

Dear Sir,
Transcatheter aortic valve implantation (TAVI) or transcatheter aortic valve replacement (TAVR) has become a treatment option for patients with severe aortic valve stenosis.(1) Transcatheter aortic valve-in-valve replacement for degenerated surgical aortic bioprostheses has also become an established, less invasive alternative to redo open aortic valve replacement.(2) Transcatheter tricuspid valve-in-valve (TV ViV) replacement has been employed in much smaller numbers in degenerated tricuspid bioprostheses.(3) We herein report the initial experience in Southeast Asia of a percutaneous transvenous transcatheter tricuspid valve replacement of a failed surgical tricuspid bioprosthesis with three-year follow-up.
A 64-year-old man was referred to our institution for increasing exertional dyspnoea (New York Heart Association [NYHA] Class III), abdominal distension and lower limb oedema for the past 2–3 months. Past medical history included hypertension, single vessel coronary angioplasty and stenting, atrial flutter on warfarin, Child-Pugh Class B liver cirrhosis and rheumatic heart disease with aortic valve replacement (23-mm Mitroflow bioprosthesis [Sorin Group, Milan, Italy]), mitral valve annuloplasty (28-mm Sorin ring [Sorin Group]), and a tricuspid valve replacement (31-mm Pericarbon bioprosthesis [Sorin Group]) 6.5 years prior to the current presentation.
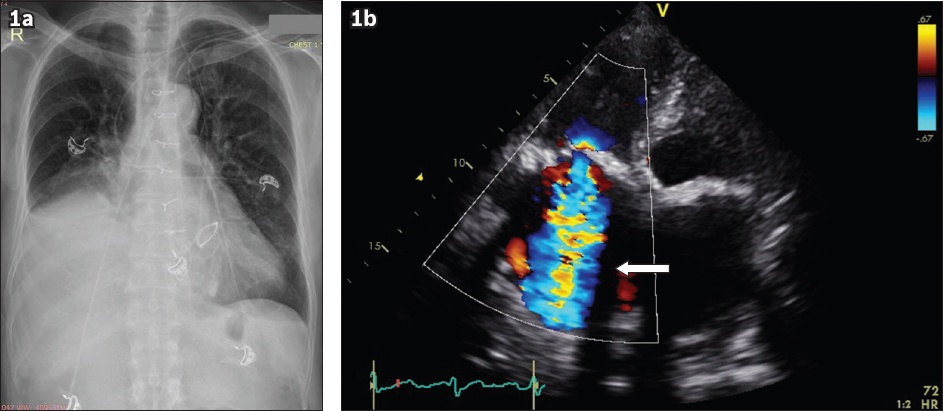
Chest radiography revealed a large right pleural effusion (
Fig. 1
(a) Chest radiograph shows a large right pleural effusion. (b) Echocardiographic image shows severe tricuspid regurgitation with torrential regurgitant colour jet (white arrow).
Due to the patient’s elevated surgical risk (poor general condition, liver cirrhosis, dilated right heart immediately adjacent to the sternum and previous open heart surgery), non-surgical options were explored. The novel technique of percutaneous transcatheter TV ViV replacement was offered, and informed consent was obtained from the patient and his family.
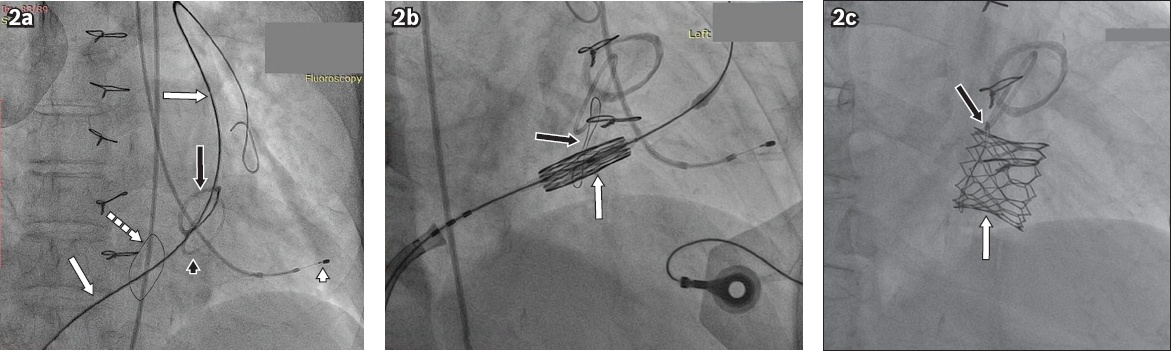
The procedure was performed in the hybrid operating room under local anaesthesia and conscious sedation. A pacing wire was advanced via the left femoral artery to the left ventricular apex. A 16-French expandable sheath was placed in the right femoral vein and a stiff wire was placed across the degenerated tricuspid bioprosthesis into the left pulmonary artery (
Fig. 2
Fluoroscopic images show (a) the stiff wire (white arrows) from the femoral vein crossing the Pericarbon tricuspid bioprosthesis (dashed arrow) into the left pulmonary artery; the pacing wire (white arrowhead) is positioned at the left ventricular apex. The aortic bioprosthetic valve (black arrow) and the mitral bioprosthetic valve (black arrowhead) are shown; (b) the SAPIEN 3 transcatheter heart valve (white arrow) positioned within the Pericarbon tricuspid bioprosthetic valve (black arrow); and (c) the fully deployed SAPIEN 3 transcatheter heart valve (white arrow) within the failed tricuspid bioprosthesis (black arrow).
