

Dear Sir,
Superficial siderosis of the central nervous system (SSCNS) is a rare nervous system disorder typically associated with hearing loss, cerebellar ataxia and disturbance of the pyramidal tract. The condition results from damage to the acoustic nerve, cerebellum and spinal cord.(1) Definitive diagnosis is usually made via magnetic resonance (MR) imaging by detecting a hypointense band around the surface of the central nervous system on T2-weighted images. Herein, we describe an unusual case of SSCNS that developed after radiotherapy and did not involve hearing loss or pyramidal tract disturbance.
A 58-year-old woman presented at our hospital after experiencing several generalised tonic-clonic seizures, which started eight months prior to admission. She showed slight gait ataxia but had no pyramidal tract disturbance or signs of hearing loss over the preceding few years. She had received radiotherapy for the treatment of nasopharyngeal carcinoma 23 years ago and did not present with any other risk factors for seizure. The only abnormal finding on physical examination was the slight gait ataxia. Electroencephalography showed findings of sharp waves, and sharp and slow wave complexes, characteristic of epilepsy, in the left temporal lobe. T2-weighted gradient echo (Figs.
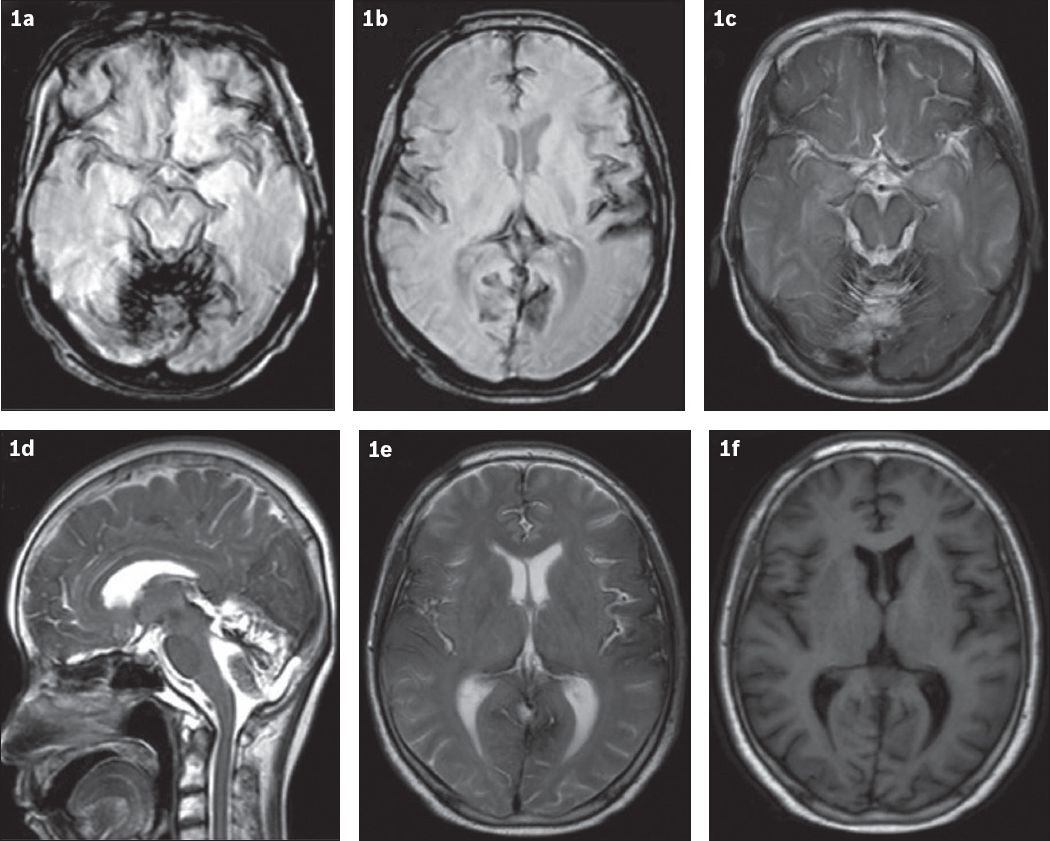
Fig. 1
(a & b) T2-W gradient echo and (c & d) T2-W MR images show hypointensity on the cerebral surface. A hypointense band is also seen around the folia of the posterior fossa and brainstem, together with cerebellar atrophy (in c & d) and around the cerebral falx and sylvian fissure (in e). (f) T1-W MR image shows that the presence of lesions is ambiguous.
The patient’s lack of other seizure risk factors led us to attribute her SSCNS to the previous radiotherapy. Review of her medical records showed that she received an eight-week course of 60Co-γ radiotherapy for pharyngeal carcinoma, which was administered at 700 Gy/week through the pre-auricular field and ancillary to the bilateral infraorbital field.
SSCNS can have various causes, including tumour, back and/or head trauma, arteriovenous malformation and/or aneurysm, postneurosurgery complications, brachial plexus injury and amyloid angiopathy.(2) Approximately half of SSCNS cases arise due to head or spine trauma.(3) Our case, the first of its kind reported in the literature, was unusual in that the patient’s condition appeared to have been triggered by radiotherapy. In addition, she did not present with hearing loss. Hearing loss is only absent in approximately 13% of SSCNS patients, mainly due to sparing of the eighth cranial nerve; the remaining patients present with hearing loss, which is a result of the vulnerability of the acoustic nerve caused by iron deposition.(3) Similar to our case, Wang et al reported a patient who presented with seizures and deafness but no ataxia; the authors suggested that seizures occur predominantly in SSCNS cases.(4) In cases of SSCNS presenting with secondary epilepsy, accumulation of haemosiderin in the subarachnoid space has been shown to irritate the cortical meninges, inducing seizures.(5) This could be the probable aetiology of seizures in our patient. Antiepileptic drugs can be effective in such cases,(6) as was observed in ours.
The present case suggests that radiotherapy can induce SSCNS. Taken together with previous reports, the case highlights that SSCNS could also induce seizures. This information may be useful for clinicians when conducting a differential diagnosis and our case provides evidence for further research into central nervous system-related complications of radiotherapy.
Acknowledgement
This study was supported by the National Natural Science Foundation of China (No. 81160168).
Yours sincerely,