Singapore Med J 2019; 60(8): 387-396 doi: https://doi.org/10.11622/smedj.2019088
Ten-year narrative review on antimicrobial resistance in Singapore
Alvin Qijia Chua1,2, BSc, MSc, Andrea Lay-Hoon Kwa1,3, PharmD, Thean Yen Tan3,4, MBBCh, MRCPath, Helena Legido-Quigley2, PhD, MSc, Li Yang Hsu2,5, MBBS, MPH
Author Information >Copyright and License information >
1Department of Pharmacy, Singapore General Hospital, Singapore 2Saw Swee Hock School of Public Health, National University of Singapore, Singapore 3Duke-NUS Medical School, National University of Singapore, Singapore 4Department of Laboratory Medicine, Changi General Hospital, Singapore 5National Centre for Infectious Diseases, Singapore Correspondence: A/Prof Li Yang Hsu, Head, Infectious Diseases Programme, Saw Swee Hock School of Public Health, National University of Singapore, 12 Science Drive 2, Singapore 117549. mdchly@nus.edu.sg
Antimicrobial resistance (AMR) results in drug-resistant infections that are harder to treat, subsequently leading to increased morbidity and mortality. In 2008, we reviewed the problem of AMR in Singapore, limiting our discussion to the human healthcare sector. Ten years later, we revisit this issue again, reviewing current efforts to contain it in order to understand the progress made as well as current and emerging challenges. Although a significant amount of work has been done to control AMR and improve antibiotic prescribing in Singapore, most of it has focused on the hospital setting, with mixed impact. The role of antibiotic use and AMR in food animals and the environment – and the link to human health – is better understood today. This issue of AMR encompasses both human health as well as animal/food safety, and efforts to control it will need to continually evolve to maintain or improve on current gains.
Keywords: anti-bacterial agents/therapeutic use, antimicrobial stewardship, bacterial drug resistance, public health, Singapore
INTRODUCTION
Antimicrobial resistance (AMR), which results in drug-resistant infections that are harder to treat and attendant increased morbidity and mortality, is a slow but implacable evolutionary process that has been sped up by human activity in multiple sectors, particularly human health and agriculture.(1-4) In 2008, when the issue was less well known, we wrote a position paper on the problem of AMR in Singapore, limiting our discussion to the human healthcare sector.(5)
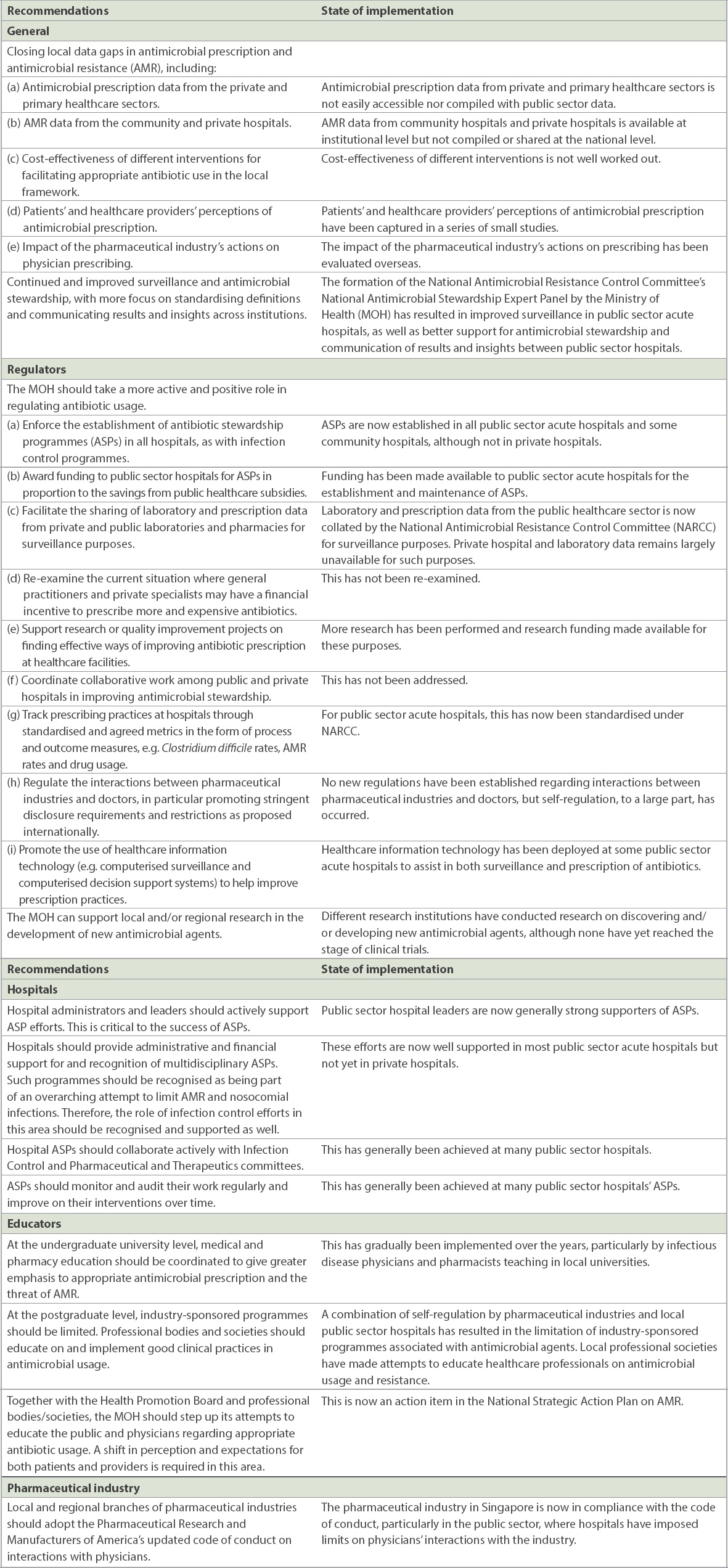
Several recommendations, as summarised in Table I, were made based on evidence and expert opinion available a decade ago that would facilitate the prudent and appropriate use of antibiotics.(5) These included hospital- and ministry-level policies and interventions that resulted in enhanced surveillance, formal antimicrobial stewardship programmes (ASPs) in hospitals, and education on AMR.(5) As seen in Table I, we observed that the majority of the recommendations made in 2008(5) have been implemented over the past decade in local public sector hospitals, but not in private hospitals or the primary healthcare sector. All acute care public sector hospitals now have ASPs – primarily funded by the Ministry of Health (MOH) – and formal laboratory surveillance of key antibiotic-resistant bacteria isolated from patients attending public sector hospitals. Teaching of AMR to healthcare professionals and undergraduates is also increasingly emphasised.
Table I
Recommendations made in 2008 to reduce inappropriate antimicrobial usage and an assessment of their implementation over the past decade.
Understanding of AMR has broadened, particularly with regard to the role of agriculture and the environment.(1-4) After ten years, it is timely that the issue of AMR and efforts to contain it in Singapore be reviewed again, in order to understand the progress made and the challenges that remain or have emerged over time.
AWARENESS AND POLICY-SETTING GOALS
Unlike a decade ago, AMR is widely recognised as a global public health threat today.(1-4) The threat of a post-antibiotic era ‘doomsday scenario’, where common infections or minor injuries can result in death, has been raised by the World Health Organization (WHO).(1) The United Kingdom’s Review on AMR estimated that by 2050, the continued rise in AMR could result in ten million deaths annually and an economic loss of USD 100 trillion.(2) This is corroborated by a separate World Bank report conducted in 2016, which estimated that the impact of AMR would mirror that of the 2008 global financial crisis by 2050.(6)
In response, the World Health Assembly adopted a Global Action Plan for AMR in 2015, calling on each member state to develop and implement a corresponding context-specific multisectoral national plan.(3) In the following year, at a special high-level meeting of the United Nations General Assembly, all member states pledged to dedicate themselves to a global response against this rising threat, adopting a ‘One Health’ approach.(4)
In line with this goal, Singapore launched its own National Strategic Action Plan on AMR in November 2017.(7) The multisectoral plan, which was jointly developed by the MOH, the former Agri-Food and Veterinary Authority of Singapore (AVA), the National Environment Agency (NEA), and the national water agency PUB, sets a national ‘One Health’ framework to reduce the emergence and spread of drug-resistant micro-organisms through five core strategies: (a) surveillance and risk assessment, to enable timely and appropriate responses to be mounted; (b) research, to better understand AMR and provide information – where gaps in evidence exist – to support the other core strategies; (c) education, to increase awareness and understanding of AMR; (d) prevention and control of infection, to stop transmission of resistant organisms in healthcare settings and the community; and (e) optimisation of antimicrobial use, to slow the emergence of resistance and minimise healthcare costs.
