Singapore Med J 2019; 60(6): 270-280 doi: https://doi.org/10.11622/smedj.2019057
A systematic review of the association of obesity with the outcomes of inflammatory rheumatic diseases
Yi Xuan Lee1,*, BSc(Pharm)(Hons), Yu Heng Kwan2,*, BSc(Pharm)(Hons), Ka Keat Lim2, MPharm, MSc, Chuen Seng Tan3, PhD, Nai Lee Lui4, MBBS, MRCP, Jie Kie Phang4, BSc(Hons), Eng Hui Chew1, BSc(Pharm)(Hons), PhD, Truls Ostbye2, MD, PhD, Julian Thumboo4, MBBS, FRCPEd, Warren Fong4, MBBS, MRCP
Author Information >Copyright and License information >
1Department of Pharmacy, National University of Singapore, Singapore 2Programme in Health Services and Systems Research, Duke-NUS Medical School, Singapore 3Saw Swee Hock School of Public Health, National University of Singapore, Singapore 4Department of Rheumatology and Immunology, Singapore General Hospital, Singapore Correspondence: Dr Warren Fong, Consultant, Department of Rheumatology and Immunology, Singapore General Hospital, Academia, Level 4, 20 College Road, Singapore 169856. warren.fong.w.s@singhealth.com.sg
This was a systematic review of the literature on the association between obesity and the outcome of inflammatory rheumatic diseases. We conducted a literature search using PubMed®, Embase and PsycINFO®. Articles were classified into three categories based on the effects of obesity on the outcomes of inflammatory rheumatic diseases. The subject population, country, type of studies, number of patients, measurement of obesity and outcomes assessed were presented. Quality was appraised using Kmet et al’s criteria. 4,331 articles were screened and 60 were relevant to the objective. Obesity had a negative, positive and neutral association with outcomes of inflammatory rheumatic diseases in 38 (63.3%) studies with 57,612 subjects, 11 (18.3%) studies with 3,866 subjects, and 11 (18.3%) studies with 3,834 subjects, respectively. In most studies, the disease population had been diagnosed with rheumatoid arthritis (RA). Tumour necrosis factor-α inhibitors were mostly associated with negative outcomes. More studies examining subjects outside Europe and North America and diseases other than RA are warranted.
Inflammatory rheumatic diseases, such as rheumatoid arthritis (RA), psoriatic arthritis (PsA) and spondyloarthritis (SpA), are usually progressive and associated with pain. Comorbidities may occur in association with rheumatic diseases.(1) If inflammatory rheumatic diseases are not treated appropriately, daily activities will be affected. Disease-modifying antirheumatic drugs (DMARDs), including conventional synthetic DMARDs and biologic DMARDs (bDMARDs), have been used to decrease pain and inflammation, reduce or prevent joint damage, and preserve joint structure and function.
Outcomes of inflammatory rheumatic diseases can be assessed mainly by two ways – patient-reported outcomes (PROs) and clinical outcomes. Most clinical outcomes involve clinical assessment or laboratory investigations by the healthcare provider. On the other hand, PROs are directly reported by the patient, without requiring interpretation by others. PROs add valuable and unique information on treatment efficacy and quality of life that is immediately relevant to the management of disease activity. Examples of PROs include the Health Assessment Questionnaire (HAQ) for RA and the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) for SpA.(2,3) In terms of clinical use, a predictive factor is any measurable attribute of an individual that can be used to infer a health-related outcome.
Obesity is increasing in prevalence, with over 600 million adults worldwide being obese. Overweight is defined as a body mass index (BMI) greater than or equal to 25 kg/m2, while obesity refers to a BMI greater than or equal to 30 kg/m2.(4) As Asian populations have different associations among BMI, percentage of body fat, and health risks compared to European populations, a lower BMI cut-off is often used. Asians with a BMI above 23 kg/m2 are considered to be overweight, while a BMI of above or equal to 25 kg/m2 is considered to be obese. Non-communicable comorbidities such as cardiovascular diseases, diabetes mellitus and musculoskeletal disorders have been associated with obesity.(4)
Overall, the prevalence of obesity in many inflammatory rheumatic diseases seems to be similar or slightly higher than in the general population.(5) The excessive fats in adipose tissues cause the release of inflammatory mediators such as tumour necrosis factor-a (TNF-a) and interleukin,(6) predisposing the body to a pro-inflammatory state.(7) Obesity may impair mobility of the thoracic spine, and an increase in adipose tissue is associated with the increased of production pro-inflammatory cytokines,(6) which may lead to worsening of the inflammatory rheumatic diseases. Furthermore, patients with RA tend to have high rates of cardiovascular morbidity and mortality;(8) obesity further increases this risk.
Several recent studies found an increased risk of RA occurrence related to obesity, while no longitudinal studies were found for other inflammatory rheumatic disease.(9) RA patients have an altered body composition, with decreased lean mass and increased fat mass. This may adversely affect the reliability of conventional BMI cut-offs used to define obesity. Although lower thresholds of BMI have been proposed, these thresholds are not applied in published clinical studies.(9)
To date, there have been numerous conflicting studies regarding the effects of obesity on the outcomes of RA.(10,11) In addition, studies reporting the effects of obesity on the outcomes of other inflammatory rheumatic diseases such as SpA are lacking. However, to the best of our knowledge, there has been no systematic review on the association of obesity with the outcomes of inflammatory rheumatic diseases. Therefore, this article aimed to provide a systematic review of the current literature on how obesity is associated with the outcomes of RA, SpA, ankylosing spondylitis (AS), systemic lupus erythematosus (SLE) and PsA. This systematic review can provide clinicians and researchers with a clearer understanding of the impact of obesity on inflammatory rheumatic diseases.
METHODS
We conducted a systematic review in accordance with the Preferred Reporting Items for Systemic reviews and Meta-Analysis (PRISMA) checklist, but we did not lodge a protocol. We searched the literature using the electronic databases Embase®, PubMed® and PsycINFO®. Hand searches were carried out using the references of the related articles. The databases were searched from their inception to September 2018. The keywords used were: ((obes* OR (body mass index) OR weight)) AND ((clinical outcomes) OR (treatment outcomes) OR (patient-reported outcomes) OR outcomes)) AND ((spondyloarthritis) OR (systemic lupus erythematosus) OR (psoriatic arthritis) OR (Sjogren’s syndrome) OR (ankylosing spondylitis) OR (inflammatory bowel disease related to arthritis) OR rheum*)).
Two independent reviewers reviewed both the article inclusion and data extraction process. The inclusion criteria were English peer-reviewed journals that studied adults aged ≥ 18 years with all autoimmune rheumatic diseases and sought to determine the effect of obesity on outcomes. Systematic reviews, meta-analyses, case series, case reports, grey articles and unpublished articles were excluded from the review. Non-English studies as well as studies that investigated autoimmune or rheumatic disease in subjects aged < 18 years were also excluded.
Articles were then classified into three main categories based on the effect of obesity on the outcomes of the autoimmune rheumatic diseases. Studies that showed positive associations that were statistically significant were classified as positive, those that showed negative associations that were statistically significant were classified as negative, and studies that showed no statistical significance were classified as neutral. Data such as subject population, country of study, type of study, number of patients, measurement of obesity and outcomes assessed was extracted, tabulated and presented accordingly. We also rated the quality of the studies found using the standard quality assessment criteria detailed by Kmet et al in 2004.(12) Although no threshold was set for this systematic review, a score of above 0.75 was considered good, with a higher score representing better quality.
