayne DB, Butter J, Siddall VJ, et al. Simulation-based training of internal medicine residents in advanced cardiac life support protocols: a randomized trial. Teach Learn Med 2005; 17:210-6. https://doi.org/10.1207/s15328015tlm1703_3
PMid:16042514
134. Clay AS, Que L, Petrusa ER, Sebastian M, Govert J. Debriefi ng in the intensive care unit: a feedback tool to facilitate bedside teaching. Crit Care Med 2007; 35:738-54. https://doi.org/10.1097/01.CCM.0000257329.22025.18
PMid:17255866
135. Blum RH, Raemer DB, Carroll JS, Dufresne RL, Cooper JB. A method for measuring the effectiveness of simulation-based team training for improving communication skills. Anesth Analg 2005; 100:1375-80. https://doi.org/10.1213/01.ANE.0000148058.64834.80
PMid:15845689
136. Schmid MB, Reister F, Mayer B, et al. Prospective risk factor monitoring reduces intracranial hemorrhage rates in preterm infants. Dtsch Arztebl Int 2013; 110:489-96.
PMid:24000297 PMCid:PMC3752580
137. Berden HJ, Willems FF, Hendrick JM, Pijls NH, Knape JT. How frequently should basic cardiopulmonary resuscitation training be repeated to maintain adequate skills? BMJ 1993; 306:1576-7. https://doi.org/10.1136/bmj.306.6892.1576
PMid:8329917 PMCid:PMC1677995
138. Ernst KD, Cline WL, Dannaway DC, et al. Weekly and consecutive day neonatal intubation training: comparable on a pediatrics clerkship. Acad Med 2014; 89:505-10. https://doi.org/10.1097/ACM.0000000000000150
PMid:24448036
139. Kaczorowski J, Levitt C, Hammond M, et al. Retention of neonatal resuscitation skills and knowledge: a randomized controlled trial. Fam Med 1998; 30:705-11.
PMid:9827341
140. Kovacs G, Bullock G, Ackroyd-Stolarz S, Cain E, Petrie D. A randomized controlled trial on the effect of educational interventions in promoting airway management skill maintenance. Ann Emerg Med 2000; 36:301-9. https://doi.org/10.1067/mem.2000.109339
PMid:11020676
141. Montgomery C, Kardong-Edgren SE, Oermann MH, Odom-Maryon T. Student satisfaction and self report of CPR competency: HeartCode BLS courses, instructor-led CPR courses, and monthly voice advisory manikin practice for CPR skill maintenance. Int J Nurs Educ Scholarsh 2012; 9. https://doi.org/10.1515/1548-923X.2361
142. Oermann MH, Kardong-Edgren SE, Odom-Maryon T. Effects of monthly practice on nursing students' CPR psychomotor skill performance. Resuscitation 2011; 82:447-53. https://doi.org/10.1016/j.resuscitation.2010.11.022
PMid:21227563
144. Su E, Schmidt TA, Mann NC, Zechnich AD. A randomized controlled trial to assess decay in acquired knowledge among paramedics completing a pediatric resuscitation course. Acad Emerg Med 2000; 7:779-86. https://doi.org/10.1111/j.1553-2712.2000.tb02270.x
PMid:10917328
145. Sutton RM, Niles D, Meaney PA, et al. "Booster" training: evaluation of instructor-led bedside cardiopulmonary resuscitation skill training and automated corrective feedback to improve cardiopulmonary resuscitation compliance of Pediatric Basic Life Support providers during simulated cardiac arrest. Pediatr Crit Care Med 2011; 12:e116-21. https://doi.org/10.1097/PCC.0b013e3181e91271
PMid:20625336 PMCid:PMC3717252
146. Turner NM, Scheffer R, Custers E, Cate OT. Use of unannounced spaced telephone testing to improve retention of knowledge after life-support courses. Med Teach 2011; 33:731-7. https://doi.org/10.3109/0142159X.2010.542521
PMid:21355700
147. Lubin J, Carter R. The feasibility of daily mannequin practice to improve intubation success. Air Med J 2009; 28:195-7. https://doi.org/10.1016/j.amj.2009.03.006
PMid:19573768
148. Mosley CM, Shaw BN. A longitudinal cohort study to investigate the retention of knowledge and skills following attendance on the Newborn Life support course. Arch Dis Child 2013; 98:582-6. https://doi.org/10.1136/archdischild-2012-303263
PMid:23595225
149. Nadel FM, Lavelle JM, Fein JA, et al. Teaching resuscitation to pediatric residents: the effects of an intervention. Arch Pediatr Adolesc Med 2000; 154:1049-54. https://doi.org/10.1001/archpedi.154.10.1049
PMid:11030858
150. Niles D, Sutton RM, Donoghue A, et al. "Rolling Refreshers": a novel approach to maintain CPR psychomotor skill competence. Resuscitation 2009; 80:909-12. https://doi.org/10.1016/j.resuscitation.2009.04.021
PMid:19467759
151. Nishisaki A, Donoghue AJ, Colborn S, et al. Effect of just-in-time simulation training on tracheal intubation procedure safety in the pediatric intensive care unit. Anesthesiology 2010; 113:214-23. https://doi.org/10.1097/ALN.0b013e3181e19bf2
PMid:20526179
152. O'Donnell CM, Skinner AC. An evaluation of a short course in resuscitation training in a district general hospital. Resuscitation 1993; 26:193-201. https://doi.org/10.1016/0300-9572(93)90179-T
153. Breckwoldt J, Svensson J, Lingemann C, Gruber H. Does clinical teacher training always improve teaching effectiveness as opposed to no teacher training? A randomized controlled study. BMC Med Educ 2014; 14:6. https://doi.org/10.1186/1472-6920-14-6
PMid:24400838 PMCid:PMC3893403
154. Boerboom TB, Jaarsma D, Dolmans DH, et al. Peer group reflection helps clinical teachers to critically reflect on their teaching. Med Teach 2011; 33:e615-23. https://doi.org/10.3109/0142159X.2011.610840
PMid:22022915
155. Litzelman DK, Stratos GA, Marriott DJ, Lazaridis EN, Skeff KM. Beneficial and harmful effects of augmented feedback on physicians' clinical-teaching performances. Acad Med 1998; 73:324-32. https://doi.org/10.1097/00001888-199803000-00022
PMid:9526460
156. Naji SA, Maguire GP, Fairbairn SA, Goldberg DP, Faragher EB. Training clinical teachers in psychiatry to teach interviewing skills to medical students. Med Educ 1986; 20:140-7. https://doi.org/10.1111/j.1365-2923.1986.tb01062.x
PMid:3959930
158. Skeff KM, Stratos G, Campbell M, Cooke M, Jones HW 3rd. Evaluation of the seminar method to improve clinical teaching. J Gen Intern Med 1986; 1:315-22. https://doi.org/10.1007/BF02596211
PMid:3772621
160. Regan-Smith M, Hirschmann K, Iobst W. Direct observation of faculty with feedback: an effective means of improving patient-centered and learner-centered teaching skills. Teach Learn Med 2007; 19:278-86. https://doi.org/10.1080/10401330701366739
PMid:17594224