In July 2018, the WHO released a report on action against AMR at the country level.(8) The report was based on submissions of a country self-assessment questionnaire, summarising national progress on the strategic objectives in the Global Action Plan.(3,9) The topics assessed included human health, animal production, food safety concerns, plant production and the environment. A total of 154 countries were included in the report, showing much international effort to tackle AMR. Singapore was reported to have achieved most of the strategic objectives, especially for human health.(10) Some gaps were identified, including better antibiotic stewardship, surveillance, education and awareness, and research on areas involving animal and plant health, as well as the environment.(10)
CHANGES IN ANTIMICROBIAL RESISTANCE EPIDEMIOLOGY OVER A DECADE
Global perspective
The first global surveillance report published by the WHO in 2014 showed high rates of AMR in almost all WHO regions, although updated data is not available from several countries. Asia had the highest rates of third-generation cephalosporin-resistant Enterobacteriaceae.(1) The vast majority of third-generation cephalosporin resistance in Enterobacteriaceae is due to the production of extended-spectrum beta-lactamases (ESBLs) and, to a lesser extent, AmpC beta-lactamases.(11) This is not just a problem within hospitals, as the incidence of ESBL infections is also increasing rapidly in the community setting, with ESBL-producing Enterobacteriaceae faecal colonisation rates among healthy individuals reported at 14% or higher worldwide.(12,13)
The widespread use of carbapenems, largely directed against possible and proven ESBL-producing Enterobacteriaceae infections, likely promoted the selection and subsequent dissemination of multiple different mechanisms of carbapenem resistance among Enterobacteriaceae.(14) In South and Southeast Asia, carbapenem-resistant Enterobacteriaceae (CRE) has been reported in virtually every country, possibly exceeding 10% of all hospital-cultured Enterobacteriaceae in South Asian countries.(15) More recently, transmissible resistance to colistin, one of the few available drugs for treating carbapenem-resistant Gram-negative infections, has also surfaced. Plasmid-mediated mcr (mobilised colistin resistance) genes were first described in Escherichia coli (E. coli) isolated from food animals in China in 2015. They were subsequently found in clinical isolates in various parts of the world, including Singapore.(16,17)
Methicillin-resistant Staphylococcus aureus (S. aureus) (MRSA) was initially considered a purely nosocomial pathogen. This changed significantly with the emergence and establishment of community-associated MRSA (CA-MRSA).(18) Moreover, recent reports suggest that CA-MRSA is taking over healthcare-associated MRSA as a cause of endemic healthcare-acquired infections at many hospitals around the world.(19)
Other than in humans, these drug-resistant organisms have also been found in animals and the environment. ESBL-producing Enterobacteriaceae have been reported in livestock and wildlife.(20,21) Reports of livestock-associated MRSA, which are genetically distinct from human isolates, have steadily increased.(18) This is probably due to the overcrowded conditions of food animals in most commercial farms, along with extensive use of antibiotics as growth promoters, prophylaxis or metaphylaxis.(22) The problem is exacerbated by the complicated exchange of antibiotic resistance genes between human, livestock and environmental pools, either via direct contact or through the food chain by contact with or ingestion of animal food products.(21)
Local perspective
Multidrug-resistant organisms have also been reported in Singapore. The diversity in the epidemiology of these drug-resistant organisms is likely the consequence of Singapore’s strategic geographical location at international crossroads.
ESBL and AmpC beta-lactamase-producing Enterobacteriaceae were first documented in 1986 and 2003, respectively, in Singapore.(23,24) In 2006, 30.3% and 19.6% of hospital isolates of Klebsiella spp. and E. coli, respectively, were ESBL producers, with 5.6% and 8.5% of each type of bacteria also producing AmpC.(25) These rates have remained relatively stable over the past decade in local hospitals. However, two dissimilar surveys in 2006 by Young et al and 2016 (Alex Cook et al, personal communication) showed a marked difference in community rectal carriage of ESBL-producing Enterobacteriaceae (6.3% in 2006 vs. 26.0% in 2016), which appears to signify an increasing trend despite the differing methodology of the studies.(26)
Of greater concern is the growing threat of CRE. Rare in 2008, CRE was at that time due almost entirely to a combination of ESBL or AmpC beta-lactamases production combined with drug impermeability due to porin loss.(24) The introduction of carbapenemase-producing Enterobacteriaceae (CP-CRE) – with diverse plasmid-borne enzymes such as NDM, KPC and OXA-48-like variants – into local hospitals in rapid succession since 2010 has changed the local dynamic drastically.(27,28) In a study conducted in Singapore General Hospital, the largest hospital in Singapore, carbapenem resistance rates among Klebsiellapneumoniae and E. coli increased from 2% and 0% to 12% and 5%, respectively, between 2011 and 2015.(29) From 2010 to 2013, NDM was the most frequently detected gene (57.3%), followed by OXA-48-like (24.2%) and KPC (13.7%) genes,(30) although the situation can change rapidly. Fortunately, CP-CRE rates appear to have stabilised in the past two years.(31) Antibiotic resistance in non-fermenting Gram-negative bacteria is also of concern. From 2011 to 2015, the prevalence of carbapenem-resistant Acinetobacter baumannii and Pseudomonas aeruginosa has remained stable at approximately 50% and 10%, respectively.(29)
MRSA emerged in Singapore in the 1970s,(32) becoming endemic in local healthcare facilities, with 35.3% of all S. aureus isolates reported to be methicillin-resistant in 2006.(33) Apart from acute care hospitals, intermediate-term and long-term care facilities are also important reservoirs for MRSA. In 2014, the prevalence of MRSA was found to be significantly higher in intermediate (29.9%) and long-term (20.4%) care facilities than in acute care hospitals (11.8%), as reported in a recent study.(34) The organism has also been sporadically reported in the community as well as in local food and animals.(35-37) The MOH, working with public sector hospitals, has stepped up measures to track and control the rates of MRSA, which have since fallen considerably from over a decade ago.(38) However, MRSA rates in private sector hospitals are not publicly available.
Vancomycin-resistant Enterococcus (VRE) was first reported in Singapore in 1994 but remained rare until two significant outbreaks in 2004 and 2005.(39) A passive laboratory surveillance programme from 2006 to 2010 concluded that 0.4%–0.7% of all clinical enterococcal isolates were resistant to vancomycin over these five years, with the overall incidence density of VRE remaining stable over time.(40) Unfortunately, resistance to the few antibiotics with activity against VRE has started to emerge, and VRE carriage rates appear to have increased since 2010.(41,42)
LOCAL SURVEILLANCE
In the human healthcare sector, the Network for Antimicrobial Resistance Surveillance (Singapore) – an informal collaboration between public sector clinical microbiologists, pharmacists and infectious diseases physicians that was established in 2005 – was the first local multi-hospital group to elucidate the scale of antibiotic drug resistance and prescription in the local setting.(33) Participation in this programme was voluntary, resulting in gaps in the data collected. The network published reports until 2011, several of which took the form of academic publications.(43-45)
In 2009, the MOH formally established the National Antimicrobial Taskforce (NAT) – consisting of infectious disease physicians, microbiologists, infection control physicians, nurses and pharmacists – to formulate and implement measures to monitor the use of antibiotics as well as AMR rates. The NAT was also tasked with recommending measures to prevent and limit the incidence of such infections. The NAT has published annual reports on public sector hospital AMR and antibiotic prescribing rates since 2012, but these are not publicly available. In 2014, the NAT was reorganised into the National Antimicrobial Resistance Control Committee (NARCC), for surveillance of AMR and antibiotic prescribing, and the National Infection Prevention and Control Committee, for providing national guidelines on infection prevention in the healthcare setting.