RESULTS
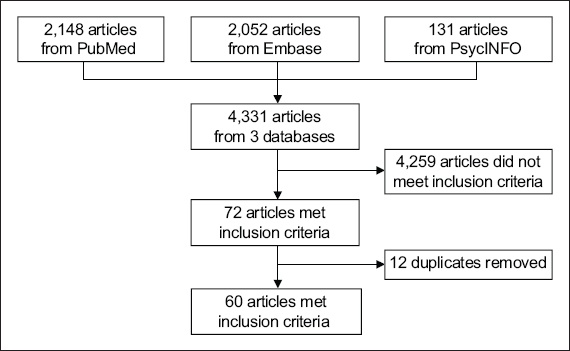
A total of 4,331 articles were retrieved from the three databases, consisting of 2,148, 2,052 and 131 articles from PubMed®, Embase and PsycINFO®, respectively. Fig. 1 shows the selection process. Out of these 4,331 articles, only 72 articles met the inclusion criteria outlined in our study. The other 4,259 articles did not meet our inclusion criteria, were not related to obesity or were not about autoimmune rheumatic diseases. After removing 12 duplicates, 60 articles were included in our review. Out of these 60 articles, 26 (43.3%) were cohort studies and 34 (56.7%) were cross-sectional studies.
Fig. 1
Flowchart shows selection of articles for review.
Positive association with outcome
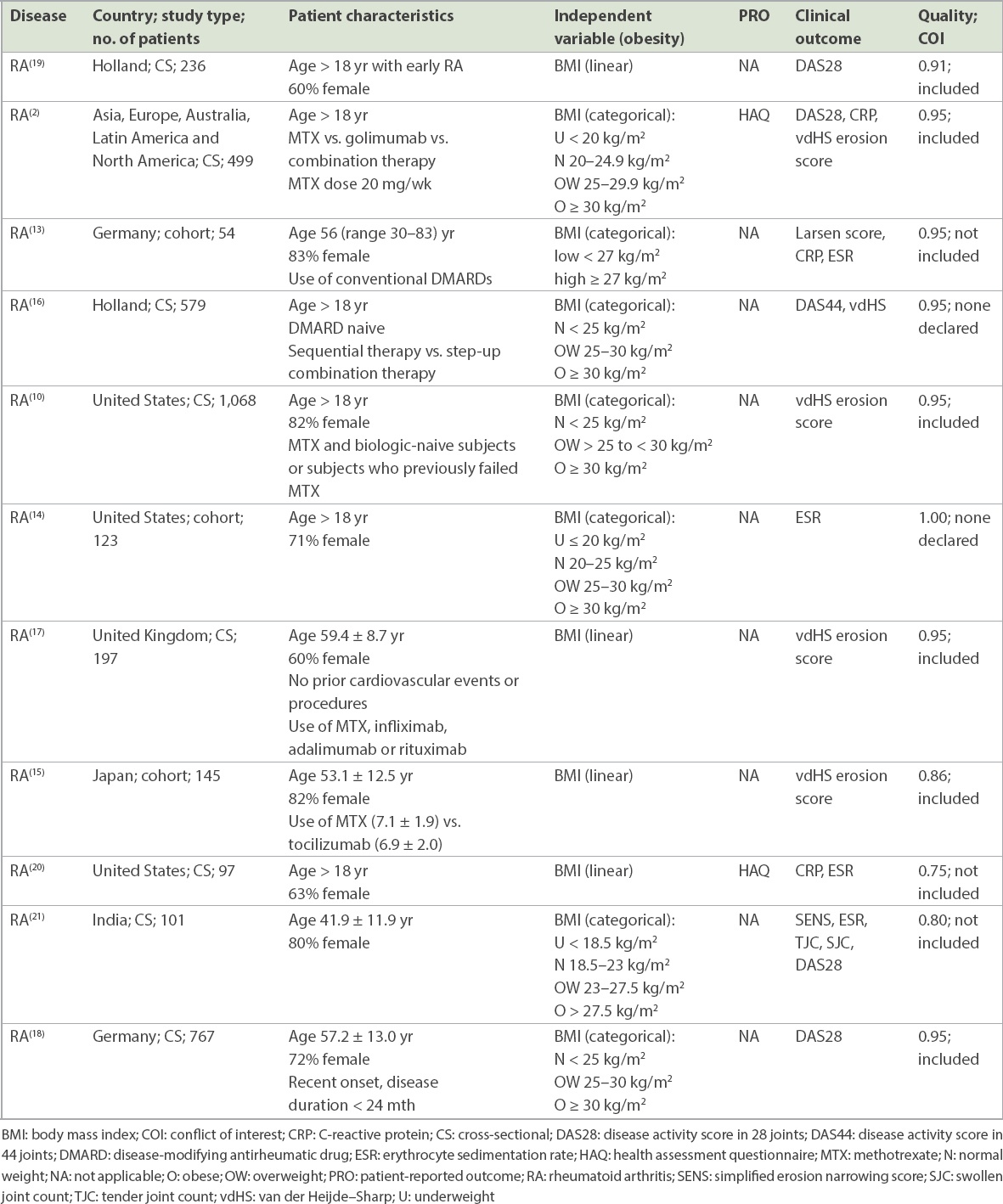
From the search, it was found that a total of 11 studies with 3,866 subjects showed that obesity is significantly associated with better outcome (Table I).(2,10,13-21) All of the 11 studies were focused on the RA disease population. Most of these studies were conducted in Western populations based in America and Europe, with only three investigating Asian subjects. Van der Heijde–Sharp (vdHS) erosion scores were the most commonly used clinical outcome. Other clinical outcomes included C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), simplified erosion narrowing score, tender joint count (TJC), disease activity score in 28 joints (DAS28), disease activity score in 44 joints, Larsen score and swollen joint count (SJC). PROs were assessed using the HAQ. Out of the 11 studies, 8 (72.7%) were cross-sectional studies, while 3 (27.3%) were cohort studies.
Table I
Studies that show a positive association between obesity and outcome (n = 3,866).
Neutral association with outcome
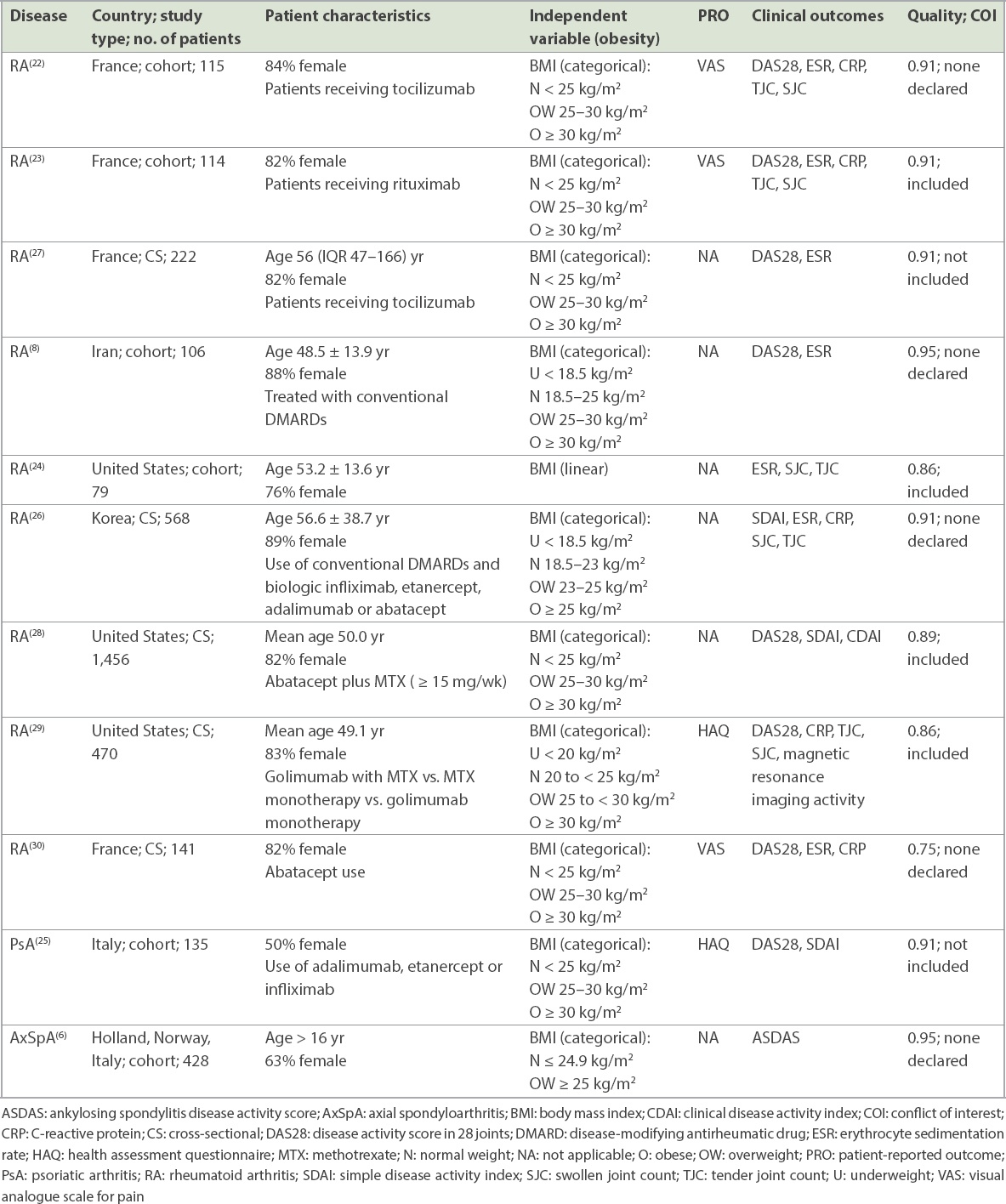
A total of 11 studies with 3,834 subjects showed that obesity was neither associated with better nor worse outcomes, with insignificant associations reported (Table II).(6,8,22-30) Most of the studies investigated the RA disease population. For PsA and axial SpA (AxSpA), one study was found for each disease population. Again, most of the studies were conducted on subjects from Western populations, and only one study was conducted in Asia. For the RA studies, clinical outcome DAS28 was the most commonly used. PROs used included the visual analogue scale for pain (VAS) and HAQ. Clinical outcomes included CRP, ESR, simple disease activity index (SDAI), TJC and SJC. For the PsA study, SDAI, DAS28 or HAQ was used. For the AxSpA study, the AS disease activity score was used. Out of the 11 studies, 5 (45.5%) studies were cross-sectional studies, while 6 (54.5%) were cohort studies.
