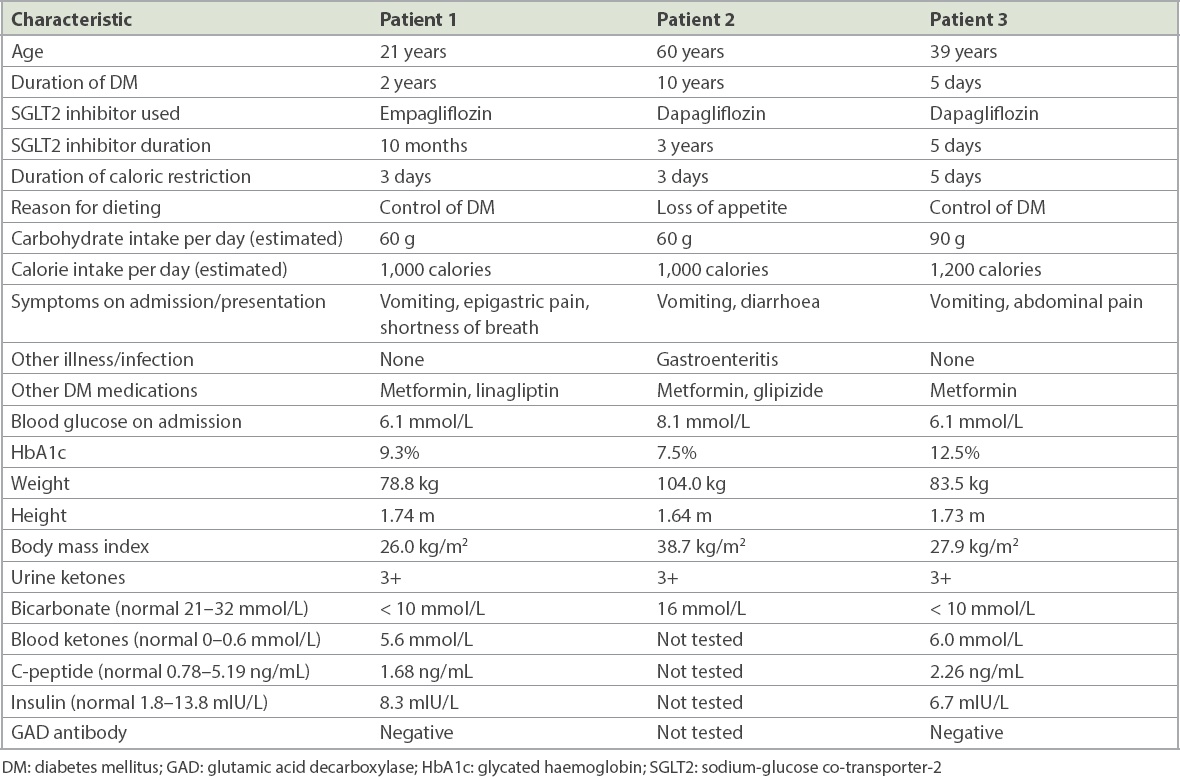
Between December 2018 and February 2020, three cases of euglycaemic diabetic ketoacidosis (EuDKA) were seen in my practice (Table I). All three had Type 2 diabetes mellitus (DM). All cases involved the use of sodium-glucose co-transporter-2 (SGLT2) inhibitors and a short period of calorie restriction a few days prior to admission to hospital. The three patients varied in age (21–60 years), duration of DM (5 days–10 years) and duration of use of SGLT2 inhibitors (5 days–3 years). None were on insulin. The calorie restriction was deliberate in two patients, who were attempting to quickly control their DM, and partially involuntary in the third, who had gastroenteritis. All developed ketoacidosis within five days of their change in diet.
Table I
Patient characteristics and clinical presentation.