Surveillance on AMR and antimicrobial prescribing has been patchy in the animal and food sectors in Singapore. Academic projects implemented prior to 2018 were primarily independent and one-off.(35,46,47) With the announcement of the National Strategic Action Plan against AMR, however, representatives of the MOH, AVA, NEA and PUB have made an effort to initiate AMR surveillance in the animal, food and environmental sectors, and this information will be incorporated into a joint ‘One Health’ report along with the NARCC annual reports in the near future.
LOCAL RESEARCH
Research is critical to fill in evidence gaps in AMR by generating new knowledge. This includes identifying risk factors for the emergence and spread of resistant organisms, and ways to stop their progress. This information will support relevant policymakers and organisations in making decisions on the appropriate actions necessary to combat AMR. There has been an increase in research activities and collaboration between various research groups in recent years, largely supported by the public sector in Singapore.
The National Research Foundation is currently funding a SGD 30-million research project in AMR over five years.(48) This project, helmed by the Singapore-MIT Alliance for Research and Technology, is being conducted by an interdisciplinary research group (IRG) in partnerships with universities and research institutions in Singapore.(49) The IRG seeks to identify new mechanisms of AMR to develop new drugs and drug delivery technologies, and to exploit host immunity to kill resistant microbes. It is also interested in developing new therapeutic diagnostic methods that are fast, cheap and easy to administer.
On a smaller scale, the National Medical Research Council (NMRC) is currently funding an SGD 5-million four-year collaborative grant on AMR.(50) The grant programme, Collaborative Solutions Targeting Antimicrobial Resistance Threats in the Health System (CoSTAR-HS), is a collaboration between three major hospitals in Singapore. CoSTAR-HS focuses on health systems and is looking to develop new diagnostic methods for identification of resistance mechanisms in microbes, new assessments for infection control strategies, optimisation of ASPs, and research into health systems and behavioural drivers of AMR. In addition to the above, multiple individual research grants have been given out by the NMRC, MOH and Agency for Science, Technology and Research for a variety of independent research efforts into AMR over the past decade.
Other than research on human health, it is also important to focus on animals, food and the environment. Although there is ongoing research in these sectors, much more work is needed to develop new vaccines, drugs, animal management systems and husbandry practices.(46,51) In addition, there is a need to understand how antibiotics may contribute to the selection and spread of drug-resistant organisms in the natural environment. This information is necessary to better control the transmission of drug-resistant organisms between the human, animal, food and environment sectors.
One critical piece that is missing in Singapore is an estimate of the socioeconomic impact of AMR at the local level. While a number of macro- and microeconomic studies have been published,(2,6,52) these do not include the unique features of our healthcare system nor our reliance on food importation; a more accurate local assessment would enable better financing estimates for the control of AMR in Singapore.
EDUCATION ON ANTIMICROBIAL RESISTANCE AND ANTIBIOTIC PRESCRIBING
As misconceptions about appropriate antibiotic use and the consequences of misusing antibiotics are common,(53) education is needed to guide people towards a correct, unified understanding and perception of AMR, including its impact on society. Education serves two main purposes: (a) to let the target audience recognise that AMR is an urgent issue that needs to be acted upon; and (b) to equip them with the right knowledge to effectively participate in activities against AMR.
Education for healthcare and veterinary professionals should include appropriate antibiotic usage, contributors to AMR and infection control issues. These are currently included in the education curricula of many undergraduate and graduate healthcare professional programmes. Ongoing continuing education keeps professionals up to date as new evidence on AMR emerges. Training workshops can also be conducted. For example, in the area of antimicrobial stewardship, the annual Singapore Antimicrobial Stewardship Training introduces local and regional participants to best practices and skills that are needed to establish ASPs.(54)
In addition to knowledge and skills, promoting behavioural changes in practice is also important and should be guided by sociobehavioural understanding of the target audience. A local focus group study was conducted to explore hospital physicians’ perceptions of and attitudes toward their ASP.(55) Two reasons identified for poor acceptance of ASP recommendations were lack of awareness of the ASP team and lack of trust in them. These could potentially be addressed through improved communication with the various hospital departments via educational roadshows, regular reports on their antibiotic prescription trends, and published evidence that ASP recommendations specific to their department are advantageous to their patients.(56-60)
Patients’ attitudes and expectations often influence physicians’ antibiotic prescribing practices,(53) reinforcing the need for public education to increase awareness about the issue of AMR and appropriate antibiotic use. Since 2016, Singapore has been actively participating in the annual World Antibiotic Awareness Week, supported by the WHO every November, by reaching out to the public at various public forums, hospitals and national libraries.(61,62) In 2017, the MOH and Health Promotion Board organised a social campaign called F.I.G.H.T., focusing on the general prevention of infection to fight the spread of influenza and other infectious diseases.(63) Most recently, the issue of antibiotics overprescription was featured in the local newspapers.(64,65) The articles highlighted the results of a recent national point prevalence study (PPS) stating that more than half the patients in acute hospitals were on at least one antibiotic, a much higher proportion compared to inpatients in European hospitals.(66)
Emphasis should also be placed on education in the agriculture and biopharmaceutical sectors, although these are small in Singapore. End-users of veterinary medicines such as farmers should know how to responsibly use antibiotics in farm animals. Pharmaceutical industries, farms and hospitals involved in the disposal of waste should be educated on proper waste management to reduce the discharge of antibiotics into the environment, reinforced by local regulatory controls.
PREVENTION AND CONTROL OF INFECTION IN SINGAPORE
Effective infection prevention and control (IPC) measures are required to minimise infection risks and limit the emergence and spread of drug-resistant organisms among humans and animals, which ultimately reduces the usage of antibiotics. Vaccination is occasionally overlooked as an intervention against AMR. However, the prevention of viral or bacterial infections that could lead to healthcare visits correspondingly reduces opportunities for antibiotic prescription. In 2017, MOH established the National Adult Immunisation Schedule to facilitate the uptake of important vaccinations such as influenza and pneumococcal vaccines among adults.(67) These recommendations are not mandatory, and measures to monitor and encourage vaccine uptake are necessary.
IPC programmes are mandated for all hospitals as part of hospital licensing. National guidelines for IPCs have recently been published by the National Infection Prevention and Control Committee and help to establish standards and guidance to prevent the spread of infections, including from multidrug-resistant organisms.(68) Hospitals must report infection control indicators routinely to the MOH for detection of any peculiar trends.
In the animal sector, the Singapore Food Agency (SFA) enforces strict biosecurity requirements and good animal husbandry/aquaculture practices to reduce the occurrence of infectious diseases in animals, although testing for multidrug-resistant organisms in food is not routinely performed.
OPTIMISATION OF ANTIMICROBIAL PRESCRIPTION AND USE
Community and veterinary prescription of antibiotics
There remains a gap in knowledge about the amount and appropriateness of antibiotic prescribing in the primary healthcare setting in Singapore, although it is likely that improvements can be made.(53) A similar gap exists for antibiotics prescribed in local veterinary and agricultural practices. In these settings, in addition to attempts to improve data capture, strategies to improve prescribing practices in the community – such as guidelines for antibiotic prescription and incentives to encourage proper antibiotic usage – should be developed to tackle the issue of inappropriate prescribing. The use of antibiotics in veterinary medicine could be governed by regulations, while guidelines would encourage the prudent use of antibiotics in livestock and veterinary medicine.