Table II
Studies that show a neutral association between obesity and outcome (n = 3,834).
Negative association with outcome
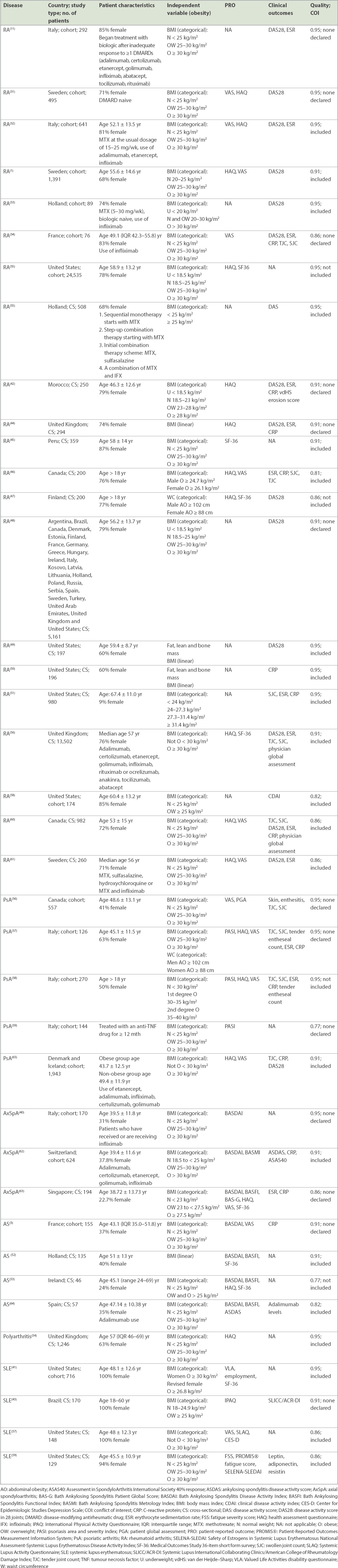
A total of 38 studies with 57,612 subjects showed that obesity is significantly associated with worse outcomes (Table III).(1,3,11,31-65) 21 studies were focused on the RA disease population, while five studies assessed PsA patients, and another four studies examined the AS disease population. There were three studies on AxSpA, four studies on SLE and one study on polyarthritis. Most of the studies were conducted on Western populations with limited studies based on Asian populations. For RA studies, the clinical outcome DAS28 was also the most commonly used. PROs used included VAS and HAQ. Clinical outcomes included CRP, ESR, TJC, SJC and vdHS erosion score. For PsA studies, TJC, SJC, Psoriasis Area and Severity Index score, HAQ, VAS, patient global assessment, ESR, CRP and tender entheseal count were used. For AS studies, BASDAI was the most commonly used PRO; other instruments used included the Bath AS Functional Index, AS disease activity score, VAS and the 36-Item Short Form Health Survey (i.e. SF-36). For the AxSpA studies, BASDAI was used, and for the polyarthritis study, HAQ was used. For the SLE studies, employment, International Physical Activity Questionnaire, SLICC/ACR-DI (Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index) and Valued Life Activities disability questionnaire were used. Out of the 38 studies, 21 (55.3%) were cross-sectional studies and 17 (44.7%) were cohort studies.
Table III
Studies that show a negative association between obesity and outcome (n = 57,612).
Rheumatoid arthritis studies
Out of the 60 studies, 41 (68.3%) studies were conducted in the RA population. Among these 41 studies, 11 (26.8%) found that obesity was associated with a positive outcome in the RA population. In another 9 (22.0%) RA studies, obesity was associated with a neutral outcome, while 21 (51.2%) RA studies found that it was associated with a negative outcome. Only 4 (9.8%) of the 41 RA studies were conducted in Asian populations.
Quality assessment
All studies achieved a score of at least 0.75. 41 (68.3%) of the studies achieved a score of more than 0.90, showing that all studies included were of good quality.
DISCUSSION
This study comprehensively reviewed the available literature on the association of obesity with the outcomes of inflammatory rheumatic diseases. We also closely followed the PRISMA checklist for reporting systematic reviews. As far as we know, there is no systematic review regarding the association between obesity and the outcomes of inflammatory rheumatic diseases. Our study gives an overview of the studies that provided evidence that obesity could have a positive, neutral or negative association with the outcomes of autoimmune rheumatic disease. We also found the number of studies done on various types of inflammatory rheumatic diseases.
Out of the 60 studies, 38 (63.3%), 11 (18.3%) and 11 (18.3%) studies showed that obesity is negatively associated, not associated and positively associated, respectively, with the outcomes of autoimmune rheumatic disease. No studies on PsA, AS, AxSpA, SLE and polyarthritis showed that obesity had a positive association with outcomes. However, given that the number of studies in these areas is limited and that the populations studied are not very varied, with different outcomes used for evaluation, this information may not be sufficient to draw the conclusion that obesity only has a negative association with these diseases.
Most of the studies were completed in countries in the West, including America and European countries. Only four out of 41 RA studies were conducted in Asia. The body composition of Asians is different from that of Caucasians. Asians may have higher body fat at a specific BMI as compared to Caucasians;(4) as such, the definition of obesity in various studies may not be applicable to Asians. The various BMI categories for Asians have been defined as: < 18.5 kg/m2 for underweight, 18.5–22.9 kg/m2 for normal weight, 23.0–24.9 kg/m2 for overweight and ≥ 25 kg/m2 for obese,(4) which is different from the international definitions. Furthermore, as ethnicity may result in variability in responses to drug therapy, Asians and Caucasians may respond differently to medications. Therefore, we may not be able to conclude from this study that obesity is negatively associated with the outcome of RA in an Asian setting.