The entity of EuDKA was first reported in 1973.(1) Reports of ketoacidosis in relation to the use of SGLT2 inhibitors began to appear in 2015.(2) Significantly, some occurred in patients with Type 2 DM. Ketoacidosis has been reported in patients without DM and those who were not using SGLT2 inhibitors. For instance, Shah and Isley reported that a 51-year-old woman without DM developed four episodes of ketoacidosis while on a ‘no carbohydrate’ diet (over a period of four years) with a carbohydrate intake that was estimated to be as low as 20 g per day.(3)
Our patients were estimated to have taken about 60–90 g of carbohydrate each day and had a calorie intake of only 1,000–1,200 calories per day. They developed ketoacidosis after 3–5 days of dieting. It is likely that the suddenness of the diet as well as the insufficient calorie and carbohydrate intake contributed to the development of EuDKA in these three patients. Patients 1 and 3 had normal C-peptide and insulin levels during admission. However, very low carbohydrate intake can lead to reduction in insulin release and the relative insulinopenia could contribute to EuDKA. In Patient 2, gastroenteritis causing dehydration could be a contributing factor.
Hamblin et al reported that SGLT2 inhibitor usage increases the risk of EuDKA developing during hospital admissions.(4) More users (with Type 2 DM) developed EuDKA, as an inpatient, as compared to non-users of SGLT2 inhibitors (14 cases vs. two cases). In the United Kingdom, it is advised that patients pause the use of SGLT2 inhibitors when they are hospitalised for surgery or acute illnesses; treatment with SGLT2 inhibitors may be restarted once their condition has stabilised.(5) The Australian and New Zealand College of Anaesthetists recommends that SGLT2 inhibitors be stopped up to three days preoperatively (two days prior to and on the day of surgery) or in other physically stressful situations.(6)
We should be mindful that patients on SGLT2 inhibitors may develop EuDKA in situations where calorie intake is temporarily curtailed. With low carbohydrate diets, ketogenic diets, intermittent fasting and other forms of calorie restriction becoming more popular, we may begin to see the entity of EuDKA more often.
References Munro JF, Campbell IW, McCuish AC, Duncan LJP.Euglycaemic diabetic ketoacidosis.Br Med J. 1973;2:578-80. Peters AL, Buschur EO, Buse JB, et al. Euglycaemic diabetic ketoacidosis:a potential complication of treatment with sodium-glucose cotransporter 2 inhibition.Diabetes Care. 2015;38:1687-93. Shah P, Isley WL.Ketoacidosis dang a low-carbohydrate diet.N Engl J Med. 2006;354:97-8. Hamblin PS, Wong R, Ekinci EI, et al. SGLT2 inhibitors increase the risk of diabetic ketoacidosis developing in the community and dang hospital admission.J Clin Endocrinol Metab. 2019;104:3077-87. UK Medicines and Healthcare Products Regulatory AgencySGLT2 inhibitors:updated advice on the risk of diabetic ketoacidosis. Available at: https://www.gov.uk/drug-safety-update/sglt2-inhibitors-updated-advice-on-the-risk-of-diabetic-ketoacidosis. Accessed February 26, 2020. Australian and New Zealand College of AnaesthetistsAlert:Severe euglycaemic ketoacidosis with SGLT2 inhibitor use in the perioperative period. Available at: https://www.anzca.edu.au/documents/alert-dka-and-oral-hypoglycaemics-20180215.pdf. Accessed February 26, 2020.
2. Peters AL, Buschur EO, Buse JB, et al. Euglycaemic diabetic ketoacidosis: a potential complication of treatment with sodium-glucose cotransporter 2 inhibition. Diabetes Care 2015; 38:1687-93. https://doi.org/10.2337/dc15-0843
PMid:26078479 PMCid:PMC4542270
3. Shah P, Isley WL. Ketoacidosis during a low-carbohydrate diet. N Engl J Med 2006; 354:97-8. https://doi.org/10.1056/NEJMc052709
PMid:16394313
4. Hamblin PS, Wong R, Ekinci EI, et al. SGLT2 inhibitors increase the risk of diabetic ketoacidosis developing in the community and during hospital admission. J Clin Endocrinol Metab 2019; 104:3077-87. https://doi.org/10.1210/jc.2019-00139
PMid:30835263