Hospital antibiotic prescription
Data from the acute care hospitals suggests that antibiotic usage is high: in a national PPS conducted in 2015, 51% of 5,415 patients from 13 private and public acute hospitals were on at least one systemic antibiotic.(66) This was significantly higher than comparable results from a global PPS that reported 37.2% and 39% in other Asian and European settings, respectively.(69) The national study also found that 12.8% of the prescriptions were for surgical prophylaxis, the majority of which were prescribed for more than one day, a practice that is non-evidence-based.(66) Unfortunately, appropriateness of antibiotic prescriptions was not assessed as it was beyond the scope of this national PPS, although public hospitals – such as KK Women’s and Children’s Hospital – have reported that broad-spectrum antibiotics such as carbapenems were appropriately prescribed up to 90% of the time.(70)
Antimicrobial stewardship programmes in Singapore
ASPs aim to optimise antibiotic use through multi-pronged strategies, including pre-authorisation, prospective audit with intervention and feedback, and, more recently, the use of computerised clinical decision support systems (CDSSs) to improve antibiotic prescribing at the time of prescribing.(71) In 2011, MOH provided SGD 20 million to fund the development of ASPs in Singapore’s public acute care hospitals. This fund was used for the provision of ASP teams – consisting of infectious diseases physicians, microbiologists, infectious diseases pharmacists and executives – as well as the development of CDSSs. Guidelines for training and practice of antimicrobial stewardship were introduced the year after in order to ensure a consistent standard of delivery.(72)
Since then, numerous studies from various institutions have reported that ASPs were able to improve the appropriateness of antibiotic prescriptions and reduce the duration of antibiotic use without compromising patient safety.(56-60) Acceptance of ASP recommendations was associated with shorter lengths of stay, decreases in mortality and re-admissions, and substantial cost savings for patients, although ASPs on their own were notably unsuccessful in significantly decreasing the incidence of AMR in local hospitals.(73-75)
The first local CDSS, ARUS-C (Antibiotic Resistance Utilisation and Surveillance-Control), was developed by Tan Tock Seng Hospital in 2009, prior to MOH’s ASP funding – which spurred attempts to adopt ARUS-C or develop new CDSSs after 2011.(76) By using appropriate algorithms, CDSSs could potentially provide patient-specific, evidence-based antibiotic recommendations at the point of prescribing, an advantage that is potentially magnified by the availability of other patient data within electronic medical records such as drug allergies, culture results, and renal and/or liver function.
Unfortunately, the CDSSs set up in Singapore had limited success in improving antibiotic prescribing: only 63%–67% of the antibiotic recommendations from the various CDSSs were accepted.(55,77) Another attempt to adopt ARUS-C at another local hospital failed entirely, with the hospital’s senior management pulling the plug after a short trial period. Understanding physician behaviour when using CDSS, integrating CDSS into the work process in a user-friendly manner and education on its proper usage are important to optimise uptake and acceptance.
Since 2011, ASPs have been implemented in all public acute care hospitals in Singapore. They have not been established in private hospitals and are present in only a couple of community hospitals.
Future steps to optimise prescription in hospitals
ASPs should ideally be established in both public and private hospitals, which might require a regulatory approach similar to that used for infection prevention programmes in Singapore. One possibility for established ASPs is to shift from antibiotic-specific audits to syndrome-specific audits. This is an effective way to improve prescribing, as the intervention message can be focused, with clinical guidelines and algorithms reinforced.(71) Syndrome-specific audits could then be regularly evaluated to identify new areas for targeted interventions based on local needs.(71)
The recently established National Collaborative Prescribing Programme trains experienced pharmacists and advanced practice nurses to legally prescribe medicines and order tests, without requiring a doctor’s countersignature.(78) This could possibly change the landscape of ASPs, with ASP pharmacists taking on a more active role to ensure appropriate antibiotic prescriptions or to order further investigations for the team.
New technology can be harnessed to improve patient care and the use of antibiotics. A National Electronic Health Records (NEHR) system, set up in 2011, has been collating patient health records across different healthcare providers.(79) The NEHR allows healthcare professionals to have a holistic and longitudinal view of patients’ healthcare histories. As the number of institutions participating in the NEHR increases, including general practitioner clinics, we can expect more seamless care for patients, as all previous laboratory and radiological investigations as well as prior antibiotic usage would be readily available. This enormous amount of data could potentially be harnessed for machine learning and artificial intelligence to identify potentially inappropriate prescriptions as well as improve prescribing via the development of superior versions of current-day CDSSs.(80,81)
CONCLUSION
AMR has gained considerable recognition as a major global public health threat. The position paper published in this journal a decade ago was limited in scope, focusing on human health and antibiotic prescribing in particular. A more nuanced understanding of AMR as a ‘One Health’ issue has emerged since then, and considerable work has gone into controlling AMR and improving antibiotic prescribing in Singapore, although this has been largely focused in the public hospital setting. The actual impact on the control of AMR has been mixed, with better control of MRSA coupled with a global rise in Gram-negative resistance that has also affected local hospitals and the community.
More efforts for AMR control are required in the human health, animal and environment sectors. These gaps are recognised in Singapore’s National Strategic Action Plan against AMR, which has also led to the formation of a new entity – the AMR Coordinating Office based at the National Centre for Infectious Diseases – to track and coordinate national efforts.
Other potential future steps towards the control of AMR in Singapore include expanding surveillance and educational efforts directed towards the private healthcare sector, the community and the agricultural/veterinary sectors; improving vaccination rates and other aspects of IPC in hospitals and community; continued research funding, particularly for estimating the socioeconomic impact of AMR at the local level; improving the delivery of ASPs; and harnessing new technology, including artificial intelligence, to improve antibiotic prescribing.
Because AMR is an evolutionary process, the implementation of policies to control AMR as a ‘One Health’ effort similarly needs to continually evolve in order to maintain or improve on current gains. This will require persistently strong political will and a motivated workforce in Singapore.