Although some of the included RA studies had a methotrexate arm, the dosing of methotrexate varied from study to study. Methotrexate dosing is usually based on a balance of efficacy and tolerability. The dose in one of the studies conducted in the Japanese population was 7.1 ± 1.9 mg/week,(15) while the dose in an Italian study was 15–25 mg/week.(32) As Asians are likely to have a smaller body surface area compared to the Western population, a lower methotrexate dose may be tolerated, thus possibly favouring the study drug in those studies conducted in Asian populations.
bDMARDs that were used in the included studies can be categorised into three classes: TNF-a inhibitors, B-cell targeted therapies and interleukin-6 (IL-6) inhibitors. TNF-a is a cytokine that results in inflammation and bone degradation, and TNF-a inhibitors include adalimumab, etanercept, infliximab and golimumab. The effects of a TNF-a inhibitor may be dependent on TNF-a expression in synovial joints and infiltration by inflammatory cells that produce TNF-a.(66) B-cell targeted therapy includes rituximab, a chimeric monoclonal antibody that targets the CD20 surface molecule of some B cells. Its mechanism of action in RA is not completely understood.(67) IL-6 inhibitors, comprising the relatively new agent tocilizumab, inhibit IL-6-mediated signalling and induce B-regulatory cells, decreasing pro-inflammatory cytokines.(68)
We found that the studies involving TNF-a inhibitors were associated with different outcomes: four studies(2,10,16,17) were associated with positive outcomes, three studies(25,26,29) with neutral outcomes and ten studies(11,32-34,40,55,56,61,62,65) with negative outcomes. Rituximab was associated with positive,(17) neutral(23) and negative(11,56) outcomes, while tocilizumab was similarly associated with positive,(15) neutral(22,27) and negative(11,56) outcomes. Due to the limited number of studies for tocilizumab, we conducted an additional literature search on it and found that tocilizumab is unlikely to be affected by obesity.(69) An alternative modality for RA is abatacept, a selective modulator that targets the CD80/CD86:CD28 pathway that is needed for complete activation of T cells. The relevant studies showed neutral(26,28,30) or negative(11,56) outcomes. However, the two studies in which rituximab, tocilizumab and abatacept were associated with negative outcomes(11,56) were conducted in populations with refractory disease, and thus obesity was unlikely to be the only reason for the lack of response. Further studies are needed to determine if obesity is indeed associated with negative outcomes for patients on rituximab, tocilizumab or abatacept.
A relatively new drug, tofacitinib, is a potent selective Janus kinase (JAK) inhibitor that preferentially inhibits JAK1 and JAK3. Tofacitinib was found to be non-inferior to adalimumab, although more studies are needed to determine its place in therapy.(70) As tofacitinib is oral therapy, it may be more acceptable than bDMARDs. To our knowledge, there are currently no studies to determine if tofacitinib efficacy is affected by obesity, and more studies are needed in this area.
Apart from having a direct impact on inflammation, obesity may modify the pharmacokinetics of bDMARDs. Studies have identified high body weight as a risk factor associated with increased clearance of TNF-a inhibitors, leading to lower serum trough concentration and shorter half-life,(71) which may explain the greater number of studies that associate RA with negative outcomes.
It is interesting to note that cross-sectional studies made up 73%, 46% and 55% of the studies, respectively, that showed positive outcomes, neutral outcomes and negative outcomes associated with obesity. As cross-sectional studies are generally regarded as weaker study designs than cohort studies,(72) this should be taken into consideration when interpreting the results that linked obesity to positive outcomes.
Using the quality assessment criteria, we found that the included studies were generally of good quality, with all studies achieving a score more than 0.75.(12) However, some studies did not include a conflict of interest section and we could not evaluate potential bias arising from it.
A limitation of the present study is that it is a systematic review and not a meta-analysis of the effect of obesity on the outcomes of inflammatory rheumatic diseases; hence, we do not know the aggregate level of the effect of obesity on the outcome. However, we have summarised the literature as much as possible. Another weakness is that non-English articles have been excluded. Nevertheless, the number of non-English articles in this area is limited. Although we sought to carry out a systematic review on inflammatory rheumatic diseases using thorough and comprehensive keywords, the search results only yielded the particular diseases we have listed.
In conclusion, a systematic review was conducted and 60 articles that met the inclusion criteria were selected. Further studies focused on examining Asian populations suffering from RA as well as other inflammatory rheumatic diseases are warranted.
References Ajeganova S, Andersson ML, Hafström I.BARFOT Study GroupAssociation of obesity with worse disease severity in rheumatoid arthritis as well as with comorbidities:a long-term followup from disease onset.Arthritis Care Res (Hoboken). 2013;65:78-87. Baker JF, George M, Baker DG, et al. Associations between body mass, radiographic joint damage, adipokines and risk factors for bone loss in rheumatoid arthritis.Rheumatology (Oxford). 2011;50:2100-7. Ottaviani S, Allanore Y, Tubach F, et al. Body mass index influences the response to infliximab in ankylosing spondylitis.Arthritis Res Ther. 2012;14:R115. WHO Expert ConsultationAppropriate body-mass index for Asian populations and its implications for policy and intervention strategies.Lancet. 2004;363:157-63. Erratum in:Lancet 2004;363:p902. Gremese E, Tolusso B, Gigante MR, Ferraccioli G.Obesity as a risk and severity factor in rheumatic diseases (autoimmune chronic inflammatory diseases).Front Immunol. 2014;5:576. Rubio Vargas R, van den Berg R, van Lunteren M, et al. Does body mass index (BMI) influence the Ankylosing Spondylitis Disease Activity Score in axial spondyloarthritis?: Data from the SPACE cohort.RMD Open. 2016;2:e000283. Ellulu M S, Patimah I, Khaza'ai H, Rahmat A, Abed Y.Obesity and inflammation:the linking mechanism and the complications.Arch Med Sci. 2017;13:851-63. Mirpoaan M, Salesi M, Abdolahi H, Farajzadegan Z, Karimzadeh H.The association of body mass index with disease activity and clinical response to combination therapy in patients with rheumatoid arthritis.J Res Med Sci. 2014;19:509-14. Daïen CI, Sellam J.Obesity and inflammatory arthritis:impact on occurrence, disease characteristics and therapeutic response.RMD Open. 2015;1:e000012. Baker JF, Ostergaard M, George M, et al. Greater body mass independently predicts less radiographic progression on X-ray and MRI over 1-2 years.Ann Rheum Dis. 2014;73:1923-8. Iannone F, Fanizzi R, Notarnicola A, et al. Obesity reduces the drug survival of second line biological drugs following a first TNF-a inhibitor in rheumatoid arthritis patients.Joint Bone Spine. 2015;82:187-91. Kmet LM, Lee R, Cook LS. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of FieldsEdmonton Alberta Heritage Foundation for Medical Research, 2004. Kaufmann J, Kielstein V, Kilian S, Stein G, Hein G.Relation between body mass index and radiological progression in patients with rheumatoid arthritis.J Rheumatol. 2003;30:2350-5. Escalante A, Haas RW, del Rincon I.Paradoxical effect of body mass index on survival in rheumatoid arthritis:role of comorbidity and systemic inflammation.Arch Intern Med. 2005;165:1624-9. Hashimoto J, Garnero P, van der Heijde D, et al. A combination of biochemical markers of cartilage and bone turnover, radiographic damage and body mass index to predict the progression of joint destruction in patients with rheumatoid arthritis treated with disease-modifying anti-rheumatic drugs.Mod Rheumatol. 2009;19:273-82. van der Helm-van Mil AH, van der Kooij SM, Allaart CF, Toes RE, Huizinga TW.A high body mass index has a protective effect on the amount of joint destruction in small joints in early rheumatoid arthritis.Ann Rheum Dis. 2008;67:769-74. Giles JT, Allison M, Bingham CO, 3rdScott WM, JrBathon JM.Adiponectin is a mediator of the inverse association of adiposity with radiographic damage in rheumatoid arthritis.Arthritis Rheum. 2009;61:1248-56. Westhoff G, Rau R, Zink A.Radiographic joint damage in early rheumatoid arthritis is highly dependent on body mass index.Arthritis Rheum. 2007;56:3575-82. Jurgens MS, Jacobs JW, Geenen R, et al. Utrecht Arthritis Cohort Study GroupIncrease of body mass index in a tight controlled methotrexate-based strategy with prednisone in early rheumatoid arthritis:side effect of the prednisone or better control of disease activity?.Arthritis Care Res (Hoboken). 2013;65:88-93. Munro R, Capell H.Prevalence of low body mass in rheumatoid arthritis:association with the acute phase response.Ann Rheum Dis. 1997;56:326-9. Velpula UD, Agrawal S, Thomas J, et al. Low body mass index is adversely associated with radiographic joint damage in Indian patients with early rheumatoid arthritis.J Rheumatol. 2011;38:434-8. Gardette A, Ottaviani S, Sellam J, et al. Body mass index and response to tocilizumab in rheumatoid arthritis:a real life study.Clin Rheumatol. 2016;35:857-61. Ottaviani S, Gardette A, Roy C, et al. Body mass index and response to rituximab in rheumatoid arthritis.Joint Bone Spine. 2015;82:432-6. Morgan SL, Anderson AM, Hood SM, et al. Nutrient intake patterns, body mass index, and vitamin levels in patients with rheumatoid arthritis.Arthritis Care Res. 1997;10:9-17. Iannone F, Fanizzi R, Scioscia C, Anelli MG, Lapadula G.Body mass does not affect the remission of psoriatic arthritis patients on anti-TNF-a therapy.Scand J Rheumatol. 2013;42:41-4. Choe JY, Bae J, Lee H, Park SH, Kim SK.Lack association of body mass index with disease activity composites of rheumatoid arthritis in Korean population:cross-sectional observation.Clin Rheumatol. 2014;33:485-92. Pers YM, Godfrin-Valnet M, Lambert J, et al. Response to tocilizumab in rheumatoid arthritis is not influenced by the body mass index of the patient.J Rheumatol. 2015;42:580-4. D'Agostino M, Alten R, Mysler E, et al. Body mass index and clinical response to intravenous or subcutaneous abatacept in patients with rheumatoid arthritis.Clin Rheumatol. 2017;36:2655-65. George MD, Østergaard M, Conaghan PG, et al. Obesity and rates of clinical remission and low MRI inflammation in rheumatoid arthritis.Ann Rheum Dis. 2017;76:1743-6. Gardette A, Ottaviani S, Sellam J, et al. Body mass index and response to abatacept in rheumatoid arthritis.Eur J Clin Invest. 2016;46:1048-52. Sandberg ME, Bengtsson C, Kallberg H, et al. Overweight decreases the chance of achieving good response and low disease activity in early rheumatoid arthritis.Ann Rheum Dis. 2014;73:2029-33. Gremese E, Carletto A, Padovan M, et al. Gruppo Italiano di Studio sulle Early Arthritis (GISEA)Obesity and reduction of the response rate to anti-tumor necrosis factor a in rheumatoid arthritis:an approach to a personalized medicine.Arthritis Care Res (Hoboken). 2013;65:94-100. Klaasen R, Wijbrandts CA, Gerlag DM, Tak PP.Body mass index and clinical response to infliximab in rheumatoid arthritis.Arthritis Rheum. 2011;63:359-64. Ottaviani S, Gardette A, Tubach F, et al. Body mass index and response to infliximab in rheumatoid arthritis.Clin Exp Rheumatol. 2015;33:478-83. Wolfe F, Michaud K.Effect of body mass index on mortality and clinical status in rheumatoid arthritis.Arthritis Care Res (Hoboken). 2012;64:1471-9. Eder L, Thavaneswaran A, Chandran V, Cook RJ, Gladman DD.Obesity is associated with a lower probability of achieving sustained minimal disease activity state among patients with psoriatic arthritis.Ann Rheum Dis. 2015;74:813-7. Di Minno MN, Peluso R, Iervolino S, et al. CaRRDs Study GroupWeight loss and achievement of minimal disease activity in patients with psoriatic arthritis starting treatment with tumour necrosis factor a blockers.Ann Rheum Dis. 2014;73:1157-62. Di Minno MN, Peluso R, Iervolino S, et al. Obesity and the prediction of minimal disease activity:a prospective study in psoriatic arthritis.Arthritis Care Res (Hoboken). 2013;65:141-7. Cassano N, Galluccio A, De Simone C, et al. Influence of body mass index, comorbidities and prior systemic therapies on the response of psoriasis to adalimumab:an exploratory analysis from the APHRODITE data.J Biol Regul Homeost Agents. 2008;22:233-7. Gremese E, Bernardi S, Bonazza S, et al. Body weight, gender and response to TNF-a blockers in axial spondyloarthritis.Rheumatology (Oxford). 2014;53:875-81. Katz P, Yazdany J, Julian L, et al. Impact of obesity on functioning among women with systemic lupus erythematosus.Arthritis Care Res (Hoboken). 2011;63:1357-64. Ibn Yacoub Y, Amine B, Laatiris A, et al. Prevalence of overweight in Moroccan patients with rheumatoid arthritis and its relationships with disease features.Clin Rheumatol. 2012;31:479-82. Moura dos Santos Fde M, Borges MC, Telles RW, Correia MI, Lanna CC.Excess weight and associated risk factors in patients with systemic lupus erythematosus.Rheumatol Int. 2013;33:681-8. Stavropoulos-Kalinoglou A, Metsios GS, Panoulas VF, et al. Underweight and obese states both associate with worse disease activity and physical function in patients with established rheumatoid arthritis.Clin Rheumatol. 2009;28:439-44. Garcia-Poma A, Segami MI, Mora CS, et al. Obesity is independently associated with impaired quality of life in patients with rheumatoid arthritis.Clin Rheumatol. 2007;26:1831-5. Colmegna I, Hitchon CA, Bardales MC, Pa L, Bartlett SJ.High rates of obesity and greater associated disability among people with rheumatoid arthritis in Canada.Clin Rheumatol. 2016;35:457-60. Uutela T, Kautiainen H, Järvenpää S, et al. Waist circumference based abdominal obesity may be helpful as a marker for unmet needs in patients with RA.Scand J Rheumatol. 2014;43:279-85. Jawaheer D, Olsen J, Lahiff M, et al. QUEST-RAGender, body mass index and rheumatoid arthritis disease activity:results from the QUEST-RA Study.Clin Exp Rheumatol. 2010;28:454-61. Giles JT, Bartlett SJ, Andersen RE, Fontaine KR, Bathon JM.Association of body composition with disability in rheumatoid arthritis:impact of appendicular fat and lean tissue mass.Arthritis Rheum. 