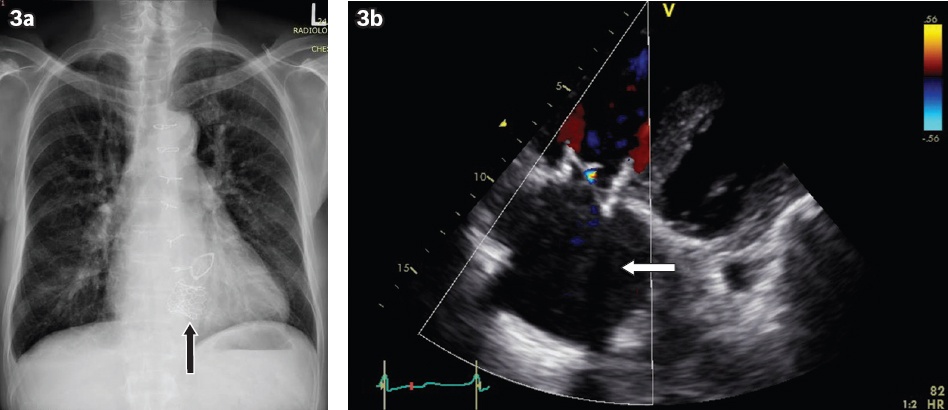
Recovery was uneventful and the patient was discharged two days after the procedure. The patient was well at 30 days and reported marked improvement in functional status (NYHA Class I–II) and resolution of the abdominal distension and lower limb oedema. His chest radiograph showed that the right pleural effusion had resolved (
Fig. 3
(a) Chest radiograph shows resolution of the right pleural effusion. The SAPIEN 3 transcatheter heart valve (arrow) can be seen. (b) Echocardiographic image at three years shows trivial tricuspid regurgitation with no regurgitant colour jet (white arrow).
TAVI has become an established therapeutic option for patients with severe aortic valve stenosis,(1) and transcatheter aortic valve-in-valve replacement is increasingly accepted as a less invasive and lower-risk treatment for patients with degenerated aortic bioprostheses.(2,4) Transcatheter TV ViV replacement for failed tricuspid bioprostheses is, however, less commonly performed due to the paucity of patients with previous surgical bioprosthetic tricuspid valve replacement. Several approaches are available: a direct transatrial approach or a transvenous approach via the femoral or internal jugular vein. The direct transatrial approach facilitates coaxial delivery of the transcatheter heart valve due to the proximity of the atriotomy to the tricuspid valve.(3,5) However, this approach requires a surgical thoracotomy and general anaesthesia, leading to a longer recovery period with elevated bleeding risk. A true percutaneous technique using a transvenous approach via the femoral vein or the internal jugular vein is thus more attractive due to its less invasive nature, reduced risk of major bleeding and a significantly shorter hospital stay. However, it requires more wire and catheter manipulations, and there is a theoretical risk of valve malposition, as the transcatheter heart valve would likely not be coaxial to the failed tricuspid bioprosthesis. Despite these limitations, multicentre registries have shown a high procedural success rate of 97%–98% and satisfactory short- to mid-term outcomes.(3,6)
We herein reported our initial experience of a percutaneous transfemoral TV ViV replacement in Southeast Asia using the Edwards Sapien 3 balloon-expandable valve with mid-term follow-up. An oversized Sapien 3 transcatheter heart valve was selected because the transcatheter heart valve must be larger than the previous bioprosthesis to anchor within it (true internal diameter of the 31-mm Pericarbon valve: 27 mm). An appropriately sized transcatheter heart valve also optimises haemodynamics and minimises the risk of paravalvular leak. Temporary rapid ventricular pacing (to stabilise the deployment of the Sapien valve during balloon inflation) could possibly be more reliable when performed through the coronary sinus. However, due to our lack of familiarity with this method, we chose to perform rapid pacing via the left ventricle. Our report has demonstrated that the transfemoral (transvenous) route for transcatheter TV ViV replacement is technically feasible with a successful procedure result. This is an attractive approach as compared to redo open chest surgery in a frail, high-risk patient and led to a rapid recovery with a short two-day hospital stay and a good clinical outcome with satisfactory valve function at three years.
Yours sincerely,