References World Health OrganizationAntimicrobial resistance:global report on surveillance. 2014;. Available at: https://apps.who.int/iris/bitstream/handle/10665/112642/9789241564748_eng.pdf?sequence=1. Accessed September 16, 2018. O'Neill J.Tackling drug-resistant infections globally:final report and recommendations.The review on antimicrobial resistance. 2016;May. Available at: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf. Accessed September 16, 2018. World Health OrganizationGlobal action plan on antimicrobial resistance. 2015;. Available at: http://www.wpro.who.int/entity/drug_resistance/resources/global_action_plan_eng.pdf.. Accessed September 16, 2018. United Nations General AssemblyPolitical declaration of the high-level meeting of the General Assembly on antimicrobial resistance. 2016;. Available at: https://digitallibrary.un.org/record/842813/files/A_71_L-2-EN.pdf. Accessed September 16, 2018. Hsu LY, Kwa AL, Lye DC, et al. Reducing antimicrobial resistance through appropriate antibiotic usage in Singapore.Singapore Med J. 2008;49:749-55. World Bank GroupDrug-resistant infections:a threat to our economic future (final report). 2017;March. Available at: http://documents.worldbank.org/curated/en/323311493396993758/pdf/114679-REVISED-v2-Drug-Resistant-Infections-Final-Report.pdf.. Accessed September 16, 2018. Agri-Food &Veterinary Authority of Singapore, Ministry of Health, National Environment Agency, National Water AgencyThe national strategic action plan on antimicrobial resistance, Singapore. 2017;. Available at: https://www.moh.gov.sg/docs/librariesprovider5/resources-statistics/reports/sg-national-strategic-action-plan-on-amr.pdf. Accessed September 16, 2018. World Health OrganizationCountries step up to tackle antimicrobial resistance. Available at: https://www.who.int/news-room/detail/18-07-2018-countries-step-up-to-tackle-antimicrobial-resistance. Accessed September 16, 2018. World Health OrganizationGlobal monitoring of country progress on antimicrobial resistance (AMR):Country self-assessment questionnaire (version two). Available at: https://amrcountryprogress.org/download/AMR-self-assessment-country-questionnaire-2017-English.pdf. Accessed September 16, 2018. World Health OrganizationGlobal database for antimicrobial resistance country self assessment. Available at: https://amrcountryprogress.org. Accessed September 16, 2018. Vasoo S, Barreto JN, Tosh PK.Emerging issues in gram-negative bacterial resistance:an update for the practicing clinician.Mayo Clin Proc. 2015;90:395-403. McDanel J, Schweizer M, Crabb V, et al. Incidence of extended-spectrum b-lactamase (ESBL)-producing Escherichia coli and Klebsiella infections in the United States:a systematic literature review.Infect Control Hosp Epidemiol. 2017;38:1209-15. Karanika S, Karantanos T, Arvanitis M, Grigoras C, Mylonakis E.Fecal colonization with extended-spectrum beta-lactamase-producing Enterobacteriaceae and risk factors among healthy individuals:a systematic review and metaanalysis.Clin Infect Dis. 2016;63:310-8. Hawkey PM.Multidrug-resistant Gram-negative bacteria:a product of globalization.J Hosp Infect. 2015;89:241-7. Hsu LY, Apisarnthanarak A, Khan E, et al. Carbapenem-resistant Acinetobacter baumannii and Enterobacteriaceae in South and Southeast Asia.Clin Microbiol Rev. 2017;30:1-22. Liu YY, Wang Y, Walsh TR, et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China:a microbiological and molecular biological study.Lancet Infect Dis. 2016;16:161-8. Wang R, van Dorp L, Shaw LP, et al. The global distribution and spread of the mobilized colistin resistance gene MCR-1.Nat Commun. 2018;9:1179. Lakhundi S, Zhang K.Methicillin-resistant Staphylococcus aureus:molecular characterization, evolution, and epidemiology.Clin Microbiol Rev. 2018;31:e00020-18. Otter JA, French GL.Nosocomial transmission of community-associated methicillin-resistant Staphylococcus aureus:an emerging threat.Lancet Infect Dis. 2006;6:753-5. Okpara EO, Ojo OE, Awoyomi OJ, et al. Antimicrobial usage and presence of extended-spectrum b-lactamase-producing Enterobacteriaceae in animal-rearing households of selected rural and peri-urban communities.Vet Microbiol. 2018;218:31-9. Dolejska M, Papagiannitsis CC.Plasmid-mediated resistance is going wild.Plasmid. 2018;99:99-111. Graveland H, Duim B, van Duijkeren E, Heederik D, Wagenaar JA.Livestock-associated methicillin-resistant Staphylococcus aureus in animals and humans.Int J Med Microbiol. 2011;301:630-4. Inglis TJ, Kumarasinghe G, Chow C, Liew HY.Multiple antibiotic resistance in Klebsiella spp. and other Enterobacteriaceae isolated in Singapore.Singapore Med J. 1994;35:602-4. Koh TH.Gram-negative resistance in Singapore:a historical perspective.Ann Acad Med Singapore. 2008;37:847-54. Tan TY, Hsu LY, Koh TH, et al. Antibiotic resistance in gram-negative bacilli:a Singapore perspective.Ann Acad Med Singapore. 2008;37:819-25. Young BE, Lye DC, Krishnan P, Chan SP, Leo YS.A prospective observational study of the prevalence and risk factors for colonization by antibiotic resistant bacteria in patients at admission to hospital in Singapore.BMC Infect Dis. 2014;14:298. Teo J, Ngan G, Balm M, et al. Molecular characterization of NDM-1 producing Enterobacteriaceae isolates in Singapore hospitals.Western Pac Surveill Response J. 2012;3:19-24. Balm MN, Ngan G, Jureen R, Lin RT, Teo JW.OXA-181-producing Klebsiella pneumoniae establishing in Singapore.BMC Infect Dis. 2013;13:58. Teo JQ, Cai Y, Lim TP, Tan TT, Kwa AL.Carbapenem resistance in Gram-negative bacteria:the not-so-little problem in the little red dot.Microorganisms. 2016;4:E13. Teo JW, Tan P, La MV, et al. Surveillance trends of carbapenem-resistant Enterobacteriaceae from Singapore, 2010-2013.J Glob Antimicrob Resist. 2014;2:99-102. Marimuthu K, Venkatachalam I, Khong WX, et al. Carbapenemase-Producing Enterobacteriaceae in Singapore (CaPES) Study GroupClinical and molecular epidemiology of carbapenem-resistant Enterobacteriaceae among adult inpatients in Singapore.Clin Infect Dis. 2017;64:suppl_2S68-S75. Esuvaranathan K, Kuan YF, Kumarasinghe G, Bassett DC, Rauff A.A study of 245 infected surgical wounds in Singapore.J Hosp Infect. 1992;21:231-40. Hsu LY, Tan TY, Jureen R, et al. Antimicrobial drug resistance in Singapore hospitals.Emerg Infect Dis. 2007;13:1944-7. Chow A, Lim VW, Khan A, et al. MRSA transmission dynamics among interconnected acute, intermediate-term, and long-term healthcare facilities in Singapore.Clin Infect Dis. 2017;64:suppl_2S76-S81. Aung KT, Hsu LY, Koh TH, et al. Prevalence of methicillin-resistant Staphylococcus aureus (MRSA) in retail food in Singapore.Antimicrob Resist Infect Control. 2017;6:94. Hsu LY, Koh YL, Chlebicka NL, et al. Establishment of ST30 as the predominant clonal type among community-associated methicillin-resistant Staphylococcus aureus isolates in Singapore.J Clin Microbiol. 2006;44:1090-3. Sergio DM, Koh TH, Hsu LY, et al. Investigation of meticillin-resistant Staphylococcus aureus in pigs used for research.J Med Microbiol. 2007;56:Pt 81107-9. Philomin L. Hospitals step up measures to curb 'superbug'that spreads via touch. TODAY 2015 Nov 1. Available at: https://www.todayonline.com/singapore/hospitals-step-measures-curb-superbug-spreads-touch. Accessed October 23, 2018. Chlebicki MP, Kurup A.Vancomycin-resistant enterococcus:a review from a Singapore perspective.Ann Acad Med Singapore. 2008;37:861-9. Cai Y, Chan JP, Fisher DA, et al. Vancomycin-resistant Enterococci in Singaporean hospitals:5-year results of a multi-centre surveillance programme.Ann Acad Med Singapore. 2012;41:77-81. Chow A, Win NN, Ng PY, Lee W, Win MK.Vancomycin-resistant enterococci with reduced daptomycin susceptibility in Singapore:prevalence and associated factors.Epidemiol Infect. 2016;144:2540-5. Tan D, Htun HL, Koh J, et al. Comparative epidemiology of vancomycin-resistant enterococci colonization in an acute-care hospital and its affiliated intermediate- and long-term care facilities in Singapore.Antimicrob Agents Chemother. 2018;62:e01507-18. Hsu LY, Tan TY, Tam VH, et al. Network for Antimicrobial Resistance Surveillance (Singapore)Surveillance and correlation of antibiotic prescription and resistance of Gram-negative bacteria in Singaporean hospitals.Antimicrob Agents Chemother. 2010;54:1173-8. Teo J, Tan TY, Hon PY, et al. Network for Antimicrobial Resistance Surveillance (Singapore)ST22 and ST239 MRSA duopoly in Singaporean hospitals 2006-2010.Epidemiol Infect. 