2008;59:1407-15. Giles JT, Bartlett SJ, Andersen R, et al. Association of body fat with C-reactive protein in rheumatoid arthritis.Arthritis Rheum. 2008;58:2632-41. Caplan L, Davis LA, Bright CM, et al. Body mass index and the rheumatoid arthritis swollen joint count:an observational study.Arthritis Care Res (Hoboken). 2013;65:101-6. van Genderen S, Boonen A, van der Heijde D, et al. Accelerometer quantification of physical activity and activity patterns in patients with ankylosing spondylitis and population Controls.J Rheumatol. 2015;42:2369-75. Durcan L, Wilson F, Conway R, Cunnane G, O'Shea FD.Increased body mass index in ankylosing spondylitis is associated with greater burden of symptoms and poor perceptions of the benefits of exercise.J Rheumatol. 2012;39:2310-4. Humphreys JH, Verstappen SM, Mirjafari H, et al. Association of morbid obesity with disability in early inflammatory polyarthritis:results from the Norfolk Arthritis Register.Arthritis Care Res (Hoboken). 2013;65:122-6. Heimans L, van den Broek M, le Cessie S, et al. Association of high body mass index with decreased treatment response to combination therapy in recent-onset rheumatoid arthritis patients.Arthritis Care Res (Hoboken). 2013;65:1235-42. Kearsley-Fleet L, Davies R, De Cock D, et al. BSRBR-RA Contributors GroupBiologic refractory disease in rheumatoid arthritis:results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis.Ann Rheum Dis. 2018;77:1405-12. Patterson SL, Schmajuk G, Jafri K, Yazdany J, Katz P.Obesity is independently associated with worse patient-reported outcomes in women with systemic lupus erythematosus.Arthritis Care Res (Hoboken). 2019;71:126-33. Kreps DJ, Halperin F, Desai SP, et al. Association of weight loss with improved disease activity in patients with rheumatoid arthritis:a retrospective analysis using electronic medical record data.Int J Clin Rheumtol. 2018;13:1-10. Mahieu MA, Ahn GE, Chmiel JS, et al. Serum adipokine levels and associations with patient-reported fatigue in systemic lupus erythematosus.Rheumatol Int. 2018;38:1053-61. Schulman E, Bartlett SJ, Schieir O, et al. CATCH InvestigatorsOverweight, obesity, and the likelihood of achieving sustained remission in early rheumatoid arthritis:results from a multicenter prospective cohort study.Arthritis Care Res (Hoboken). 2018;70:1185-91. Levitsky A, Brismar K, Hafström I, et al. Obesity is a strong predictor of worse clinical outcomes and treatment responses in early rheumatoid arthritis:results from the SWEFOT trial.RMD Open. 2017;3:e000458. Micheroli R, Hebeisen M, Wildi LM, et al. Rheumatologists of the Swiss Clinical Quality Management ProgramImpact of obesity on the response to tumor necrosis factor inhibitors in axial spondyloarthritis.Arthritis Res Ther. 2017;19:164. Lee YX, Kwan YH, Png WY, et al. Association of obesity with patient-reported outcomes in patients with axial spondyloarthritis:a cross-sectional study in an urban Asian population.Clin Rheumatol. 2017;36:2365-70. Rosas J, Llinares-Tello F, Senabre-Gallego JM, et al. and the AIRE-MB GroupObesity decreases clinical efficacy and levels of adalimumab in patients with ankylosing spondylitis.Clin Exp Rheumatol. 2017;35:145-8. Højgaard P, Glintborg B, Kristensen LE, et al. The influence of obesity on response to tumour necrosis factor-a inhibitors in psoriatic arthritis:results from the DANBIO and ICEBIO registries.Rheumatology (Oxford). 2016;55:2191-9. Ma X, Xu S.TNF inhibitor therapy for rheumatoid arthritis.Biomed Rep. 2013;1:177-84. Cohen MD, Keystone E.Rituximab for rheumatoid arthritis.Rheumatol Ther. 2015;2:99-111. Scott LJ.Tocilizumab:a review in rheumatoid arthritis.Drugs. 2017;77:1865-79. Shan J, Zhang J.Impact of obesity on the efficacy of different biologic agents in inflammatory diseases:a systematic review and meta-analysis.Joint Bone Spine. 2019;86:173-83. Dhillon S.Tofacitinib:a review in rheumatoid arthritis.Drugs. 2017;77:1987-2001. Singh S, Facciorusso A, Singh AG, et al. Obesity and response to anti-tumor necrosis factor-a agents in patients with select immune-mediated inflammatory diseases:a systematic review and meta-analysis.PLoS One. 2018;13:e0195123. Murad MH, Asi N, Alsawas M, Alahdab F.New evidence pyramid.Evid Based Med. 2016;21:125-7.
REFERENCES:
1. Ajeganova S, Andersson ML, Hafström I; BARFOT Study Group. Association of obesity with worse disease severity in rheumatoid arthritis as well as with comorbidities: a long-term followup from disease onset. Arthritis Care Res (Hoboken) 2013; 65:78-87. https://doi.org/10.1002/acr.21710
PMid:22514159
2. Baker JF, George M, Baker DG, et al. Associations between body mass, radiographic joint damage, adipokines and risk factors for bone loss in rheumatoid arthritis. Rheumatology (Oxford) 2011; 50:2100-7. https://doi.org/10.1093/rheumatology/ker294
PMid:21890621
3. Ottaviani S, Allanore Y, Tubach F, et al. Body mass index influences the response to infliximab in ankylosing spondylitis. Arthritis Res Ther 2012; 14:R115. https://doi.org/10.1186/ar3841
PMid:22584116 PMCid:PMC3446492
4. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004; 363:157-63. Erratum in: Lancet 2004; 363:902. https://doi.org/10.1016/S0140-6736(03)15268-3
5. Gremese E, Tolusso B, Gigante MR, Ferraccioli G. Obesity as a risk and severity factor in rheumatic diseases (autoimmune chronic inflammatory diseases). Front Immunol 2014; 5:576. https://doi.org/10.3389/fimmu.2014.00576
PMid:25426122 PMCid:PMC4227519
6. Rubio Vargas R, van den Berg R, van Lunteren M, et al. Does body mass index (BMI) influence the Ankylosing Spondylitis Disease Activity Score in axial spondyloarthritis?: Data from the SPACE cohort. RMD Open 2016; 2:e000283. https://doi.org/10.1136/rmdopen-2016-000283
PMid:27403336 PMCid:PMC4932251
7. Ellulu M S, Patimah I, Khaza'ai H, Rahmat A, Abed Y. Obesity and inflammation: the linking mechanism and the complications. Arch Med Sci 2017; 13:851-63. https://doi.org/10.5114/aoms.2016.58928
PMid:28721154 PMCid:PMC5507106
8. Mirpourian M, Salesi M, Abdolahi H, Farajzadegan Z, Karimzadeh H. The association of body mass index with disease activity and clinical response to combination therapy in patients with rheumatoid arthritis. J Res Med Sci 2014; 19:509-14.
9. Daïen CI, Sellam J. Obesity and inflammatory arthritis: impact on occurrence, disease characteristics and therapeutic response. RMD Open 2015; 1:e000012. https://doi.org/10.1136/rmdopen-2014-000012
PMid:26509048 PMCid:PMC4613154
10. Baker JF, Ostergaard M, George M, et al. Greater body mass independently predicts less radiographic progression on X-ray and MRI over 1-2 years. Ann Rheum Dis 2014; 73:1923-8. https://doi.org/10.1136/annrheumdis-2014-205544
PMid:25091439 PMCid:PMC4809044
11. Iannone F, Fanizzi R, Notarnicola A, et al. Obesity reduces the drug survival of second line biological drugs following a first TNF-α inhibitor in rheumatoid arthritis patients. Joint Bone Spine 2015; 82:187-91. https://doi.org/10.1016/j.jbspin.2014.12.006
PMid:25619156
12. Kmet LM, Lee R, Cook LS. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields. Edmonton: Alberta Heritage Foundation for Medical Research, 2004.
13. Kaufmann J, Kielstein V, Kilian S, Stein G, Hein G. Relation between body mass index and radiological progression in patients with rheumatoid arthritis. J Rheumatol 2003; 30:2350-5.