2013;141:153-7. Liew YX, Krishnan P, Yeo CL.Surveillance Singapore Network for Antimicrobial ResistanceSurveillance of broad-spectrum antibiotic prescription in Singaporean hospitals:a 5-year longitudinal study.PLoS One. 2011;6:e28751. Hartantyo SHP, Chau ML, Fillon L, et al. Sick pets as potential reservoirs of antibiotic-resistant bacteria in Singapore.Antimicrob Resist Infect Control. 2018;7:106. Chau ML, Chen SL, Yap M, et al. Group B streptococcus infections caused by improper sourcing and handling of fish for raw consumption, Singapore, 2015-2016.Emerg Infect Dis. 2017;23:1982-90. Hio L.$83m boost to help S'pore tackle challenges.The Straits Times 2017 Dec 2. Available at: https://www.straitstimes.com/singapore/83m-boost-to-help-spore-tackle-challenges. Accessed October 1, 2018. Singapore-MIT Alliance for Research and TechnologyAntimicrobial resistance interdisciplinary research group. Available at: https://smart.mit.edu/research/amr/about-amr. Accessed October 1, 2018. Saw Swee Hock School of Public HealthCollaborative solutions targeting antimicrobial resistance threats in the health system (CoSTAR-HS). Available at: https://sph.nus.edu.sg/research/costar-hs/. Accessed July 3, 2019. Lim EJ, Ho SX, Cao DY, et al. Extended-spectrum beta-lactamase-producing Enterobacteriaceae in retail chicken meat in Singapore.Ann Acad Med Singapore. 2016;45:557-9. Founou RC, Founou LL, Essack SY.Clinical and economic impact of antibiotic resistance in developing countries:a systematic review and meta-analysis.PLoS One. 2017;12:e0189621. Pan DS, Huang JH, Lee MH, et al. Knowledge, attitudes and practices towards antibiotic use in upper respiratory tract infections among patients seeking primary health care in Singapore.BMC Fam Pract. 2016;17:148. Tan Tock Seng HospitalSingapore antimicrobial stewardship training course. 2017;. Available at: https://www.ttsh.com.sg/page.aspx?id=11478. Accessed October 5, 2018. Chua AQ, Tang SSL, Lee LW, et al. Psychosocial determinants of physician acceptance toward an antimicrobial stewardship program and its computerized decision support system in an acute care tertiary hospital.J Am Coll Clin Pharm. 2018;1:e1-e8. Liew YX, Lee W, Loh JC, et al. Impact of an antimicrobial stewardship programme on patient safety in Singapore General Hospital.Int J Antimicrob Agents. 2012;40:55-60. Loo LW, Liew YX, Lee W, Chlebicki P, Kwa AL.Impact of antimicrobial stewardship program (ASP) on outcomes in patients with acute bacterial skin and skin structure infections (ABSSSIs) in an acute-tertiary care hospital.Infect Dis Ther. 2015;4:Suppl 115-25. Cai Y, Shek PY, Teo I, et al. A multidisciplinary antimicrobial stewardship programme safely decreases the duration of broad-spectrum antibiotic prescription in Singaporean adult renal patients.Int J Antimicrob Agents. 2016;47:91-6. Teng CB, Ng TM, Tan MW, et al. Safety and effectiveness of improving carbapenem use via prospective review and feedback in a multidisciplinary antimicrobial stewardship programme.Ann Acad Med Singapore. 2015;44:19-25. Seah XF, Ong YL, Tan SW, et al. Impact of an antimicrobial stewardship program on the use of carbapenems in a tertiary women's and children's hospital, Singapore.Pharmacotherapy. 2014;34:1141-50. Hsu LY. The campaign for global antibiotic awareness. TODAY 2016 Nov 7. Available at: https://www.todayonline.com/daily-focus/health/campaign-global-antibiotic-awareness. Accessed October 5, 2018. Choy CY, Hsu LY.World antibiotic awareness week.Ann Acad Med Singapore. 2017;46:413-4. Health Promotion Board.Fight the spread of infectious diseases. Available at: https://www.healthhub.sg/programmes/52/Fight_The_Spread. Accessed October 5, 2018. Hsu LY.Doctors here too eager to prescribe antibiotics.The New Paper 2018 Oct 2. Available at: https://www.tnp.sg/news/singapore/doctors-here-too-eager-prescribe-antibiotics. Accessed October 5, 2018. Khalik S.Hospital patients at risk of catching an infection.The Straits Times 2018 Oct 2. Available at: https://www.straitstimes.com/singapore/hospital-patients-at-risk-of-catching-an-infection. Accessed October 5, 2018. Cai Y, Venkatachalam I, Tee NW, et al. Prevalence of healthcare-associated infections and antimicrobial use among adult inpatients in Singapore acute-care hospitals:results from the first national point prevalence survey.Clin Infect Dis. 2017;64:suppl_2S61-S67. Ministry of Health SingaporeMOH establishes national adult immunisation schedule;extends use of medisave for vaccines under the schedule. 21 Oct 2017. Available at: https://www.moh.gov.sg/news-highlights/details/moh-establishes-national-adult-immunisation-schedule-extends-use-of-medisave-for-vaccines-under-the-schedule. Accessed February 9, 2019. Ministry of Health SingaporeThe national infection prevention and control guidelines for acute healthcare facilities 2017. Available at: https://www.moh.gov.sg/docs/librariesprovider5/resources-statistics/guidelines/national-infection-prevention-and-control-guidelines-for-acute-healthcare-facilities---2017.pdf. Accessed February 9, 2019. Versporten A, Zarb P, Caniaux I, et al. Global-PPS networkAntimicrobial consumption and resistance in adult hospital inpatients in 53 countries:results of an internet-based global point prevalence survey.Lancet Glob Health. 2018;6:e619-e629. KK Women's and Children's HospitalCarbapenem appropriateness in KKH. Available at: https://www.kkh.com.sg/about-kkh/corporate-profile/carbapenem-appropriateness. Accessed November 4, 2018. Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program:guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America.Clin Infect Dis. 2016;62:e51-77. Teng CB, Lee W, Yeo CL, et al. Guidelines for antimicrobial stewardship training and practice.Ann Acad Med Singapore. 2012;41:29-34. Ng TM, Phang VY, Young B, et al. Clinical impact of non-antibiotic recommendations by a multi-disciplinary antimicrobial stewardship team.Int J Antimicrob Agents. 2017;50:166-70. Lew KY, Ng TM, Tan M, et al. Safety and clinical outcomes of carbapenem de-escalation as part of an antimicrobial stewardship programme in an ESBL-endemic setting.J Antimicrob Chemother. 2015;70:1219-25. Liew YX, Lee W, Kwa AL, Chlebicki MP.Cost effectiveness of an antimicrobial stewardship programme.Int J Antimicrob Agents. 2015;46:594-5. Chow AL, Ang A, Chow CZ, et al. Implementation hurdles of an interactive, integrated, point-of-care computerised decision support system for hospital antibiotic prescription.Int J Antimicrob Agents. 2016;47:132-9. Chow A, Lye DC, Arah OA.Psychosocial determinants of physicians'acceptance of recommendations by antibiotic computerised decision support systems:a mixed methods study.Int J Antimicrob Agents. 2015;45:295-304. Baker JA.Experienced public healthcare sector pharmacists, nurses to be allowed to prescribe medicines from July.Channel NewsAsia 2018 Mar 7. Available at: https://www.channelnewsasia.com/news/singapore/experienced-public-healthcare-sector-pharmacists-nurses-to-be-10021468. Accessed November 4, 2018. IHiSNational Electronic Health Record (NEHR). Available at: https://www.ihis.com.sg/nehr/about-nehr. Accessed November 4, 2018. Beaudoin M, Kabanza F, Nault V, Valiquette L.Evaluation of a machine learning capability for a clinical decision support system to enhance antimicrobial stewardship programs.Artif Intell Med. 2016;68:29-36. Sethi T, Maheshwari S, Nagori A, Lodha R.Stewarding antibiotic stewardship in intensive care units with Bayesian artificial intelligence.Wellcome Open Res. 2018;3:73.
5. Hsu LY, Kwa AL, Lye DC, et al. Reducing antimicrobial resistance through appropriate antibiotic usage in Singapore. Singapore Med J 2008; 49:749-55.
7. Agri-Food & Veterinary Authority of Singapore, Ministry of Health, National Environment Agency, National Water Agency. The national strategic action plan on antimicrobial resistance, Singapore. 2017. Available at: https://www.moh.gov.sg/docs/librariesprovider5/resources-statistics/repo.... Accessed September 16, 2018.
10. World Health Organization. Global database for antimicrobial resistance country self assessment. Available at: https://amrcountryprogress.org. Accessed September 16, 2018.
11. Vasoo S, Barreto JN, Tosh PK. Emerging issues in gram-negative bacterial resistance: an update for the practicing clinician. Mayo Clin Proc 2015; 90:395‑403. https://doi.org/10.1016/j.mayocp.2014.12.002
PMid:25744116
12. McDanel J, Schweizer M, Crabb V, et al. Incidence of extended-spectrum β-lactamase (ESBL)-producing Escherichia coli and Klebsiella infections in the United States: a systematic literature review. Infect Control Hosp Epidemiol 2017; 38:1209-15. https://doi.org/10.1017/ice.2017.156
PMid:28758612
13. Karanika S, Karantanos T, Arvanitis M, Grigoras C, Mylonakis E. Fecal colonization with extended-spectrum beta-lactamase-producing Enterobacteriaceae and risk factors among healthy individuals: a systematic review and metaanalysis. Clin Infect Dis 2016; 63:310-8. https://doi.org/10.1093/cid/ciw283
PMid:27143671
14. Hawkey PM. Multidrug-resistant Gram-negative bacteria: a product of globalization. J Hosp Infect 2015; 89:241-7. https://doi.org/10.1016/j.jhin.2015.01.008
PMid:25737092
15. Hsu LY, Apisarnthanarak A, Khan E, et al. Carbapenem-resistant Acinetobacter baumannii and Enterobacteriaceae in South and Southeast Asia. Clin Microbiol Rev 2017; 30:1-22. https://doi.org/10.1128/CMR.00042-16
PMid:27795305 PMCid:PMC5217790
16. Liu YY, Wang Y, Walsh TR, et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis 2016; 16:161‑8.
17. Wang R, van Dorp L, Shaw LP, et al. The global distribution and spread of the mobilized colistin resistance gene MCR-1. Nat Commun 2018; 9:1179. https://doi.org/10.1038/s41467-018-03205-z
PMid:29563494 PMCid:PMC5862964
18. Lakhundi S, Zhang K. Methicillin-resistant Staphylococcus aureus: molecular characterization, evolution, and epidemiology. Clin Microbiol Rev 2018; 31:e00020-18. https://doi.org/10.1128/CMR.00020-18
PMid:30209034
19. Otter JA, French GL. Nosocomial transmission of community-associated methicillin-resistant Staphylococcus aureus: an emerging threat. Lancet Infect Dis 2006; 6:753-5. https://doi.org/10.1016/S1473-3099(06)70636-3
20. Okpara EO, Ojo OE, Awoyomi OJ, et al. Antimicrobial usage and presence of extended-spectrum β-lactamase-producing Enterobacteriaceae in animal-rearing households of selected rural and peri-urban communities. Vet Microbiol 2018; 218:31-9. https://doi.org/10.1016/j.vetmic.2018.03.013
PMid:29685218
22. Graveland H, Duim B, van Duijkeren E, Heederik D, Wagenaar JA. Livestock-associated methicillin-resistant Staphylococcus aureus in animals and humans. Int J Med Microbiol 2011; 301:630-4. https://doi.org/10.1016/j.ijmm.2011.09.004
PMid:21983338
23. Inglis TJ, Kumarasinghe G, Chow C, Liew HY. Multiple antibiotic resistance in Klebsiella spp. and other Enterobacteriaceae isolated in Singapore. Singapore Med J 1994; 35:602-4.
24. Koh TH. Gram-negative resistance in Singapore: a historical perspective. Ann Acad Med Singapore 2008; 37:847-54.
25. Tan TY, Hsu LY, Koh TH, et al. Antibiotic resistance in gram-negative bacilli: a Singapore perspective. Ann Acad Med Singapore 2008; 37:819-25.
26. Young BE, Lye DC, Krishnan P, Chan SP, Leo YS. A prospective observational study of the prevalence and risk factors for colonization by antibiotic resistant bacteria in patients at admission to hospital in Singapore. BMC Infect Dis 2014; 14:298. https://doi.org/10.1186/1471-2334-14-298
PMid:24889720 PMCid:PMC4057577
27. Teo J, Ngan G, Balm M, et al. Molecular characterization of NDM-1 producing Enterobacteriaceae isolates in Singapore hospitals. Western Pac Surveill Response J 2012; 3:19-24. https://doi.org/10.5365/wpsar.2011.2.4.010
PMid:23908903 PMCid:PMC3729072
28. Balm MN, Ngan G, Jureen R, Lin RT, Teo JW. OXA-181-producing Klebsiella pneumoniae establishing in Singapore. BMC Infect Dis 2013; 13:58. https://doi.org/10.1186/1471-2334-13-58
PMid:23374756 PMCid:PMC3570352
29. Teo JQ, Cai Y, Lim TP, Tan TT, Kwa AL. Carbapenem resistance in Gram-negative bacteria: the not-so-little problem in the little red dot. Microorganisms 2016; 4:E13. https://doi.org/10.3390/microorganisms4010013
PMid:27681907 PMCid:PMC5029518
30. Teo JW, Tan P, La MV, et al. Surveillance trends of carbapenem-resistant Enterobacteriaceae from Singapore, 2010-2013. J Glob Antimicrob Resist 2014; 2:99-102. https://doi.org/10.1016/j.jgar.2013.11.003
PMid:27873598
31. Marimuthu K, Venkatachalam I, Khong WX, et al; Carbapenemase-Producing Enterobacteriaceae in Singapore (CaPES) Study Group. Clinical and molecular epidemiology of carbapenem-resistant Enterobacteriaceae among adult inpatients in Singapore. Clin Infect Dis 2017; 64(suppl_2):S68-S75.
32. Esuvaranathan K, Kuan YF, Kumarasinghe G, Bassett DC, Rauff A. A study of 245 infected surgical wounds in Singapore. J Hosp Infect 1992; 21:231-40. https://doi.org/10.1016/0195-6701(92)90080-6
33. Hsu LY, Tan TY, Jureen R, et al. Antimicrobial drug resistance in Singapore hospitals. Emerg Infect Dis 2007; 13:1944-7. https://doi.org/10.3201/eid1312.070299
PMid:18258055 PMCid:PMC2876746
34. Chow A, Lim VW, Khan A, et al. MRSA transmission dynamics among interconnected acute, intermediate-term, and long-term healthcare facilities in Singapore. Clin Infect Dis 2017; 64(suppl_2):S76-S81. https://doi.org/10.1093/cid/cix072
PMid:28475785 PMCid:PMC5849126
35. Aung KT, Hsu LY, Koh TH, et al. Prevalence of methicillin-resistant Staphylococcus aureus (MRSA) in retail food in Singapore. Antimicrob Resist Infect Control 2017; 6:94. https://doi.org/10.1186/s13756-017-0255-3
PMid:28904790 PMCid:PMC5591520
36. Hsu LY, Koh YL, Chlebicka NL, et al. Establishment of ST30 as the predominant clonal type among community-associated methicillin-resistant Staphylococcus aureus isolates in Singapore. J Clin Microbiol 2006; 44:1090-3. https://doi.org/10.1128/JCM.44.3.1090-1093.2006
PMid:16517901 PMCid:PMC1393129
37. Sergio DM, Koh TH, Hsu LY, et al. Investigation of meticillin-resistant Staphylococcus aureus in pigs used for research. J Med Microbiol 2007; 56(Pt 8):1107-9. https://doi.org/10.1099/jmm.0.47283-0
PMid:17644720
39. Chlebicki MP, Kurup A. Vancomycin-resistant enterococcus: a review from a Singapore perspective. Ann Acad Med Singapore 2008; 37:861-9.
40. Cai Y, Chan JP, Fisher DA, et al. Vancomycin-resistant Enterococci in Singaporean hospitals: 5-year results of a multi-centre surveillance programme. Ann Acad Med Singapore 2012; 41:77-81.