14. Escalante A, Haas RW, del Rincon I. Paradoxical effect of body mass index on survival in rheumatoid arthritis: role of comorbidity and systemic inflammation. Arch Intern Med 2005; 165:1624-9. https://doi.org/10.1001/archinte.165.14.1624
PMid:16043681
15. Hashimoto J, Garnero P, van der Heijde D, et al. A combination of biochemical markers of cartilage and bone turnover, radiographic damage and body mass index to predict the progression of joint destruction in patients with rheumatoid arthritis treated with disease-modifying anti-rheumatic drugs. Mod Rheumatol 2009; 19:273-82. https://doi.org/10.3109/s10165-009-0170-4
PMid:19452245
16. van der Helm-van Mil AH, van der Kooij SM, Allaart CF, Toes RE, Huizinga TW. A high body mass index has a protective effect on the amount of joint destruction in small joints in early rheumatoid arthritis. Ann Rheum Dis 2008; 67:769-74. https://doi.org/10.1136/ard.2007.078832
PMid:17965124
17. Giles JT, Allison M, Bingham CO 3rd, Scott WM Jr, Bathon JM. Adiponectin is a mediator of the inverse association of adiposity with radiographic damage in rheumatoid arthritis. Arthritis Rheum 2009; 61:1248-56. https://doi.org/10.1002/art.24789
PMid:19714593 PMCid:PMC2759038
18. Westhoff G, Rau R, Zink A. Radiographic joint damage in early rheumatoid arthritis is highly dependent on body mass index. Arthritis Rheum 2007; 56:3575-82. https://doi.org/10.1002/art.23033
PMid:17968909
19. Jurgens MS, Jacobs JW, Geenen R, et al; Utrecht Arthritis Cohort Study Group. Increase of body mass index in a tight controlled methotrexate-based strategy with prednisone in early rheumatoid arthritis: side effect of the prednisone or better control of disease activity? Arthritis Care Res (Hoboken) 2013; 65:88-93. https://doi.org/10.1002/acr.21797
PMid:22807253
20. Munro R, Capell H. Prevalence of low body mass in rheumatoid arthritis: association with the acute phase response. Ann Rheum Dis 1997; 56:326-9. https://doi.org/10.1136/ard.56.5.326
PMid:9175935 PMCid:PMC1752373
21. Velpula UD, Agrawal S, Thomas J, et al. Low body mass index is adversely associated with radiographic joint damage in Indian patients with early rheumatoid arthritis. J Rheumatol 2011; 38:434-8. https://doi.org/10.3899/jrheum.100535
PMid:21078713
22. Gardette A, Ottaviani S, Sellam J, et al. Body mass index and response to tocilizumab in rheumatoid arthritis: a real life study. Clin Rheumatol 2016; 35:857-61. https://doi.org/10.1007/s10067-016-3183-3
PMid:26801332
23. Ottaviani S, Gardette A, Roy C, et al. Body mass index and response to rituximab in rheumatoid arthritis. Joint Bone Spine 2015; 82:432-6. https://doi.org/10.1016/j.jbspin.2015.02.011
PMid:26184536
24. Morgan SL, Anderson AM, Hood SM, et al. Nutrient intake patterns, body mass index, and vitamin levels in patients with rheumatoid arthritis. Arthritis Care Res 1997; 10:9-17. https://doi.org/10.1002/art.1790100103
PMid:9313385
25. Iannone F, Fanizzi R, Scioscia C, Anelli MG, Lapadula G. Body mass does not affect the remission of psoriatic arthritis patients on anti-TNF-α therapy. Scand J Rheumatol 2013; 42:41-4. https://doi.org/10.3109/03009742.2012.715186
PMid:22991950
26. Choe JY, Bae J, Lee H, Park SH, Kim SK. Lack association of body mass index with disease activity composites of rheumatoid arthritis in Korean population: cross-sectional observation. Clin Rheumatol 2014; 33:485-92. https://doi.org/10.1007/s10067-013-2427-8
PMid:24202616
27. Pers YM, Godfrin-Valnet M, Lambert J, et al. Response to tocilizumab in rheumatoid arthritis is not influenced by the body mass index of the patient. J Rheumatol 2015; 42:580-4. https://doi.org/10.3899/jrheum.140673
PMid:25641885
28. D'Agostino M, Alten R, Mysler E, et al. Body mass index and clinical response to intravenous or subcutaneous abatacept in patients with rheumatoid arthritis. Clin Rheumatol 2017; 36:2655-65. https://doi.org/10.1007/s10067-017-3788-1
PMid:28822046 PMCid:PMC5681604
29. George MD, Østergaard M, Conaghan PG, et al. Obesity and rates of clinical remission and low MRI inflammation in rheumatoid arthritis. Ann Rheum Dis 2017; 76:1743-6. https://doi.org/10.1136/annrheumdis-2017-211569
PMid:28606966
30. Gardette A, Ottaviani S, Sellam J, et al. Body mass index and response to abatacept in rheumatoid arthritis. Eur J Clin Invest 2016; 46:1048-52. https://doi.org/10.1111/eci.12691
PMid:27736006
31. Sandberg ME, Bengtsson C, Kallberg H, et al. Overweight decreases the chance of achieving good response and low disease activity in early rheumatoid arthritis. Ann Rheum Dis 2014; 73:2029-33. https://doi.org/10.1136/annrheumdis-2013-205094
PMid:24818635
32. Gremese E, Carletto A, Padovan M, et al; Gruppo Italiano di Studio sulle Early Arthritis (GISEA). Obesity and reduction of the response rate to anti-tumor necrosis factor α in rheumatoid arthritis: an approach to a personalized medicine. Arthritis Care Res (Hoboken) 2013; 65:94-100. https://doi.org/10.1002/acr.21768
PMid:22730143
33. Klaasen R, Wijbrandts CA, Gerlag DM, Tak PP. Body mass index and clinical response to infliximab in rheumatoid arthritis. Arthritis Rheum 2011; 63:359-64. https://doi.org/10.1002/art.30136
PMid:21279992
34. Ottaviani S, Gardette A, Tubach F, et al. Body mass index and response to infliximab in rheumatoid arthritis. Clin Exp Rheumatol 2015; 33:478-83.
35. Wolfe F, Michaud K. Effect of body mass index on mortality and clinical status in rheumatoid arthritis. Arthritis Care Res (Hoboken) 2012; 64:1471-9. https://doi.org/10.1002/acr.21627
PMid:22514152
36. Eder L, Thavaneswaran A, Chandran V, Cook RJ, Gladman DD. Obesity is associated with a lower probability of achieving sustained minimal disease activity state among patients with psoriatic arthritis. Ann Rheum Dis 2015; 74:813-7. https://doi.org/10.1136/annrheumdis-2013-204448
PMid:24431392
37. Di Minno MN, Peluso R, Iervolino S, et al; CaRRDs Study Group. Weight loss and achievement of minimal disease activity in patients with psoriatic arthritis starting treatment with tumour necrosis factor α blockers. Ann Rheum Dis 2014; 73:1157-62. https://doi.org/10.1136/annrheumdis-2012-202812
PMid:23771989 PMCid:PMC4033114
38. Di Minno MN, Peluso R, Iervolino S, et al. Obesity and the prediction of minimal disease activity: a prospective study in psoriatic arthritis. Arthritis Care Res (Hoboken) 2013; 65:141-7. https://doi.org/10.1002/acr.21711
PMid:22514189
39. Cassano N, Galluccio A, De Simone C, et al. Influence of body mass index, comorbidities and prior systemic therapies on the response of psoriasis to adalimumab: an exploratory analysis from the APHRODITE data. J Biol Regul Homeost Agents 2008; 22:233-7.
40. Gremese E, Bernardi S, Bonazza S, et al. Body weight, gender and response to TNF-α blockers in axial spondyloarthritis. Rheumatology (Oxford) 2014; 53:875-81. https://doi.org/10.1093/rheumatology/ket433
PMid:24407233
41. Katz P, Yazdany J, Julian L, et al. Impact of obesity on functioning among women with systemic lupus erythematosus. Arthritis Care Res (Hoboken) 2011; 63:1357-64. https://doi.org/10.1002/acr.20526
PMid:21702085 PMCid:PMC3183275
42. Ibn Yacoub Y, Amine B, Laatiris A, et al. Prevalence of overweight in Moroccan patients with rheumatoid arthritis and its relationships with disease features. Clin Rheumatol 2012; 31:479-82. https://doi.org/10.1007/s10067-011-1874-3
PMid:22042491
43. Moura dos Santos Fde M, Borges MC, Telles RW, Correia MI, Lanna CC. Excess weight and associated risk factors in patients with systemic lupus erythematosus. Rheumatol Int 2013; 33:681-8. https://doi.org/10.1007/s00296-012-2402-8
PMid:22527136
44. Stavropoulos-Kalinoglou A, Metsios GS, Panoulas VF, et al. Underweight and obese states both associate with worse disease activity and physical function in patients with established rheumatoid arthritis. Clin Rheumatol 2009; 28:439-44. https://doi.org/10.1007/s10067-008-1073-z
PMid:19096748
45. Garcia-Poma A, Segami MI, Mora CS, et al. Obesity is independently associated with impaired quality of life in patients with rheumatoid arthritis. Clin Rheumatol 2007; 26:1831-5. https://doi.org/10.1007/s10067-007-0583-4
PMid:17340047
46. Colmegna I, Hitchon CA, Bardales MC, Puri L, Bartlett SJ. High rates of obesity and greater associated disability among people with rheumatoid arthritis in Canada. Clin Rheumatol 2016; 35:457-60. https://doi.org/10.1007/s10067-015-3154-0
PMid:26712499
47. Uutela T, Kautiainen H, Järvenpää S, et al. Waist circumference based abdominal obesity may be helpful as a marker for unmet needs in patients with RA. Scand J Rheumatol 2014; 43:279-85. https://doi.org/10.3109/03009742.2013.858769
PMid:24467375
48. Jawaheer D, Olsen J, Lahiff M, et al; QUEST-RA. Gender, body mass index and rheumatoid arthritis disease activity: results from the QUEST-RA Study. Clin Exp Rheumatol 2010; 28:454-61.