41. Chow A, Win NN, Ng PY, Lee W, Win MK. Vancomycin-resistant enterococci with reduced daptomycin susceptibility in Singapore: prevalence and associated factors. Epidemiol Infect 2016; 144:2540-5. https://doi.org/10.1017/S0950268816000923
PMid:27174845
42. Tan D, Htun HL, Koh J, et al. Comparative epidemiology of vancomycin-resistant enterococci colonization in an acute-care hospital and its affiliated intermediate- and long-term care facilities in Singapore. Antimicrob Agents Chemother 2018; 62:e01507-18. https://doi.org/10.1128/AAC.01507-18
PMid:30224534 PMCid:PMC6256803
43. Hsu LY, Tan TY, Tam VH, et al; Network for Antimicrobial Resistance Surveillance (Singapore). Surveillance and correlation of antibiotic prescription and resistance of Gram-negative bacteria in Singaporean hospitals. Antimicrob Agents Chemother 2010; 54:1173-8. https://doi.org/10.1128/AAC.01076-09
PMid:20065055 PMCid:PMC2826017
44. Teo J, Tan TY, Hon PY, et al; Network for Antimicrobial Resistance Surveillance (Singapore). ST22 and ST239 MRSA duopoly in Singaporean hospitals: 2006-2010. Epidemiol Infect 2013; 141:153-7. https://doi.org/10.1017/S0950268812000337
PMid:22394568
45. Liew YX, Krishnan P, Yeo CL, et al; Network for Antimicrobial Resistance Surveillance Singapore. Surveillance of broad-spectrum antibiotic prescription in Singaporean hospitals: a 5-year longitudinal study. PLoS One 2011; 6:e28751. https://doi.org/10.1371/journal.pone.0028751
PMid:22174889 PMCid:PMC3235163
46. Hartantyo SHP, Chau ML, Fillon L, et al. Sick pets as potential reservoirs of antibiotic-resistant bacteria in Singapore. Antimicrob Resist Infect Control 2018; 7:106. https://doi.org/10.1186/s13756-018-0399-9
PMid:30186596 PMCid:PMC6117887
47. Chau ML, Chen SL, Yap M, et al. Group B streptococcus infections caused by improper sourcing and handling of fish for raw consumption, Singapore, 2015-2016. Emerg Infect Dis 2017; 23:1982-90. https://doi.org/10.3201/eid2312.170596
PMid:29148967 PMCid:PMC5708258
49. Singapore-MIT Alliance for Research and Technology. Antimicrobial resistance interdisciplinary research group. Available at: https://smart.mit.edu/research/amr/about-amr. Accessed October 1, 2018.
50. Saw Swee Hock School of Public Health. Collaborative solutions targeting antimicrobial resistance threats in the health system (CoSTAR-HS). Available at: https://sph.nus.edu.sg/research/costar-hs/. Accessed July 3, 2019.
51. Lim EJ, Ho SX, Cao DY, et al. Extended-spectrum beta-lactamase-producing Enterobacteriaceae in retail chicken meat in Singapore. Ann Acad Med Singapore 2016; 45:557-9.
52. Founou RC, Founou LL, Essack SY. Clinical and economic impact of antibiotic resistance in developing countries: a systematic review and meta-analysis. PLoS One 2017; 12:e0189621. https://doi.org/10.1371/journal.pone.0189621
PMid:29267306 PMCid:PMC5739407
53. Pan DS, Huang JH, Lee MH, et al. Knowledge, attitudes and practices towards antibiotic use in upper respiratory tract infections among patients seeking primary health care in Singapore. BMC Fam Pract 2016; 17:148. https://doi.org/10.1186/s12875-016-0547-3
PMid:27809770 PMCid:PMC5094024
54. Tan Tock Seng Hospital. Singapore antimicrobial stewardship training course. 2017. Available at: https://www.ttsh.com.sg/page.aspx?id=11478. Accessed October 5, 2018.
55. Chua AQ, Tang SSL, Lee LW, et al. Psychosocial determinants of physician acceptance toward an antimicrobial stewardship program and its computerized decision support system in an acute care tertiary hospital. J Am Coll Clin Pharm 2018; 1:e1-e8. https://doi.org/10.1002/jac5.1028
56. Liew YX, Lee W, Loh JC, et al. Impact of an antimicrobial stewardship programme on patient safety in Singapore General Hospital. Int J Antimicrob Agents 2012; 40:55-60. https://doi.org/10.1016/j.ijantimicag.2012.03.004
PMid:22591837
57. Loo LW, Liew YX, Lee W, Chlebicki P, Kwa AL. Impact of antimicrobial stewardship program (ASP) on outcomes in patients with acute bacterial skin and skin structure infections (ABSSSIs) in an acute-tertiary care hospital. Infect Dis Ther 2015; 4(Suppl 1):15-25. https://doi.org/10.1007/s40121-015-0085-7
PMid:26362296 PMCid:PMC4569641
58. Cai Y, Shek PY, Teo I, et al. A multidisciplinary antimicrobial stewardship programme safely decreases the duration of broad-spectrum antibiotic prescription in Singaporean adult renal patients. Int J Antimicrob Agents 2016; 47:91-6. https://doi.org/10.1016/j.ijantimicag.2015.10.021
PMid:26706421
59. Teng CB, Ng TM, Tan MW, et al. Safety and effectiveness of improving carbapenem use via prospective review and feedback in a multidisciplinary antimicrobial stewardship programme. Ann Acad Med Singapore 2015; 44:19‑25.
60. Seah XF, Ong YL, Tan SW, et al. Impact of an antimicrobial stewardship program on the use of carbapenems in a tertiary women's and children's hospital, Singapore. Pharmacotherapy 2014; 34:1141-50. https://doi.org/10.1002/phar.1490
PMid:25283969
66. Cai Y, Venkatachalam I, Tee NW, et al. Prevalence of healthcare-associated infections and antimicrobial use among adult inpatients in Singapore acute-care hospitals: results from the first national point prevalence survey. Clin Infect Dis 2017; 64(suppl_2):S61-S67. https://doi.org/10.1093/cid/cix103
PMid:28475790
69. Versporten A, Zarb P, Caniaux I, et al; Global-PPS network. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: results of an internet-based global point prevalence survey. Lancet Glob Health 2018; 6:e619-e629.
71. Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis 2016; 62:e51‑77. https://doi.org/10.1093/cid/ciw118
PMid:27080992 PMCid:PMC5006285
72. Teng CB, Lee W, Yeo CL, et al. Guidelines for antimicrobial stewardship training and practice. Ann Acad Med Singapore 2012; 41:29-34.
73. Ng TM, Phang VY, Young B, et al. Clinical impact of non-antibiotic recommendations by a multi-disciplinary antimicrobial stewardship team. Int J Antimicrob Agents 2017; 50:166-70. https://doi.org/10.1016/j.ijantimicag.2017.01.046
PMid:28625717
74. Lew KY, Ng TM, Tan M, et al. Safety and clinical outcomes of carbapenem de-escalation as part of an antimicrobial stewardship programme in an ESBL-endemic setting. J Antimicrob Chemother 2015; 70:1219-25. https://doi.org/10.1093/jac/dku479
75. Liew YX, Lee W, Kwa AL, Chlebicki MP. Cost effectiveness of an antimicrobial stewardship programme. Int J Antimicrob Agents 2015; 46:594-5. https://doi.org/10.1016/j.ijantimicag.2015.08.008
PMid:26493229
76. Chow AL, Ang A, Chow CZ, et al. Implementation hurdles of an interactive, integrated, point-of-care computerised decision support system for hospital antibiotic prescription. Int J Antimicrob Agents 2016; 47:132-9. https://doi.org/10.1016/j.ijantimicag.2015.12.006
PMid:26774157
77. Chow A, Lye DC, Arah OA. Psychosocial determinants of physicians' acceptance of recommendations by antibiotic computerised decision support systems: a mixed methods study. Int J Antimicrob Agents 2015; 45:295-304. https://doi.org/10.1016/j.ijantimicag.2014.10.009
PMid:25434998
80. Beaudoin M, Kabanza F, Nault V, Valiquette L. Evaluation of a machine learning capability for a clinical decision support system to enhance antimicrobial stewardship programs. Artif Intell Med 2016; 68:29-36. https://doi.org/10.1016/j.artmed.2016.02.001
PMid:26947174
81. Sethi T, Maheshwari S, Nagori A, Lodha R. Stewarding antibiotic stewardship in intensive care units with Bayesian artificial intelligence. Wellcome Open Res 2018; 3:73. https://doi.org/10.12688/wellcomeopenres.14629.1