49. Giles JT, Bartlett SJ, Andersen RE, Fontaine KR, Bathon JM. Association of body composition with disability in rheumatoid arthritis: impact of appendicular fat and lean tissue mass. Arthritis Rheum 2008; 59:1407-15. https://doi.org/10.1002/art.24109
PMid:18821641 PMCid:PMC2670990
50. Giles JT, Bartlett SJ, Andersen R, et al. Association of body fat with C-reactive protein in rheumatoid arthritis. Arthritis Rheum 2008; 58:2632-41. https://doi.org/10.1002/art.23766
PMid:18759279 PMCid:PMC2671067
51. Caplan L, Davis LA, Bright CM, et al. Body mass index and the rheumatoid arthritis swollen joint count: an observational study. Arthritis Care Res (Hoboken) 2013; 65:101-6. https://doi.org/10.1002/acr.21734
PMid:22623288 PMCid:PMC3430738
52. van Genderen S, Boonen A, van der Heijde D, et al. Accelerometer quantification of physical activity and activity patterns in patients with ankylosing spondylitis and population Controls. J Rheumatol 2015; 42:2369-75. https://doi.org/10.3899/jrheum.150015
PMid:26523021
53. Durcan L, Wilson F, Conway R, Cunnane G, O'Shea FD. Increased body mass index in ankylosing spondylitis is associated with greater burden of symptoms and poor perceptions of the benefits of exercise. J Rheumatol 2012; 39:2310-4. https://doi.org/10.3899/jrheum.120595
PMid:23070993
54. Humphreys JH, Verstappen SM, Mirjafari H, et al. Association of morbid obesity with disability in early inflammatory polyarthritis: results from the Norfolk Arthritis Register. Arthritis Care Res (Hoboken) 2013; 65:122-6. https://doi.org/10.1002/acr.21722
PMid:22556112 PMCid:PMC3568899
55. Heimans L, van den Broek M, le Cessie S, et al. Association of high body mass index with decreased treatment response to combination therapy in recent-onset rheumatoid arthritis patients. Arthritis Care Res (Hoboken) 2013; 65:1235-42. https://doi.org/10.1002/acr.21978
PMid:23408767
56. Kearsley-Fleet L, Davies R, De Cock D, et al; BSRBR-RA Contributors Group. Biologic refractory disease in rheumatoid arthritis: results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Ann Rheum Dis 2018; 77:1405-12. https://doi.org/10.1136/annrheumdis-2018-213378
PMid:29980575 PMCid:PMC6161665
57. Patterson SL, Schmajuk G, Jafri K, Yazdany J, Katz P. Obesity is independently associated with worse patient-reported outcomes in women with systemic lupus erythematosus. Arthritis Care Res (Hoboken) 2019; 71:126-33. https://doi.org/10.1002/acr.23576
PMid:29740985
58. Kreps DJ, Halperin F, Desai SP, et al. Association of weight loss with improved disease activity in patients with rheumatoid arthritis: a retrospective analysis using electronic medical record data. Int J Clin Rheumtol 2018; 13:1-10. https://doi.org/10.4172/1758-4272.1000154
PMid:29606976 PMCid:PMC5875117
59. Mahieu MA, Ahn GE, Chmiel JS, et al. Serum adipokine levels and associations with patient-reported fatigue in systemic lupus erythematosus. Rheumatol Int 2018; 38:1053-61. https://doi.org/10.1007/s00296-017-3924-x
PMid:29302804 PMCid:PMC5955723
60. Schulman E, Bartlett SJ, Schieir O, et al; CATCH Investigators. Overweight, obesity, and the likelihood of achieving sustained remission in early rheumatoid arthritis: results from a multicenter prospective cohort study. Arthritis Care Res (Hoboken) 2018; 70:1185-91. https://doi.org/10.1002/acr.23457
PMid:29193840
61. Levitsky A, Brismar K, Hafström I, et al. Obesity is a strong predictor of worse clinical outcomes and treatment responses in early rheumatoid arthritis: results from the SWEFOT trial. RMD Open 2017; 3:e000458. https://doi.org/10.1136/rmdopen-2017-000458
PMid:28879052 PMCid:PMC5574420
62. Micheroli R, Hebeisen M, Wildi LM, et al; Rheumatologists of the Swiss Clinical Quality Management Program. Impact of obesity on the response to tumor necrosis factor inhibitors in axial spondyloarthritis. Arthritis Res Ther 2017; 19:164. https://doi.org/10.1186/s13075-017-1372-3
PMid:28724442 PMCid:PMC5518107
63. Lee YX, Kwan YH, Png WY, et al. Association of obesity with patient-reported outcomes in patients with axial spondyloarthritis: a cross-sectional study in an urban Asian population. Clin Rheumatol 2017; 36:2365-70. https://doi.org/10.1007/s10067-017-3585-x
PMid:28378098
64. Rosas J, Llinares-Tello F, Senabre-Gallego JM, et al; and the AIRE-MB Group. Obesity decreases clinical efficacy and levels of adalimumab in patients with ankylosing spondylitis. Clin Exp Rheumatol 2017; 35:145-8.
65. Højgaard P, Glintborg B, Kristensen LE, et al. The influence of obesity on response to tumour necrosis factor-α inhibitors in psoriatic arthritis: results from the DANBIO and ICEBIO registries. Rheumatology (Oxford) 2016; 55:2191-9. https://doi.org/10.1093/rheumatology/kew326
PMid:27651526
66. Ma X, Xu S. TNF inhibitor therapy for rheumatoid arthritis. Biomed Rep 2013; 1:177-84. https://doi.org/10.3892/br.2012.42
PMid:24648915 PMCid:PMC3956207
67. Cohen MD, Keystone E. Rituximab for rheumatoid arthritis. Rheumatol Ther 2015; 2:99-111. https://doi.org/10.1007/s40744-015-0016-9
PMid:27747531 PMCid:PMC4883263
69. Shan J, Zhang J. Impact of obesity on the efficacy of different biologic agents in inflammatory diseases: a systematic review and meta-analysis. Joint Bone Spine 2019; 86:173-83. https://doi.org/10.1016/j.jbspin.2018.03.007
PMid:29635017
71. Singh S, Facciorusso A, Singh AG, et al. Obesity and response to anti-tumor necrosis factor-α agents in patients with select immune-mediated inflammatory diseases: a systematic review and meta-analysis. PLoS One 2018; 13:e0195123. https://doi.org/10.1371/journal.pone.0195123
PMid:29771924 PMCid:PMC5957395
72. Murad MH, Asi N, Alsawas M, Alahdab F. New evidence pyramid. Evid Based Med 2016; 21:125-7. https://doi.org/10.1136/ebmed-2016-110401
PMid:27339128 PMCid:PMC4975798